
Abstract
Background:
Musculoskeletal complaints are common in patients with thyroid dysfunction. Both thyrotoxic and hypothyroid myopathy have been well described, and there are distinct presentations, laboratory findings, and clinical outcomes between the two groups. Myopathy has also been reported in hyperthyroid patients only after beginning treatment, suggesting that relative hypothyroidism may also contribute to musculoskeletal disease. A confounding factor in these cases was that these patients were on antithyroid drugs that may also have direct effects on the muscle, irrespective of the rate of decline in thyroid hormone levels.
Summary:
We report a patient with Graves' disease who developed myalgias with elevated creatine kinase levels after total thyroidectomy. Addition of triiodothyronine quickly resolved her symptoms and creatine kinase levels, whereas discontinuation of triiodothyronine, despite having normal to elevated total thyroxine levels, led to a relapse.
Conclusion:
Myositis after correction of thyrotoxicosis may constitute a syndrome that should be assessed for in hyperthyroid patients complaining of myalgias after starting treatment.
Introduction
Recent reports by Suzuki et al. (4) and Mizuno et al. (5) have described hyperthyroid patients who developed myositis only after starting antithyroid drugs. Although these patients had normal or elevated thyroid hormone levels, they had features typical of hypothyroid myopathy (4,5). Interestingly, reduction in the patient's antithyroid drug dose and/or addition of levothyroxine (LT4) successfully treated the myalgias and CK elevation (4,5). It was postulated that some patients may be sensitive to correction of thyrotoxicosis, leading to a relative hypothyroid state in the muscle (4). We present a case of a patient with Graves' disease whose total thyroidectomy was complicated by myositis with CK elevation over 20 times the upper limit of normal. Unique to this case was the rapid improvement of our patient's symptoms with triiodothyronine (T3) administration.
Case Report
A 24-year-old Caucasian woman presented to her primary physician in August 2007 with complaints of diarrhea, dizziness, palpitations, heat intolerance, and a 15 lb unintentional weight loss over a 6-month period. Her past medical history was notable for birth of a healthy son 1 year ago and a lumbar laminectomy at the age of 17 years. She smoked cigarettes, and her only medication was an oral contraceptive. She had no known drug allergies. There was a positive family history of thyroid disease with a maternal grandmother with hyperthyroidism of unclear etiology and a maternal aunt with toxic multinodular goiter, but no thyroid cancer. Her initial thyroid function tests were consistent with primary hyperthyroidism: thyrotropin (TSH) <0.03, total thyroxine (T4) of 23.3 (normal 4.5–10.9 μg/dL), total T3 of 759 (normal 80–220 ng/dL), and free thyroxine (FT4) index of 33.6 (normal 5.5–11.5 μg/dL) (Fig. 1). She had an elevated thyroid-stimulating immunoglobulin level (Table 1) and an I-123 thyroid uptake, and scan showed 44% uptake at 4 and 24 hours (reference range at 4 hours: 5–15% at 4 hours and 25–31% at 24 hours) with increased uptake diffusely; these results were consistent with a diagnosis of Graves' disease.
