
Abstract
Background:
No conventional imaging method reliably distinguishes between benign and malignant thyroid nodules. Our objectives were to characterize the enhancement patterns of thyroid nodules on gray-scale contrast-enhanced ultrasound (US) and to evaluate whether these patterns were useful in the differential diagnosis of thyroid nodules.
Methods:
Ninety-five patients, scheduled for surgery for thyroid nodules detected by gray-scale sonography, were enrolled in this prospective study. In all, there were 104 nodules (47 papillary carcinomas, 3 medullary carcinomas, 1 metastatic carcinoma, 44 hyperplasia nodule, 7 follicular adenomas, 1 suture granulomas, and 1 Hashimoto's disease). After intraveneous (i.v.) injection of a 1.2 mL bolus of SonoVue, lesions were scanned with real-time gray-scale pulse inversion harmonic imaging US for at least 3 minutes at low mechanical index (MI) (0.05 to 0.08). The enhancement patterns were classified into one of four patterns by two experienced readers.
Results:
After administration of SonoVue, four enhancement patterns (homogeneous, heterogeneous, ring-enhancing, and no enhancement) were observed. Four benign and 3 malignant nodules had homogeneous enhancement pattern, 4 benign and 45 malignant nodules had heterogeneous enhancement, 44 benign and 3 malignant nodules had ring enhancement, and 1 benign nodule had no enhancement. There was a significant difference between benign and malignant nodules (p < 0.001). The benign thyroid nodules showed four enhancement patterns: ring enhancement 44/53 (83.0%), homogeneous enhancement 4/53 (7.5%), heterogeneous enhancement 4/53 (7.5%), and no enhancement 1/44 (1.9%). The malignant thyroid nodules showed three enhancement patterns: heterogeneous enhancement 45/51 (88.2%), ring enhancement 3/51 (5.9%), and homogeneous enhancement 3/51 (5.9%). Ring enhancement correlated highly with a benign diagnosis (sensitivity 83.0%, specificity 94.1%, positive predictive value 93.6%, negative predictive value 84.2%, and accuracy 88.5%). Heterogeneous enhancement correlated highly with a malignant diagnosis (sensitivity 88.2%, specificity, 92.5% positive predictive value 91.8%, negative predictive value 89.1%, and accuracy 90.4%). In both mixed and solid nodules, ring enhancement was highly predictive of a benign finding, whereas heterogeneous enhancement was highly predictive of a malignant finding.
Conclusions:
Contrast-enhanced US enhancement patterns were different in benign and malignant lesions. Ring enhancement was predictive of benign lesions, whereas heterogeneous enhancement was helpful for detecting malignant lesions.
Introduction
A relatively new technique, contrast-enhanced US (CEUS) has been shown to be a promising tool for studying the vascular pattern and flow dynamics of lesions within the liver (6). Sonographic contrast agents work by taking advantage of the propensity of microbubbles to create strong nonlinear harmonic echoes, greatly enhancing the visibility of small blood vessels. Pulse inversion harmonic sonography (7) is a technique that works by sending two separate pulses, 180 degree out of phase, and summing the reflected echoes to form the final sonographic signal. The linear fundamental frequency echoes reflected from the tissue nullify each other, whereas the nonlinear harmonic echoes reflected from the contrast medium produce a detectable signal. With the second-generation contrast agent, SonoVue, the examination can be performed with continuous real-time sonography at very low transmission power (mechanical index [MI] <0.3).
So far, only a few studies have focused on CEUS of thyroid nodules (8). Thus, the usefulness of CEUS in characterizing thyroid nodules has not been fully evaluated. For example, are there any characteristics that reliably distinguish benign and malignant nodules? What about the enhancement patterns of cystic, mixed, and solid nodules? Our intention in this study was to determine whether there are significant differences in enhancement patterns between benign and malignant lesions and to evaluate the potential of CEUS for characterizing thyroid nodules.
Methods
Patients
This study design and protocol were approved by the Ethics Committee of Peking Union Medical Hospital, and all patients gave informed consent before the CEUS. From August 2005 to December 2006, 168 consecutive patients underwent preoperative conventional US examination of the thyroid for the following indications: clinical symptoms and signs (58 patients), including hoarseness, cervical swelling, neck pain, palpable mass, and cervical lymph node enlargement on physical examination; asymptomatic incidentally found thyroid nodules (102 patients); and recurrent thyroid nodule after partial thyroidectomy (8 patients) for goiter, adenoma, and papillary thyroid carcinoma.
