
Abstract

We illustrate the features of a rare synchronous parathyroid carcinoma (P-Ca) and papillary thyroid microcarcinoma (mPTC) in the same individual.
The patient was a 42-year-old woman with a history of 40 Gy irradiation to the cervical, mediastinal, and axillary nodes as well as Mechlorethamine Oncovin Procarbazine Prednisone chemotherapy for Hodgkin's disease, 19 years earlier. She had no family history of thyroid cancer or multiple endocrine neoplasia type 1 or 2. She presented with symptoms of severe hypercalcemia (141 mg/L) and had increased serum parathyroid hormone (PTH) level (383 pg/mL) with a thyrotropin level of 1.1 μM. Physical examination revealed a right nodular thyroid without recurrent nerve palsy. On ultrasound (US), her thyroid was multinodular with a 13 mm highly hypoechoic postero-inferior vascularized oval nodule behind the right lobe (Fig. 1). On the other side, a 7 mm hypoechoic solid inferior lobe nodule and an ipsilateral level VI lymph node (central compartment) were noted (Fig. 2). Elsewhere, micronodules had sponge-like or solid features that were interpreted as benign. Technetium-99 m-methoxyisobutylisonitrile (MIBI) cervical and mediastinal substraction scintigraphy scans revealed increased uptake of right inferior lobe and left polar superior area of thyroid. US-guided fine-needle aspiration analysis of right retrothyroid nodule and left superior thyroid nodule was inconclusive. Blood and urine tests and calcitonin levels were normal, making multiple endocrine neoplasia type 2 very unlikely. Biphosphonate therapy was immediately started, but there was only a slight decrease of her hypercalcemia to 134 mg/L. A thyroidectomy, right