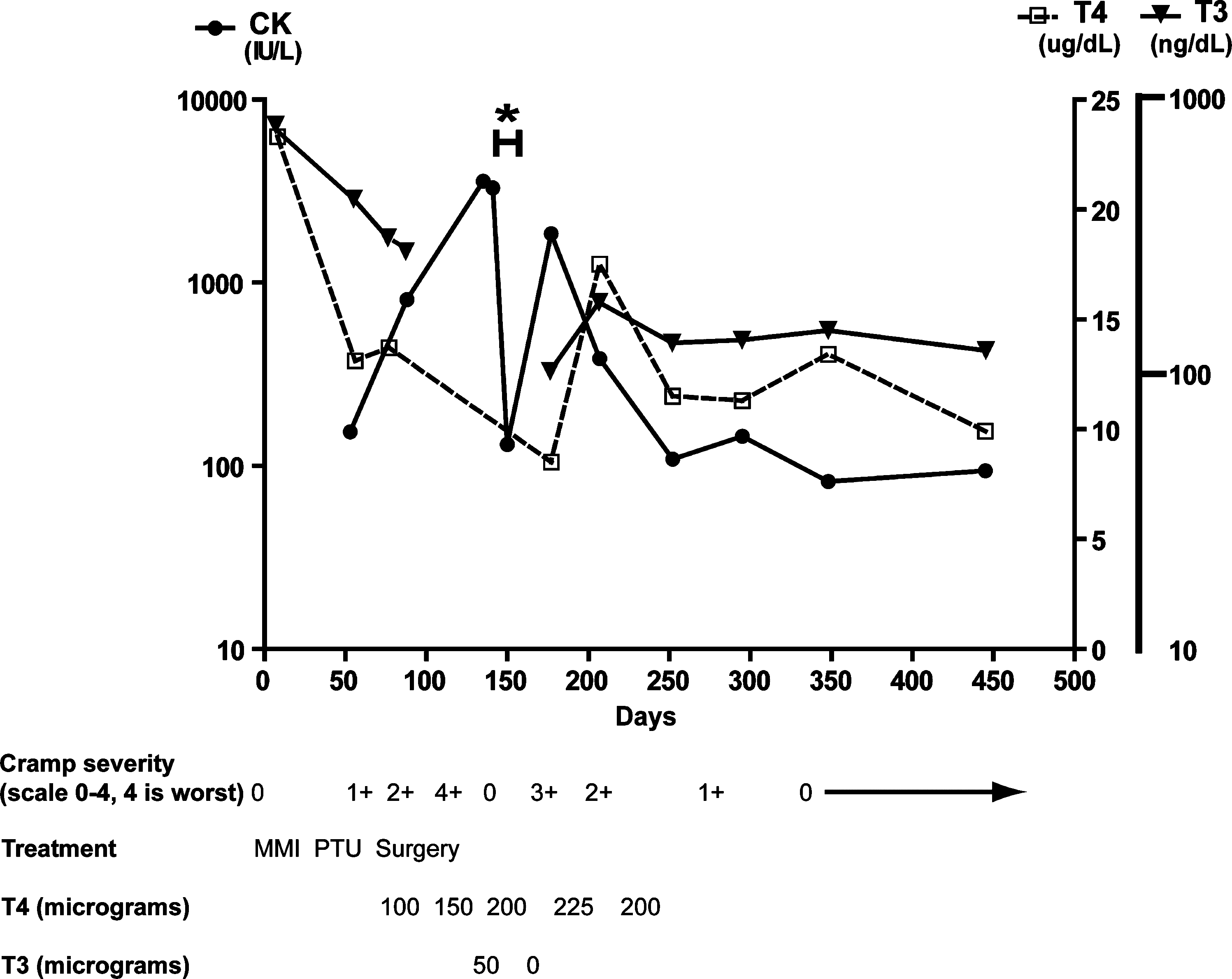
Time course of serum creatine kinase (CK), total thyroxine (T4), and total triiodothyronine (T3) levels before starting, during, and after discontinuation of thionamide therapy. Peak CK elevation and severity of muscle cramps occurred over 10 weeks after discontinuation of her antithyroid medication. The asterisk (*) marks the time the patient was on T3 therapy with rapid normalization of her CK level. When T3 therapy was stopped, the CK level increased again.
CK, creatinine kinase; ANA, antinuclear antibody test; RNP, ribonucleoprotein antibody; SSA, Sjogren's syndrome A antibody; c-ANCA, antineutrophil cytoplasmic antibody; p-ANCA, antineutrophil protoplasmic antibody; MUSK, muscle-specific tyrosine kinase.