After conventional thyroid US examination, 100 patients underwent CEUS examination. The inclusion criteria were the presence of lesions on conventional US, lesion size greater than 0.5 cm (for lesions less than 0.5 cm, it was difficult to keep the same imaging section during CEUS examination due to arterial pulsations and breathing). Pregnancy, breast-feeding, or age less than 18 years were exclusion criteria and contraindication to CEUS. Four patients dropped out of the study after CEUS and did not have thyroid surgery. Ninety-six patients underwent total thyroidectomy or partial thyroidectomy. One case was excluded because the image quality was unsatisfactory. A total of 104 nodules in 95 patients (74 women, age range 19 to 80 years, mean 42.9 years; 21 men, age range 20 to 72 years, mean 48.7 years) were included in this prospective study.
In 64 patients with multiple nodules, the CEUS evaluation focused on the lesion most suspected of malignancy or the largest lesion. All final diagnoses were made by surgical pathology.
US system and contrast agent
All sonographic examinations were performed using two commercially available scanners (Philips HDI 5000 and iU22, Bothell, WA) equipped with an L12-5 transducer for conventional US and an L7-4 transducer (HDL 5000) and an L8-4 transducer (iU22) for CEUS. Standard machine settings were used, with MI 0.05 to 0.08, compress 33 to 35, and dynamic spatial reconstructor (DSR) middle. Once set, US parameters remained unchanged in each patient.
Contrast medium was SonoVue (BR1; Bracco Imaging, Milan, Italy), which is a sulfur-hexafluoride-filled microbubble contrast agent encapsulated by a flexible phospholipid shell. A white, milky suspension of sulfur hexafluoride microbubbles is obtained by adding 5 mL of physiological saline (0.9% sodium chloride) to the powder (25 mg), using standard clinical aseptic techniques, followed by hand agitation. The obtained microbubble density is 2108 microbubbles per milliliter (mean diameter 3 μm, 90% of the microbubbles <8 μm). SonoVue shows an elimination half-life of 6 minutes, and more than 80% of the compound is exhaled through the lungs in 11 minutes (9).
Conventional US and CEUS imaging
The mass or suspicious region, including the thyroid, the surrounding tissues, and the lymph nodes in the neck, was scanned carefully by gray-scale and color Doppler US. The dynamic range, gain, depth, and focal zone were adjusted to optimize image quality during the examination. The largest plane of the lesion was selected, and the transducer was switched to gray-scale harmonic CEUS mode. Since bubble disruption is related to depth and focal zone, the focus was always placed deeper than the nodule being examined to minimize microbubble disruption. Using a 20- or 22-gauge peripheral intravenous cannula, SonoVue was injected intravenously as a bolus at a 1.2 mL dose followed by 2 mL of normal saline flush. Meantime, the timer on the US machine was started and the imaging plane was keep as stable as possible. Each contrast imaging acquisition lasted at least 3 minutes after bolus injection and was digitally stored as raw data on a personal-computer-based workstation connected to the US unit via a standard Ethernet link.