parathyroidectomy, and central and lateral cervical lymph node dissection were performed and after these procedures she became normocalcemic. Histopathological examination revealed a right inferior P-Ca with vascular emboli and extracapsular spread associated with a multifocal mPTC. There was an 8 × 5 mm mPTC in the left lobe and a 5 mm mPTC in the right lobe. There was also one metastatic lymph node next to the left recurrent nerve (level VI) (Figs. 1 and 2). Her thyroid carcinoma was staged multifocal pT1 (0.8–0.5–0.5 cm) pN1M0 (TNM AJCC 2007), and she received one therapeutic dose (3.49 GBq) of I131. She is well and without disease 14 months after surgery.
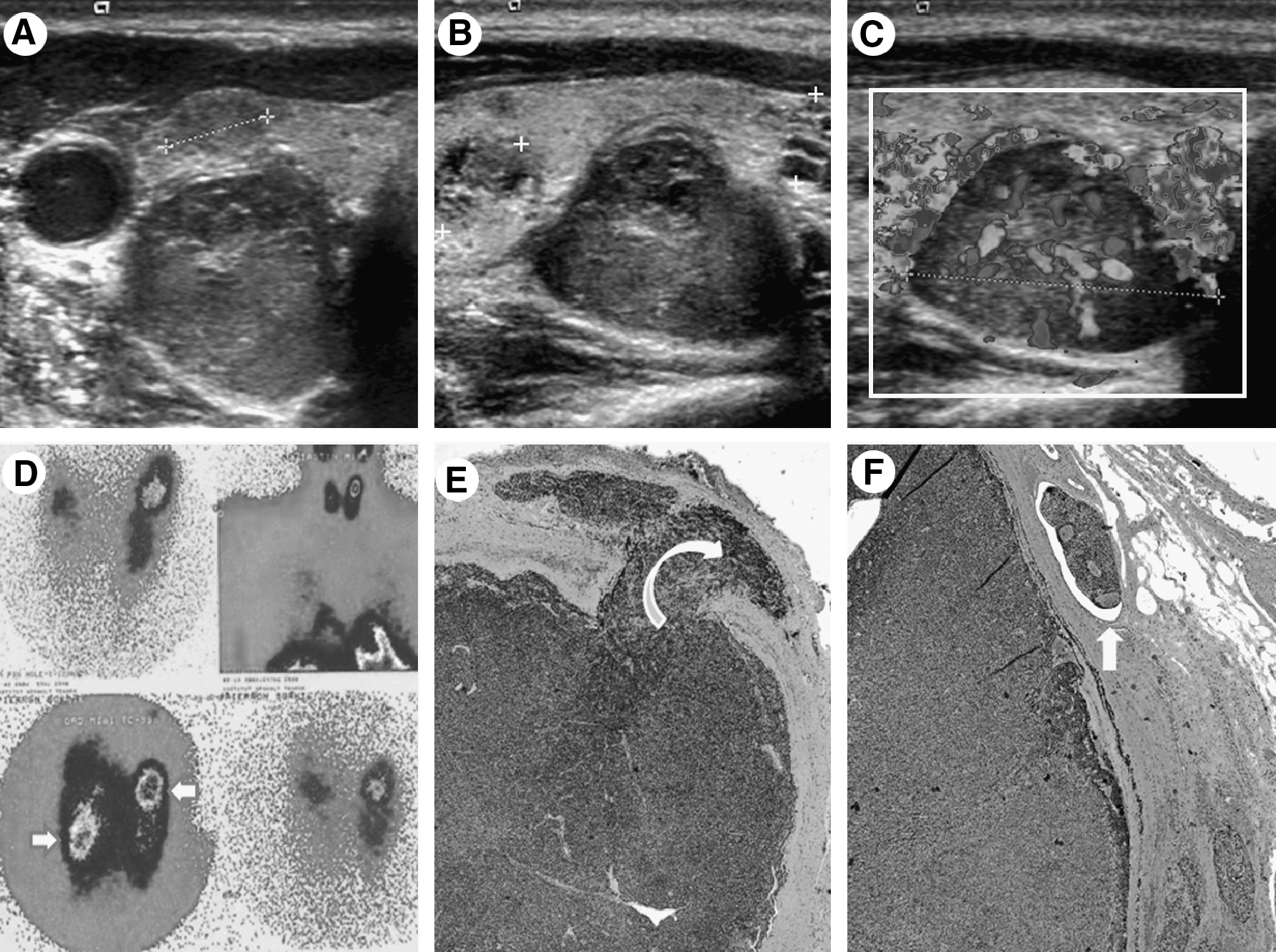
Parathyroid imaging. Ultrasound (US) scan of the right thyroid lobe (
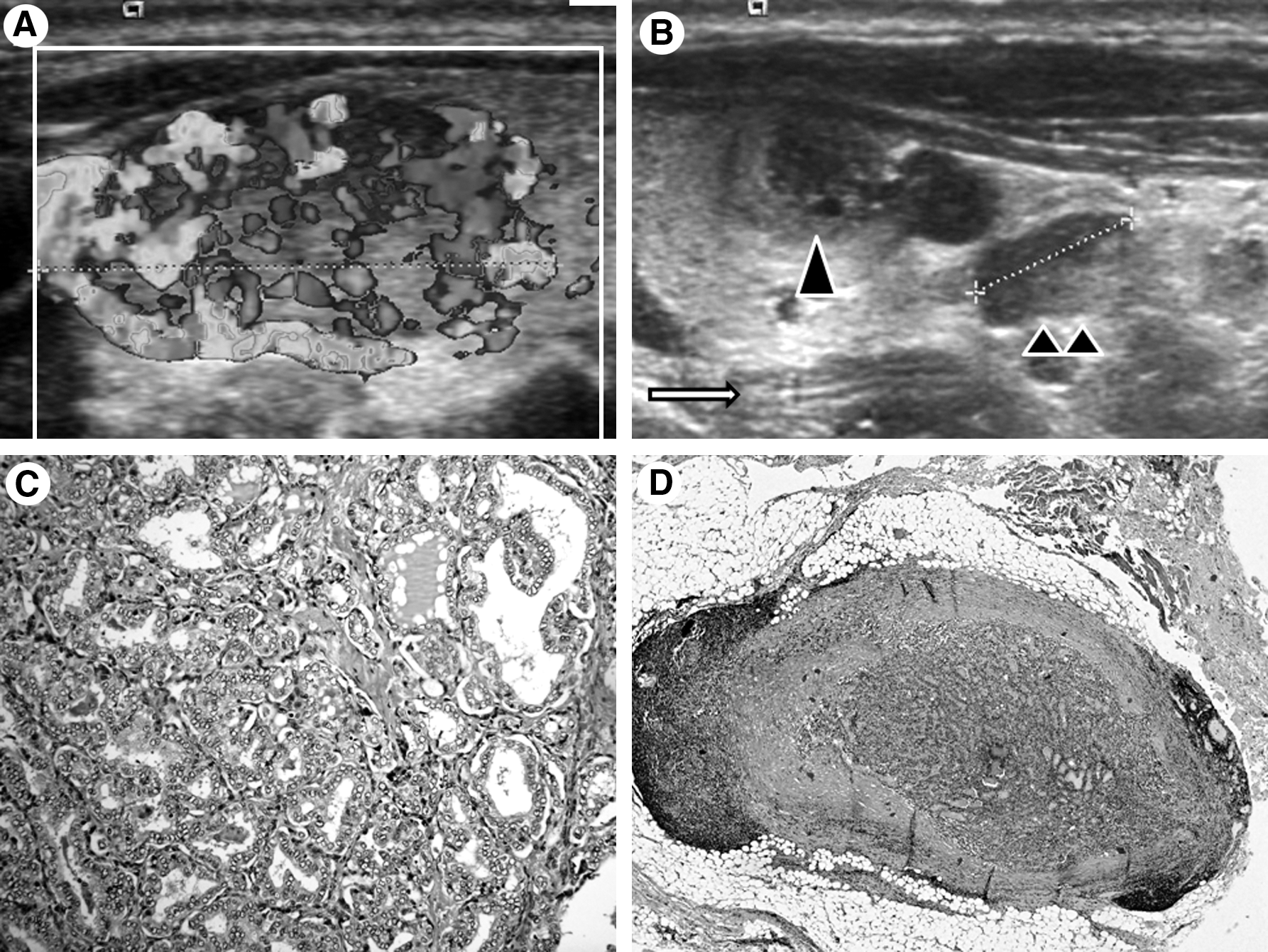
US sagittal scans and histopathology of upper (
P-Ca is a rare endocrine tumor and is responsible for less than 1% of the cases of hyperparathyroidism. Radical surgery offers the best chance of cure. Nevertheless in more than 50% of the cases, patients experience persistent or recurrent disease due to regional or distant disease (1). Papillary thyroid carcinoma (PTC) is the most common endocrine malignancy and frequently metastasizes to regional lymph nodes. Surgery therefore consists of initial en bloc—resection of the tumor and cervical lymph node dissection. Dissection of the central lymph node compartment firsthand may be recommended when the mPTC exceeds 5 mm (Fig. 2B, D) (2). The presence of severe hypercalcemia and increased PTH and a palpable cervical nodule suggests P-Ca (1,3) (Fig. 1). In the present case, the simultaneous occurrence of two carcinomas (multifocal mPTC and P-Ca) in a previously irradiated area was suggestive of radio-induced cancers (4). The addition of chemotherapy to radiotherapy in Hodgkin's disease treated in the childhood increases the risk of cancer by 4.4 times compared to 2.8 times with radiation alone (5). In addition to age and sex, external irradiation to the neck is regarded as a significant risk factor for parathyroid adenomas with a standardized incidence ratio of 1.83 (95% confidence interval 1.14–2.76) (6). The malignant form of hyperparathyroidism, P-Ca, is very rare when considering the high incidence of benign parathyroid neoplasias (no published standardized adenoma/carcinoma incidence ratio). A specific translocation of the RET gene in thyroid carcinoma has been reported (7), while somatic MEN1 (50%) has been noted in irradiation-associated parathyroid (8). However, individual genetic susceptibility probably influences the occurrence of cancer after radiotherapy. Individuals who have Hodgkin's disease may also have a genetic susceptibility as they seem to have more breast and thyroid cancers (9).
In the present case, the diagnosis of P-Ca was suggested before surgery by the following criteria: a palpable lateral neck mass with high levels of PTH and, on US, a near round shape, ill-defined borders, and central vasculature inside the hypoechoic retrothyroid nodule. The ability of the US-guided fine-needle aspiration to diagnose a parathyroid lesion would have been enhanced if the sample from the tumor was assayed for PTH (10). The preoperative diagnosis of P-Ca is very important as the initial surgery should not only be diagnostic but also, if possible, remove the entire tumor.