
Abstract
Background:
Transient hypothyroxinemia is common in extremely premature infants, but has not been extensively investigated in ill term and late preterm infants. We hypothesized that free thyroxine (T4) levels in term and late preterm infants with respiratory distress would be inversely related to severity of illness
Methods:
Eligible infants included those had ≥35 weeks of gestation requiring mechanical ventilation or nasal continuous positive airway pressure. Thyroid function (thyroid-stimulating hormone, T4, free T4 [fT4], and free triiodothyronine) and cortisol levels were collected at four specified intervals (birth, day 2, day 3, and day 5 of life). Illness severity was measured using score for neonatal acute physiology (SNAP). Infants with an SNAP ≥10 were considered to have severe illness. Statistical analysis included repeated measures analysis of variance.
Results:
A total of 20 patients were enrolled in the study. The mean gestational age of study infants was 37.0 ± 1.7 weeks. Infant with SNAP ≥10 had a diminished thyroid-stimulating hormone at birth. There was an inverse correlation between SNAP at birth and fT4. There was also an inverse correlation between lowest measured fT4 and highest mean airway pressure, oxygenation index, and A-a gradient. Infants who received inhaled nitric oxide had diminished fT4 levels compared to infants who did not receive this therapy. There were no differences in cortisol in those infants with and without SNAP ≥10 during the study period.
Conclusions:
In our study sample, there was an association between severity of illness and fT4 levels at birth, and infants requiring inhaled nitric oxide showed decreased fT4 over the study time. Further research is warranted to determine whether T4 supplementation would be beneficial in term and late preterm infants with respiratory distress.
Introduction
The primary goal of this study was to investigate the relationship between thyroid function, particularly fT4, and illness severity in term and late preterm infants with respiratory distress who require endotracheal intubation or nasal continuous positive airway pressure (N-CPAP). We hypothesized that fT4 levels in term and late preterm infants with respiratory distress would be inversely related to severity of illness, and that those infants who received rescue therapies, including iNO, would have lower fT4 compared to those infants not receiving these therapies.
Methods
This investigation was a prospective observational study of infants admitted to the neonatal intensive care unit (NICU) at Christiana Care Health Systems, Newark, Delaware. The NICU at Christiana Hospital is a Level III NICU caring for both inborn and outborn infants. The NICU at Christiana offers iNO and high-frequency ventilation but not ECMO. All infants in the study sample were admitted between January 31, 2006, and July 8, 2006. The Institutional Review Board of Christiana Care Health System approved the study. Informed written consent was obtained from parents of infants before study entry.
Consecutive infants were eligible for the study if they had ≥35 weeks of gestation and demonstrated respiratory distress requiring mechanical ventilation or N-CPAP in the first 24 hours of life (n = 20). In addition to term infants, infants ≥35 weeks who were included as late preterm infants are increasing in prevalence, often develop respiratory distress, and thyroid function has not been extensively studied in this population (11). The decision to initiate mechanical ventilation or N-CPAP was made by the medical team caring for the baby in conjunction with the attending neonatologist. Criteria for initiating N-CPAP included an oxygen saturation of <95% on a supplemental oxygen fraction ≥0.40, or a PCO2 >50 torr in the presence of labored breathing. Mechanical ventilation was initiated in those infants not responding to N-CPAP with an improvement in oxygen saturation or decrease in PCO2. Infants with any documented major congenital anomalies were excluded from the study. Gestational age was defined by the best obstetrical estimate or by modified Ballard exam if obstetrical dating was not available.
Illness severity was measured by score for neonatal acute physiology (SNAP) (12). SNAP evaluates the worst physiologic dysfunction of each organ system and is predictive of neonatal mortality, independent of diagnosis. SNAP was calculated from data on the day of birth and each subsequent day of life during the study period (days 1–5). SNAP, which is based on most severe physiologic measurements over a period of time, was therefore calculated every day and not limited to the more narrow time periods used for collection of hormone specimens. For the purposes of this study, severe illness at birth was considered an SNAP ≥10. The use of SNAP ≥10 as a cut-off for severe illness severity was based on our previous research on preterm infants (2). In that investigation SNAP ≥10 had the maximum sensitivity and specificity for predicting intraventricular hemorrhage, severe intraventricular hemorrhage, and mortality in preterm infants (2).