Image analysis
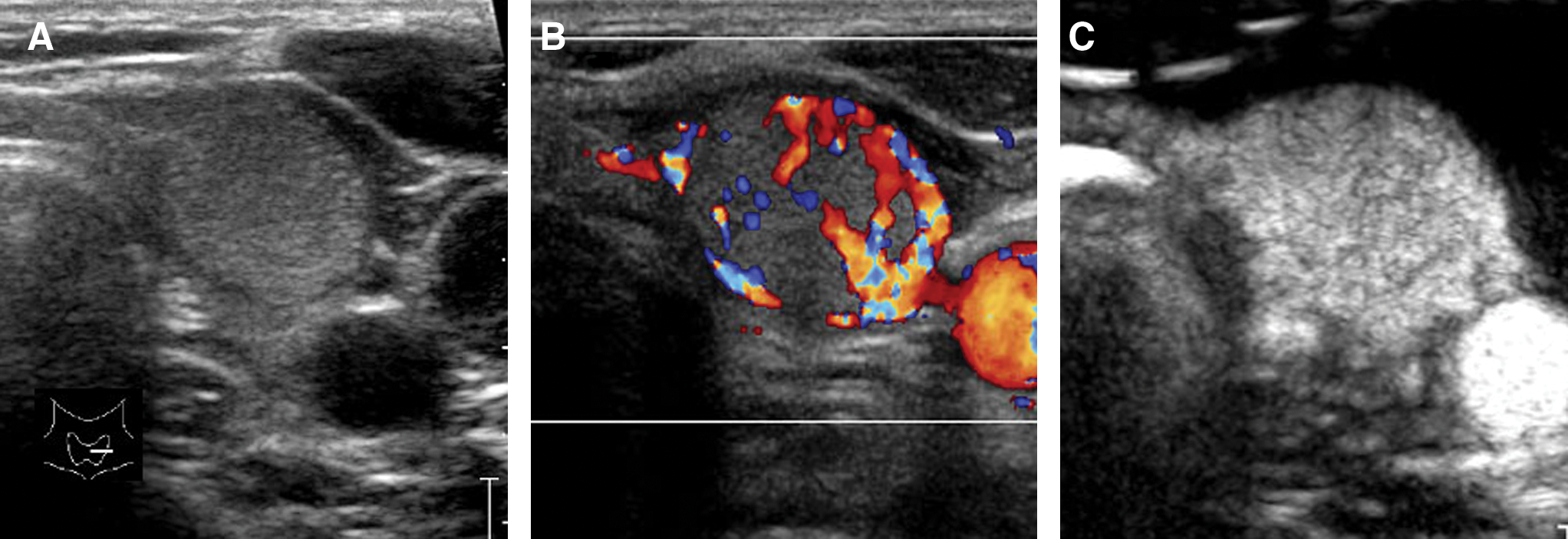
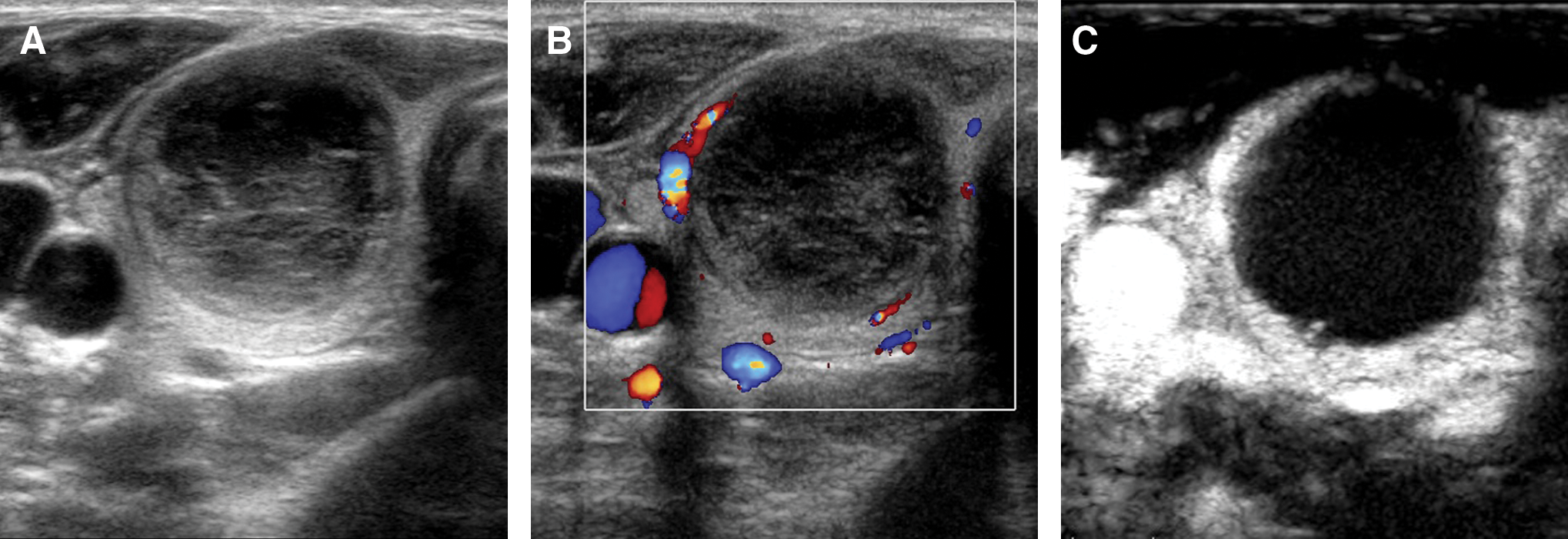
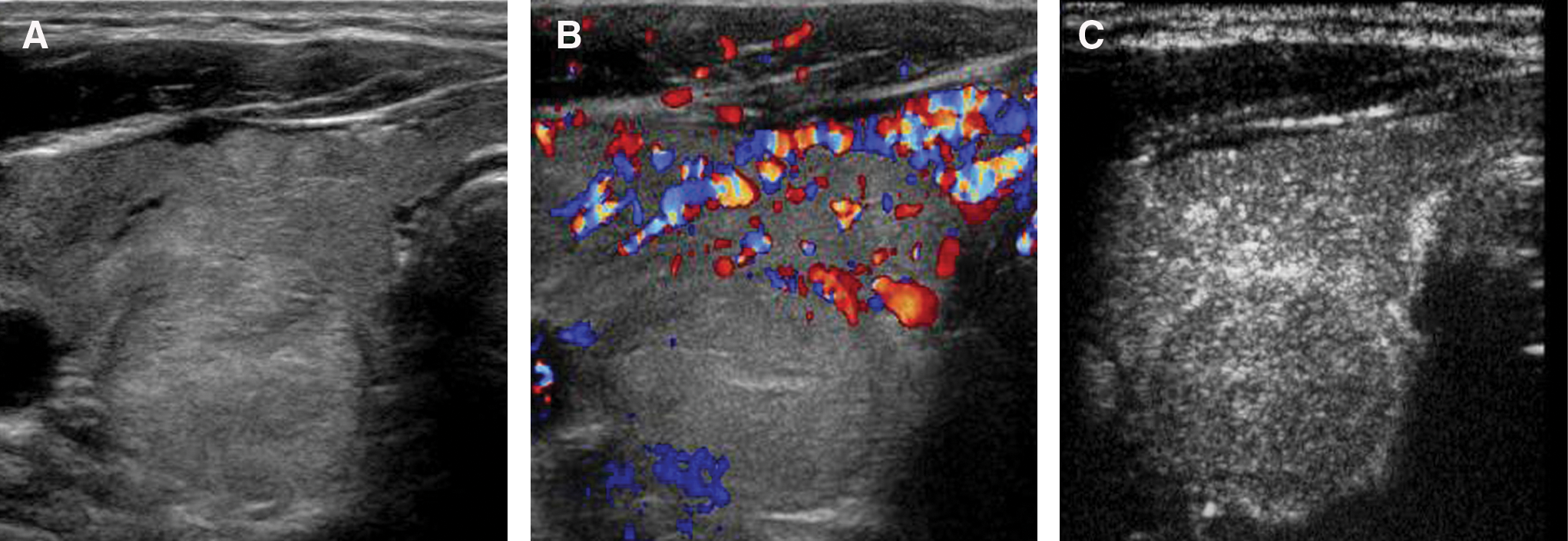
Scanning was performed by one experienced radiologist (B.Z., with 10 years experience in thyroid US). Digital video clips stored on the personal-computer-based workstation were reviewed in random order on screen by two radiologists (B.Z. and M.Y., with 6 years experience in thyroid US), who were blinded to the patient clinical data, fine-needle aspiration cytology (FNAC) findings, and history. Initially, each reader independently analyzed conventional and CEUS images. Subsequently, the two readers jointly reviewed the images in which there was a discrepancy in their opinions and which they had placed in different categories, and came to a consensus on the characterization of the enhancement patterns in those cases. The nodule echotexture was classified as cystic, complex (solid and cystic mixture), and solid by gray-scale images. On the basis of distribution of enhancement of the lesion, the images of CEUS were divided into four categories. The first was “homogeneous”; that is, the entire lesion was homogeneously and diffusely enhanced at the time of maximal enhancement. Figure 1 shows an example of the homogeneous pattern of distribution of enhancement within the lesion. The second was “heterogeneous”; that is, the lesion was partially or heterogeneously enhanced at the time of maximal enhancement. Figure 2 shows an example of the heterogeneous pattern. The third was “ring-enhancing”; that is, there was a rim-like enhancement around the lesion, which had a clear margin and could appear at wash-in or wash-out phase. Figures 3 and 4 show two examples of the ring-enhancement pattern. Once the peripheral echogenic ring appeared, the pattern would be the ring enhancement, with no consideration of whether there were homogeneous or heterogeneous features. The fourth pattern was “no enhancement”; that is, no microbubble echoes were detected within the lesion. Figure 5 shows an example of no enhancement.