The patient was started on atenolol and methimazole 30 mg a day, which alleviated the majority of her symptoms. Three weeks later, she developed left shoulder pain and bilateral hand swelling. Her complete blood count (CBC), liver function tests (LFTs), and electrolytes were normal, and she was referred to endocrinology (Table 1). On evaluation, her blood pressure was 110/60 mmHg and pulse was 70 beats/min. Pertinent findings on examination included a thyroid 35 g in size, firm, and no bruit detected. No thyroid nodules or cervical lymph nodes were appreciated. Her joint examination revealed nontender bilateral swelling of the proximal interphalangeal joints, which were not warm to touch. Labs drawn at that time showed improving hyperthyroidism and a negative rheumatologic work-up; her CK level was at the upper level of normal at 153 (20–165 IU/L) (Fig. 1 and Table 1).
We attributed her symptoms to an adverse reaction to her methimazole. She did not wish to undergo radioactive iodine therapy; therefore, we switched her to a low dose of propylthiouracil (PTU) 50 mg twice a day (BID) with subsequent resolution of her hand swelling and shoulder stiffness. Lab work 3 weeks later showed improved but persistent hyperthyroidism (Fig. 1). During this time, she developed leg cramping and intermittent sharp chest pain necessitating an emergency room visit at a local hospital; her electrocardiogram showed a normal sinus rhythm of 81 bpm, QT interval of 371 ms, and QT corrected of 431 ms. Electrolytes and troponin levels were normal. Her CK level was not checked at that time, and she was discharged with an impression that her symptoms were a side-effect from her PTU, which was not discontinued. Work-up in our clinic 2 days later showed that her CK level was now elevated at 809 (normal 20–165 IU/L) with a normal CK-myocardial band (CK-MB) isoenzyme level of 1 (normal 0–5 ng/dL). An echocardiogram showed no focal wall motion abnormalities or evidence of pericardial effusion. Examination showed a component of reproducible chest pain on palpation of her chest, suggesting that breakdown of her pectoral wall muscles were the likely cause of her angina. Normal c-ANCA, erythrocyte sedimentation rate, and C-reactive protein levels did not indicate the presence of vasculitis or other inflammatory processes. Given the severity of her symptoms and continued hyperthyroidism, she elected total thyroidectomy versus radioactive iodine or continuing on a lower dose of thionamides.
Her PTU was discontinued before her total thyroidectomy in November 2007. The pathology was reported as consistent with treated Graves' disease with a single 1 mm focus of microscopic papillary thyroid carcinoma with clear margins. She was discharged on 100 μg of generic LT4, and her beta-blocker was weaned off. Several weeks after surgery, she complained of worsening muscle cramps and chest pain. Her thyroid function tests showed TSH of 6.69, FT4 of 0.7 (normal 0.6–1.7 ng/dL), and an elevated CK at 3579 and normal CK-MB of 4.4 (Fig. 1). Her LT4 was then increased to 150 μg a day along with addition of liothyronine (Cytomel) 25 μg twice a day. Almost immediately after starting this regimen, the patient had complete resolution of her symptoms. Eight days after starting the Cytomel, her TSH was 0.05, T4 11.5, FT4 1.1 with a normal CK level of 131, and her Cytomel was discontinued. However, several weeks later her muscle cramps and intermittent chest pain recurred. Labs showed TSH 5.61, T4 8.9, FT4 0.8, T3 102, and CK level of 1851. The patient was taking her LT4 appropriately, and there were no new complaints suggestive of malabsorption; she declined to switch to a brand name LT4 or to restart Cytomel due to cost. Her LT4 dose was then increased to 225 μg a day with gradual improvement of her myalgias (Fig. 1).
One month later after continuing LT4 alone, the patient was found to be mildly overreplaced (TSH of 0.06, T4 17.9, FT4 1.93, and T3 181), but her CK level was still elevated at 386. Although her muscle cramps improved during this time, she began to re-experience palpitations and dizziness, which were similar to her original presenting symptoms of hyperthyroidism. Her LT4 dose was decreased to 200 μg a day, and atenolol was resumed. Neurology evaluation found normal strength in her upper extremities and very mild proximal upper extremity weakness. Additional work-up was negative for an intrinsic muscle disorder, including normal electromyography (EMG) testing (Table 1). Gradually her palpitations and dizziness resolved, and her beta-blocker was tapered off. About 6 months after the initial observation of an elevated CK, she was biochemically and clinically euthyroid: TSH 0.57, T4 11.5, FT4 1.3, and T3 129 with a normal CK of 109. Labs approximately 1 year from the initial observation of an elevated CK showed TSH of 0.29, TT4 9.9, FT4 1.4, and TT3 121 with CK 94, and the patient was asymptomatic with normal strength throughout. Her LT4 dose is being gradually decreased to achieve a TSH in the normal range.