To quantify the degree of respiratory illness in each infant, oxygen index (OI), Alveolar-arterial gradient (A-a gradient), and ventilator mean airway pressure were recorded with each blood gas obtained during this study period. The highest OI, A-a gradient, and mean airway pressure measured during the study were recorded. OI was calculated in standard fashion using the following formula: mean airway pressure × ([FiO2/PaO2] × 100). In addition, use of medications to regulate blood pressure (i.e., Dopamine), use of pharmacologic paralysis, use of iNO, high-frequency ventilation, and ECMO were monitored. iNO therapy was initiated if the study patient demonstrated worsening respiratory failure, as documented by an OI ≥15. Infants were transferred to an ECMO center if they continued to have an OI >25, despite maximal ventilatory support and iNO. Actual use of ECMO was determined by the clinical team at the referral center.
Blood samples for thyroid function (TSH, T4, fT4, and free triiodothyronine [T3]) and cortisol levels were collected at four specified intervals. The first specimen was collected upon NICU admission between 0 and 24 hours and is designated as the “birth” specimen. The second specimen was collected at 48 hours of life and designated “day of life 2.” The third specimen was collected at 72 hours and designated “day of life 3.” The final specimen was collected at 120 hours of age and designated “day of life 5.” With the exception of the initial specimen at 0–24 hours, a window of 6 hours before and after each time interval allowed study labs to be timed with other routine labs and thus minimize discomfort to the patient. Because respiratory distress can manifest soon after birth, or at a later time after birth, the first specimen (birth) was obtained at the time of NICU admission and coordinated with routine admission labs. Precise timing (mean ± standard deviation) of the blood samples were as follows: the initial birth samples were obtained at a mean age of 18.8 ± 5.7 hours of life, the second day of life specimens were obtained at 46.6 ± 3.5 hours, the third day of life specimens at 72.8 ± 6.4 hours, and the fifth day of life specimens at 118.6 ± 4.7 hours of age.
Cortisol was obtained as previous studies have demonstrated that low cortisol levels in preterm infants are associated with an increased risk for chronic lung disease (13). In addition, obtaining cortisol levels allowed us to evaluate another hormone influencing metabolic rate and response to stress, and has previously been studied in preterm infants in relationship to thyroid function (14).
Total T4, free T3, TSH, fT4, and cortisol levels were measured using a competitive electro-chemiluminescent assay (E170; Roche, Basel, Switzerland) in the chemistry lab at Christiana Hospital. Within run precision coefficient of variation for the fT4 assay was 1.4–2.0% with a total precision of 2.6–4.8%. fT4 was assayed as a single sample from fresh serum immediately after collection.
All caretakers were masked to study laboratory results. The clinical laboratory running the thyroid function and cortisol were masked to the infant's clinical condition. Laboratory results were screened for any results that suggested a possibility of congenital hypothyroidism, as demonstrated by a TSH >25 mIU/mL, beyond 24 hours of age by a research nurse not caring for the study infants. Routine screening for congenital hypothyroidism by the State of Delaware Newborn Screening Program continued as per routine during the study time. No infants in the study sample were found to have congenital hypothyroidism, and no infants in the study sample received thyroid hormone supplementation.