In a 53-year-old woman with a palpable nodule in the left lobe of thyroid, surgical pathology proved a hyperplasia nodule. (

In a 19-year-old woman with a palpable nodule in the isthmus of thyroid, surgical pathology proved a papillary thyroid carcinoma. (
In a 31-year-old woman with a palpable mass in the right lobe of thyroid, surgical pathology proved a hyperplasia nodule. (
In a 60-year-old woman with a palpable mass in the right lobe of thyroid, surgical pathology proved a hyperplasia nodule. (
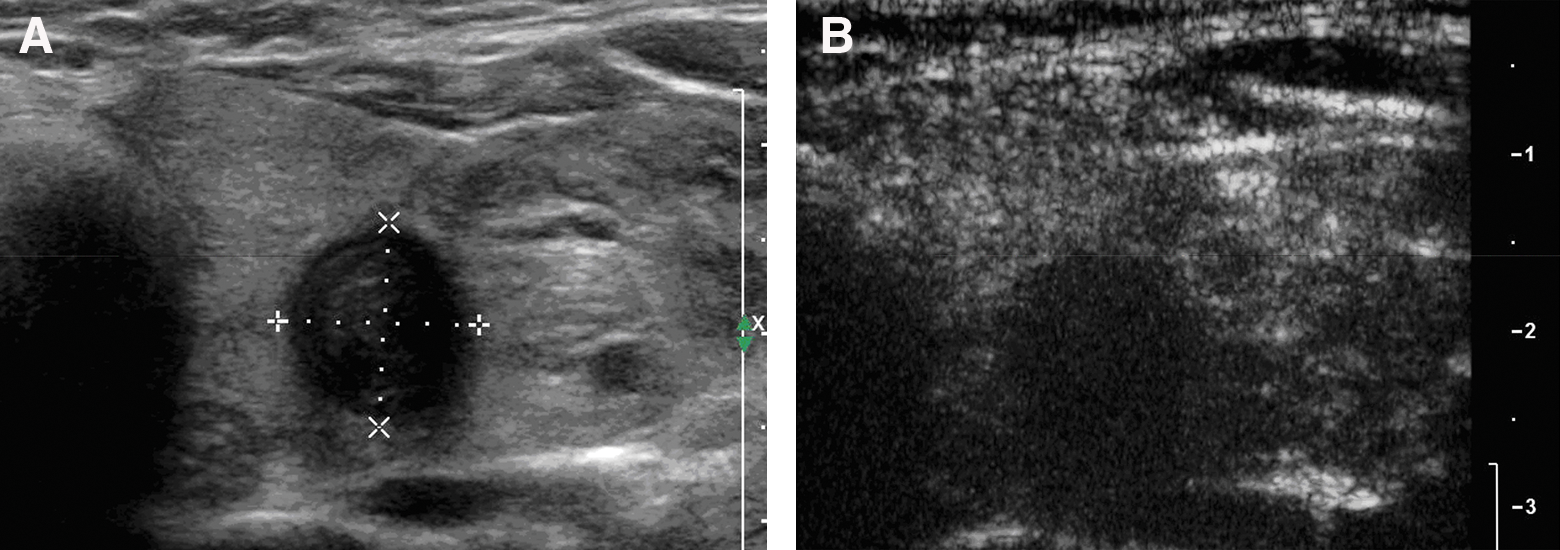
In a 44-year-old woman with a nonpalpable mass in the left lobe of thyroid, surgical pathology proved a hyperplasia nodule with old hemorrhage. (
Histological analysis
All surgical specimens were categorized according to the World Health Organization (2003) histological classification of tumors of the thyroid (10) by experienced pathologists who were blinded to the medical history and US findings. The final pathological diagnosis was used as a gold standard for the study.