Discussion
Thyroid hormone has a central role in muscle function, and thyroid dysfunction can cause a wide spectrum of myopathies. Thyrotoxic myopathy typically consists of weakness and myalgias without elevation of CK and may be considered a functional, versus structural, alteration of the muscle contractile unit leading to symptoms (1,6,7). Hypothyroid myopathy is documented by pathologic alterations of muscle skeletal fibers and/or muscle injury with increased CK levels (1,3). Additional patterns distinguishing these two types of myopathies include the lack of electro myogram (EMG) findings and faster resolution of thyrotoxic myopathy (1).
Recently, several cases have reported myositis developing in hyperthyroid patients on thionamides due to relative hypothyroidism, as these patients still had normal or elevated thyroid hormone levels when their symptoms occurred (4,5). This hybrid myopathy combines the features of quick symptomatic improvement seen in patients with thyrotoxic myopathy with the elevated CK levels found in patients who are severely hypothyroid (4,5). Our patient had no documented hypothyroidism in contrast to prototypical patients with hypothyroid myopathy. Duyff et al. did not see a difference in thyroid function tests among the hypothyroid patients with and without myopathy (1); however, the hypothyroid group had significant primary hypothyroidism with the mean TSH 53 (normal 0.4–4 mU/L) and FT4 6.1 (12–24 pM). Our patient's first abnormal CK level occurred with a normal FT4 and a T3 level that was slightly above normal at 277 (Fig. 1). In fact, the initial CK reading was at the upper limit of normal and may have signified the development of relative hypothyroidism. Two months after stopping PTU and several weeks post-thyroidectomy, she developed severe muscle cramping with an elevated CK of 3579, elevated TSH of 6.69, and FT4 level of 0.7, which was at the lower limits of normal.
While rare in the literature, relative hypothyroid-associated myopathy may be overlooked given its presentation only after starting treatment for hyperthyroidism and therefore may be attributed to an antithyroid drug side effect. The thionamide class of antithyroid drugs, which includes methimazole and PTU, is associated with musculoskeletal side effects, and the prior cases of relative hypothyroidism did not discontinue their thionamides (4,5,8). Infrequently, thionamides lead to the antithyroid arthritis syndrome, consisting of a migratory polyarthritis that usually resolves within a month after discontinuation of the drug and is not associated with elevated CK levels (9,10). Other etiologies include a primary rheumatologic disorder. Shergy and Caldwell described a case of polymyositis in a patient on PTU (11). However, our patient's normal autoimmune profile (Table 1) did not suggest a second disease process. Her normal EMG and the temporal observation of relapse and remission of her symptoms with her fluctuating thyroid hormone levels also make polymyositis unlikely. Patients with thyrotoxic periodic paralysis may have elevated CK levels when measured during a paralytic episode (12,13); however, this patient never had significant weakness. In addition, her symptoms worsened with amelioration of her hyperthyroidism, which is the opposite response seen in patients with thyrotoxic periodic paralysis.