The statistical relationship between hormone levels and illness severity was investigated in three ways. First, we investigated whether severe illness at birth, elevated over a predetermined level, SNAP ≥10, affected hormone levels over the first 5 days of life. This relationship between severe illness at birth and hormone levels was investigated using repeated measures two-way analysis of variance (ANOVA). Second, we investigated if there were any correlations between the continuous variables of SNAP on the day of birth and hormone levels on the day of birth. Third, we investigated whether peak illness severity during the study period, as measured by highest recorded daily SNAP, correlated with lowest measured hormone levels during the study period. Pearson's correlation was used in these analyses with data presented as r 2. Pearson's correlation was also used to analyze the relationships between hormone levels and maximum respiratory support. In addition, repeated measures two-way ANOVA was used to compare hormone levels over the first 5 days of life in infants who required iNO, mechanical ventilation, or pressor support compared to infants not requiring these interventions. One-way ANOVA, Chi-squared, and Mann–Whitney test were used to compare infants with and without severe illness. Power analysis indicated that 20 infants were required for the study to show a 50% difference in fT4 levels between those infants with severe illness at birth compared to those without severe illness with an α of 0.05 and a β of 0.80. Data are expressed as mean ± standard deviation. A p-value of <0.05 was considered significant. All statistical calculations were performed using Statistica 7.0 (Statsoft, Tulsa, OK).
Results
The mean gestational age of study infants was 37.0 ± 1.7 weeks, and birth weight was 2814 ± 583 g. In the study sample 5 infants received only N-CPAP and did not require mechanical ventilation, and 15 infants required mechanical ventilation, 4 infants required rescue high-frequency oscillatory ventilation, and 3 infants received iNO. All Cesarean sections were done electively as either a repeat section or due to failure of progression of labor. All infants in the study sample survived until hospital discharge; three infants were transferred to an ECMO center but did not require ECMO. None of the infants in the study sample received intravenous iodinated contrast.
There were no differences in birthweight, gestational age, maternal age, race, gender, and Apgar scores between those infants with and without SNAP ≥10 on the day of birth (Table 1). Those infants with SNAP ≥10 were more likely to receive exogenous surfactant, but there were no differences in duration of mechanical ventilation, maximum mean airway pressure, maximum OI, use of pressor support, iNO, or pharmacologic paralysis between groups.
Data are presented as mean ± standard deviation or percentage of patients.
SNAP, score for neonatal acute physiology.
In those infants with SNAP ≥10 at birth, TSH levels were lower compared to infants with SNAP <10, with the differences in hormone levels occurring on the day of birth (Table 2). Infants with SNAP ≥10 were admitted to the NICU earlier, and the first blood specimen was therefore obtained earlier (15.0 ± 4.1 vs. 21.6 ± 5.3 hours, p = 0.01) compared to infants without SNAP ≥10. However, TSH levels obtained at birth were not correlated with the hour of life which levels were obtained (r 2 = 0.01, p = 0.72). None of the infants in the study sample received dopamine or dobutamine infusions before obtaining the first blood specimen. There were no differences in TSH based on gestation (Table 2).
Hormone levels presented for all infants in study sample (n = 20). Comparison levels for those with SNAP ≥10 (n = 9) and those with SNAP <10 (n = 11), and those with gestation 35–36 weeks (n = 12) and those with gestation ≥37 weeks (n = 8). Data are presented as mean ± standard deviation. p-Values difference by SNAP and gestation over first 5 days of life.
There were no overall differences in fT4 levels over the first 5 days of life based on gestation or in infants with SNAP ≥10 compared to those with SNAP <10 (Table 2). However, highest daily SNAP was inversely correlated with the lowest fT4 over the first 120 hours of life (Fig. 1, r 2 = 0.60, p = 0.001). There was also an inverse correlation between SNAP on the day of birth and fT4 obtained at birth (r 2 = 0.28, p = 0.02). Lowest measured fT4 levels were inversely correlated with the highest mean airway pressure (r 2 = 0.45, p = 0.002), highest OI (r 2 = 0.54, p = 0.001), and highest A-a gradient (r 2 = 0.27, p = 0.04) over the study period. Gestational age was not correlated with admission fT4 (r 2 = 0.001, p = 1.0).