Statistical analysis
The statistical analyses were performed using a statistical package (SPSS 11.0, Chicago, IL). Quantitative data were expressed as mean with standard deviations. Groups were compared using Student's t-test. The chi-squared test, Fisher's exact test, and kappa concordance test were used to compare categorical data. In all cases, a p-value less than 0.05 was considered statistically significant.
Results
Lesion diagnosis
Among 104 thyroid nodules that were surgically removed, 53 were benign (44 hyperplasia nodules, 7 follicular adenomas, 1 suture granuloma, and 1 Hashimoto's disease; size range 0.9 to 5 cm; mean 2.5 cm), and 51 were malignant (47 papillary carcinomas, 3 medullary carcinomas, and 1 metastatic carcinomas; size range 0.9 to 8 cm; mean 2.6 cm) (see Table 1). There was no significant difference in size between the benign and malignant nodules (p = 0.502).
Enhancement patterns and diagnostic value of CEUS
Enhancement patterns of the 104 thyroid nodules are listed in Table 2. The enhancement patterns of benign and malignant nodules were statistically different (p < 0.001). The benign thyroid nodules showed four enhancement patterns: ring enhancement 44/53 (83.0%), homogeneous enhancement 4/53 (7.5%), heterogeneous enhancement 4/53 (7.5%), and no enhancement 1/44 (1.9%). The malignant thyroid nodules showed three enhancement patterns: heterogeneous enhancement 45/51 (88.2%), ring enhancement 3/51 (5.9%), and homogeneous enhancement 3/51 (5.9%). Ring enhancement had a sensitivity of 83.0%, specificity of 94.1%, positive predictive value (PPV) of 93.6%, negative predictive value (NPV) of 84.2%, and accuracy of 88.5% for the detection of benign lesion. The heterogeneous pattern had a sensitivity of 88.2%, specificity of 92.5%, PPV of 91.8%, NPV of 89.1%, and accuracy of 90.4% for the detection of malignant lesions.
Hyperplastic nodule with old hemorrhage on pathological examination.
Chi-squared analysis comparing the enhancement pattern of benign lesions to malignant lesions.
Echotexture and enhancement patterns
One cystic nodule showed ring enhancement. On pathologic examination this proved to be goiter with hemorrhage and cystic change. Of 41 mixed (cystic and solid) lesions, 31 were benign and 10 were malignant. Twenty-seven of the 31 mixed benign nodules (87.1%) showed ring enhancement. Eight of the 10 mixed malignant nodules (80.0%) showed heterogeneous enhancement. Of 62 solid nodules, 21 were benign and 41 were malignant. Sixteen of the 21 benign solid nodules (76.2%) showed ring enhancement, 37 of the 41 malignant solid nodules (90.2%) showed heterogeneous enhancement (Tables 3 and 4).
In mixed cystic and solid thyroid nodules, ring enhancement as a criterion for benignity showed sensitivity, specificity, PPV, NPV, and accuracy of 87.1%, 80.0%, 93.1%, 66.7%, and 85.4%, respectively. Heterogeneous enhancement as a criterion for malignancy showed sensitivity, specificity, PPV, NPV, and accuracy of 80.0%, 96.8%, 88.9%, 93.8%, and 92.7%, respectively.
In solid thyroid nodules, ring enhancement as a criterion for benignity showed sensitivity, specificity, PPV, NPV, and accuracy of 76.2%, 97.6%, 94.1%, 88.9%, and 90.3%, respectively. Heterogeneous enhancement as a criterion for malignancy showed sensitivity, specificity, PPV, NPV, and accuracy of 90.2%, 85.7%, 92.5%, 81.8%, and 88.7%, respectively.
Interreader variability in classification of enhancement
In 100 out of 104 thyroid nodules (96.2%), the two readers agreed with each other on the classification of enhancement patterns. In the remaining four nodules with disagreement, the variation in differences included homogeneous, ring, and heterogeneous patterns. The coefficient was 0.93 for the enhancement patterns. There was good interreader agreement, especially for the classification of enhancement patterns.