Identification of myositis due to relative hypothyroidism is important, as it may lead to a slower correction of the patient's hyperthyroidism and lessen further muscle damage. A more serious complication from relative hypothyroidism would be rhabdomyolysis. Rhabodmyolysis is typically seen in hypothyroid patients, but there have been four reported cases of rhabdomyolysis in hyperthyroid patients who quickly improved with antithyroid drugs and supportive measures (14 –16). Rhabdomyolysis is a clinical diagnosis, but it has traditionally been thought of as muscle destruction with CK elevation and renal compromise (17 –20). A recent panel of the National Lipid Association has recommended to replace the term “rhabdomyolysis” with “mild, moderate or marked” levels of CK elevation (20). Interestingly, a recent case by Lichtstein and Arteaga reported rhabdomyolysis due to hyperthyroidism with peak CK of 1276, myalgias and objective muscle weakness, and no evidence of renal dysfunction (15). However, this patient's symptoms began after initiation of PTU and resolved quickly with supportive measures. They did not compare pre- and postthionamide treatment T3 levels, so it is unclear if there was a rapid reduction in T3 levels after starting the PTU. Although the authors have attributed the patient's rhabdomyolysis to hyperthyroidism, an alternative explanation is that the decline in thyroid hormone levels led to myositis.
The theory of relative hypothyroidism resulting in myositis is supported by this patient's rapid symptomatic improvement and normalization of CK levels with the addition of T3 followed by a relapse with discontinuation of her T3. Within days of after addition of T3 to her LT4 regimen, her symptoms disappeared, and her CK levels normalized in 8 days, which is striking as the half-life of CK is approximately 1.5 days (17). In contrast, hypothyroid myopathy may persist for months to years after return to biochemical euthyroidism (1), and CK normalization may take months (21,22). Patients with polymyositis-like syndrome in hypothyroidism were reported to take an average of 9 and 12 weeks, after starting LT4, for CK level and clinical normalization, respectively (3). Our patient's complaints regarding the severity of her muscle cramps were reflective of the degree of her CK elevation, suggesting muscle damage, as one could theorize that her relative hypothyroidism only led to decreased renal clearance of CK (23). While on LT4, the patient was biochemically hyperthyroid (TSH 0.05, T4 17.5, FT4 1.93, and T3 181), but her CK level was still elevated at 386 and symptomatic. Indeed on LT4 therapy alone, she followed a similar course regarding recovery time for hypothyroid myopathy as it took several months for her symptoms to resolve after Cytomel discontinuation (Fig. 1).
This patient's response with the addition of T3 may suggest a local T3 deficiency in skeletal muscle. While on combination T4/T3 therapy, her T4:T3 ratio was ∼4:1, which is over the recommended physiologic replacement of at least 10:1 (24). Studies by Danzi et al. have shown that T3 can regulate myocyte gene expression over several hours (25,26). Cardiac muscle preferentially transports T3 over T4, and the use of T3 as treatment for cardiac diseases is under active investigation (27,28). In skeletal muscle, Clement et al. have shown that at least 17% of muscle-specific genes were modulated by thyroid hormone (29). Our patient's improvement with T3 highlights its role in muscle homeostasis.
It is important to identify patients who will be susceptible to relative hypothyroidism. The majority of cases were Asian, so there may be a genetic component. It is unclear how long our patient was hyperthyroid before treatment, but other cases suggested that the duration of hyperthyroidism may also be a risk factor (5). One hypothesis for development of relative hypothyroidism is that these patients may have a deficit with transport and/or production of local T3 in skeletal muscle. Recent studies have also shown how thyroid hormone transporters and deiodinases are important in maintaining local thyroid hormone levels (30 –33).
This case of severe myositis in the setting of reduced but still elevated thyroid hormone levels, in a patient off thionamides, strongly supports the concept of relative hypothyroidism. This may represent a syndrome that is underreported, and the development of myalgias after initiation of treatment for hyperthyroidism should prompt an evaluation for myositis with measurement of the CK level and/or other markers of muscle breakdown (e.g., aldolase and myoglobulin). Recognition of relative hypothyroidism has been addressed in this and other case reports with either a slower correction of a patient's hyperthyroidism or the concurrent use of T4 with thionamides, or in using T3 (4,5). Additional investigation is necessary to understand the pathophysiology of this syndrome.
Footnotes
Acknowledgments
We thank S.Y. Cheng and P.R. Larsen for helpful comments in the evaluation of this case.
Disclosure Statement
The authors declare that no competing financial interests exist.