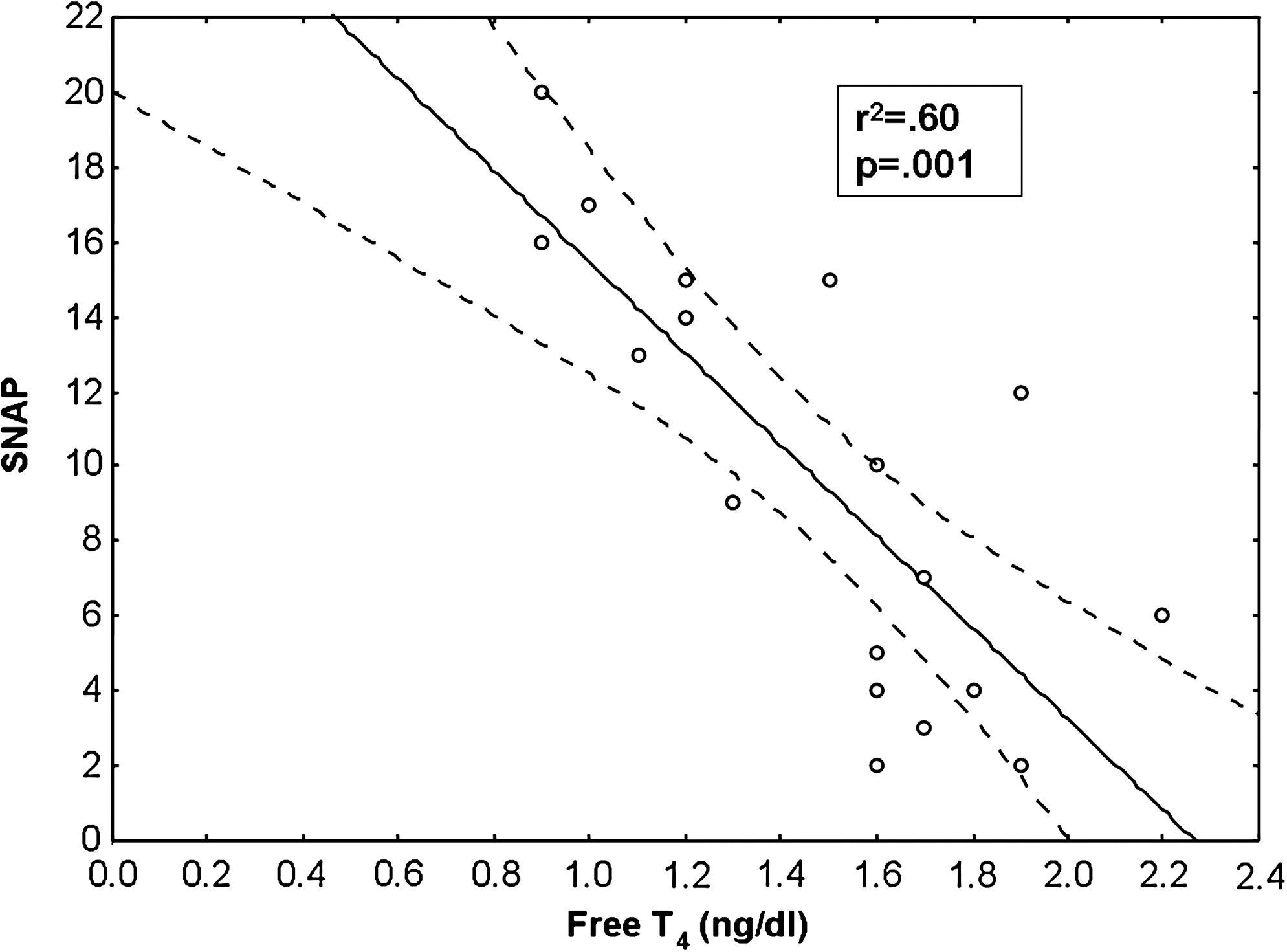
Correlation between lowest measured free thyroxine, and highest measured score for neonatal acute physiology during study period.
There were no overall differences in total T4 levels based on gestation, or in infants with SNAP ≥10 at birth compared to those with SNAP <10 (Table 2). Total T4 levels were not correlated with SNAP on the day of birth (r 2 = 0.13, p = 0.13), but highest daily SNAP was correlated with lowest measured total T4 (r 2 = 0.27, p = 0.02). There were no correlations between the lowest measured total T4 and highest mean airway pressure (r 2 = 0.12, p = 0.15), highest OI (r 2 = 0.13, p = 0.14), or highest A-a gradient (r 2 = 0.01, p = 0.63).