Discussion
The thyroid gland has abundant microvasculature, and the parenchyma of normal thyroid shows rapid uniform enhancement after the intraveneous (i.v.) injection of SonoVue. Nodules differ from the normal vascular structure, and hence their enhancement differs from that of the normal parenchyma (8). Four enhancement patterns were observed in our study (i.e., homogeneous, heterogeneous, ring, and absent enhancement).
The most meaningful finding in our study is that ring enhancement can identify a benign thyroid nodule with high sensitivity (83.0%) and specificity (94.1%). Ring enhancement is probably associated with capsular and peripheral compressed parenchymal vessels around the lesion. The correlation between CEUS findings and histological structures needs to be studied in the future. The most common enhancement pattern for malignant nodules is heterogeneous enhancement with high sensitivity (88.2%) and specificity (92.5%).
The one category of lesions in which malignancy can be confidently excluded by imaging features alone comprises those that are purely cystic with no solid component and no intrinsic flow on power Doppler sonography (11,12). The one cystic nodule in our study showed ring enhancement and at histology was hyperplasia associated with cystic degeneration and hemorrhage.
Most mixed nodules are benign, with a reported incidence of malignancy of about 14% (13). In our study 10 of 41 mixed nodules (24.4%) were malignant. It can be difficult to diagnose a mixed nodule by conventional US. The microvasculature features provided by CEUS may be helpful. Our results suggest that nodules showing enhancement are more likely to be benign, whereas nodules that show heterogeneous enhancement are more suspicious, and thus fine-needle biopsy should be recommended.
Solid nodules are more likely to be malignant (11,14). In our study 41 of 62 solid nodules (66.1%) were malignant. Additionally, it should be noted that when the cystic component of a mixed nodule was very small (i.e., 1 to 2 mm), the pattern of enhancement could be homogenous. The three nodules in our study with these small echo-free areas that showed homogeneous enhancement were benign.
The enhancement patterns of CEUS in solid thyroid nodules provided valuable information. Our study found that in solid nodules, ring enhancement was strongly associated with a benign diagnosis (PPV 94.1%) and heterogeneous enhancement was associated with malignancy (PPV 92.5%). Research of enhancement patterns of thyroid nodules is at an early stage. There is no established standard for the patterns of enhancement so far, and thus it is difficult to compare the results of different studies. In our study, only one benign thyroid nodule showed no enhancement, a goiter with old hemorrhage, whereas microbubble echoes could be detected from all the malignant solid nodules. However, in the study by Bartolotta et al. (8) from September 2003 to July 2004, 4 out of 13 malignant nodules showed no enhancement. The reason for the difference in findings could be that the imaging technique of CEUS has improved or that calcification in a thyroid nodule may affect CEUS imaging.
Pathological changes and angiogenesis are the fundamental reasons for different CEUS patterns (15). The differences in CEUS patterns of thyroid nodules may reflect differences in perfusion between benign and malignant nodules. The mechanism may be that the growth of malignant nodules is more heterogeneous than that of benign nodules and that the blood distribution is more imbalanced, with areas of rich and poor microvasculature coexisting. Additionally, malignant nodules contain regions of complicated morphological collagen degeneration, which have either no small vessels or vessels whose caliber is so small that microbubbles cannot enter, resulting in heterogeneous enhancement. For thyroid nodules, heterogeneous enhancement should be an indication for fine-needle aspiration or core biopsy to confirm the diagnosis.
Conclusion
In conclusion, this initial study suggested that CEUS enhancement patterns were different in benign and malignant lesions, and that ring enhancement was very helpful to identify benign lesions, whereas heterogeneous enhancement was helpful to detect malignant lesions. CEUS has been shown to potentially be a valuable adjunct to baseline conventional US in the characterization of thyroid nodules. This study was a preliminary exploration of CEUS in the thyroid lesions, and the results need to be assessed by further research in the field.
Footnotes
Acknowledgments
This study was supported by a grant from the National Hi-Tech Research and Development Scheme (National 863 Project; 2006AA02Z4B3). The authors thank Department of Surgery in PUMCH for their valuable help and encouragement. We also thank Drs. Weisheng Gao and Yuewu Liu for their contribution of subjects and Dr. Patrick O'Kane for editing the article.
Disclosure Statement
The authors declare that no competing financial interests exist.