There were no differences in free T3 over the first 5 days of life based on gestation, or in infants with and without SNAP ≥10 at birth (Table 2). Free T3 on the day of birth was not correlated will illness severity (r 2 = 0.12, p = 0.14), but highest SNAP was correlated with lowest measured free T3 (r 2 = 0.23, p = 0.03). There were no correlations between lowest measured free T3 and highest mean airway pressure (r 2 = 0.07, p = 0.29), highest OI (r 2 = 0.10, p = 0.20), or highest A-a gradient (r 2 = 0.01, p = 0.72).
There were no differences in cortisol based on gestation (Table 2), or in infants with and without SNAP ≥10 over the first 5 days of life. Cortisol levels at birth were not correlated with SNAP on the day of birth (r 2 = 0.0001, p = 0.93). There were no correlations between lowest measured cortisol and highest mean airway pressure (r 2 = 0.10, p = 0.20), highest OI (r 2 = 0.13, p = 0.14), or highest A-a gradient (r 2 = 0.21, p = 0.06).
fT4 levels in those infants who received iNO were significantly lower compared to infants not receiving iNO, with the difference occurring at 5 days of age (Fig. 2). There were no differences in any of the hormone levels in those infants who received blood pressure support or pharmacologic paralysis compared to the infants not receiving these therapies (data not shown).

Relationship between free thyroxine, and time and use of inhaled nitric oxide (iNO). Solid line and circles represent those infants who required treatment with iNO (n = 3). The dotted line and squares represent those infants who did not require iNO (n = 17). Data are presented as mean ± standard deviation, and data at each time point are offset for clarity.
Discussion
In our study sample of term and late preterm infants with respiratory distress, there was an inverse correlation between fT4 and illness severity. This was manifest as an inverse correlation between SNAP and fT4 at birth, and lowest T4 and highest SNAP during the first 5 days of life. There was also an inverse correlation between lowest measured fT4 and degree of respiratory illness, as quantified by mean airway pressure, OI, and A-a gradient. Those infants receiving iNO also had decreased fT4 over the study time. Infants with severe illness had a decreased TSH at birth. There were no overall differences in total T4 or fT4 levels over the first 5 days of life in those infants whose illness severity at birth exceeded a predetermined threshold (SNAP ≥10) compared to those infants without elevated illness.
Transient hypothyroxinemia, defined as low levels of T4 and normal levels of TSH, has previously been associated with adverse outcomes in infants with a very low birth weight (3,5,6,15). An association between decreased total T4 and outcome has previously been shown in term infants with respiratory distress (10). This previous study of thyroid function in mechanically ventilated term infants was a retrospective study looking at total T4 and TSH levels and did not include fT4, which is the bio-available form of the hormone (10).
Our present study is important in showing an association between low fT4 and severity of illness on the day of birth. In our sample of term and late preterm infants, low levels of fT4 were also associated with increased respiratory illness. This association was demonstrated by the inverse correlation of fT4 with three different parameters used to quantify respiratory illness, A-a gradient, OI, and mean airway pressure. There were, however, no overall differences in fT4 levels over the first 5 days of age in infants with severe illness at birth compared to infants without severe illness. This finding must be viewed in the context that our study was powered to detect a large (50%) difference in fT4 in infants with severe illness compared to those without severe illness. Our study was therefore underpowered to detect smaller differences in fT4 levels between groups.
In our previous study, we investigated thyroid function in relationship to term infants who died or required ECMO (10). No babies in the present study fulfilled those criteria. We were able to investigate thyroid function in those infants receiving iNO. iNO is a proven rescue therapy for term infants with persistent pulmonary hypertension of the newborn (16). It is important to note that initiation of iNO was based on clinical judgment. In our NICU, term and near term infants are usually placed on iNO based on a persistent oxygenation index >15, usually after the initiation of high-frequency ventilation and other rescue therapies, including systemic blood pressure support and pharmacologic paralysis. Those infants receiving iNO in our study sample represented the infants with the most severe lung disease. To our knowledge, there has been no reported association between iNO and hypothyroxinemia. There are a number of possible alternative interpretations of our finding of low fT4 in infants receiving iNO. It is possible that iNO had a direct effect in lowering fT4. Other medication such as dopamine and dobutamine have previously shown to cause a reduction in TSH (17,18).
Our finding of an association between fT4 and illness severity in late preterm and term infants with respiratory distress is consistent with previous research on very premature infants. Van Wassenaer et al. previously demonstrated a decrease in fT4 levels in ill infants who had <30 weeks of gestation during the first week of life (8). Lower levels of fT4 have been associated with the need for mechanical ventilation at 2 weeks of age in infants who had <30 weeks of gestation (19). An inverse relationship between the level of intensive care and fT4 in infants with 23–27 weeks has been shown (20). We have previously demonstrated an association between higher SNAP and lower levels of total T4 infants with <1500 g birthweight (2).
In our study sample, there was no association between cortisol levels and severity of illness. Previous studies by Watterberg et al. have demonstrated a correlation between low cortisol levels and development of chronic lung disease in preterm infants (13,21). It has been speculated that low cortisol levels interfere with the ability to respond to inflammatory stimuli and thus contribute to chronic lung disease (13). In our study we investigated short-term pulmonary outcomes such as need for mechanical ventilation, A-a gradient, and mean airway pressure, in addition to illness severity. However, in our study population, no association was noted between cortisol and these outcomes. Our study supports the finding of Fernandez et al., who showed no association between illness severity and decreased cortisol in term and late preterm infants (22).
Our study has a number of important limitations. Our data are from a single center and the need for iNO was determined by clinical judgment. However, because clinicians were blinded to the infant's thyroid levels and a protocol was in place to initiate iNO therapy, the infants who receive iNO likely represented infants with the greatest degree of respiratory distress. In the present study some infants who required only N-CPAP were enrolled. This was done to capture infants with moderate respiratory distress as well as those infants whose respiratory disease may be progressive. By chance, none of the infants in our study sample required ECMO. Further, only infants who required mechanical ventilation or N-CPAP were included. Our results may therefore not be generalizable to infants with very mild or extremely severe respiratory distress. We measured hormone levels only at four intervals to minimize blood loss and discomfort to the infants. It is possible that more frequent sampling or longer follow-up may have changed our findings. fT4 values have been shown to differ based on analytic methodology with nonequilibrium dialysis methods overestimating hypothyroxinemia (23). However, because our study compared fT4 in infants with and without SNAP ≥10, and those receiving iNO, our methodology for measuring fT4 was unlikely to have influenced the results. In this study, we defined severe illness at birth based on an SNAP ≥10. This threshold level was based on our previous studies in premature infants (2) and must therefore be interpreted with caution when applied to a more mature study population. Infants with severe illness had their first blood samples obtained earlier, which may have had some influence on lower levels of TSH compared to infants without severe illness. However, there were no correlations between TSH levels drawn at birth and the time of life samples were obtained.
In summary, our study shows an association between illness severity at birth and fT4 levels in term and late preterm infants with respiratory distress. Those infants with severe illness also had decreased TSH levels after birth. Infants who received iNO had lower fT4 compared to infants who did not receive this therapy, and there was an inverse correlation between low T4 levels and respiratory illness, including OI and A-gradient. From our research we cannot determine if the observed decrease in fT4 after birth in infants with the highest SNAP may be part of a causal pathway leading to need for iNO or increased respiratory support. Our study is important in highlighting changes in thyroid function, particularly fT4, in term and late preterm infants with respiratory distress and is important for neonatologists and pediatricians caring for this population. Our data suggest the need for randomized trials of thyroxine supplementation in term and later preterm infants with respiratory distress.
Footnotes
Disclosure Statement
The authors have no commercial associations or conflicts of interest to disclose.