
Abstract
Background:
Intratracheal goiter manifestations caused by ectopic thyroid tissue have occasionally been reported. We report a 42-year-old female who had undergone thyroid surgery twice, which had caused unilateral recurrent laryngeal nerve palsy.
Summary:
The patient presented with progressive dyspnea. Magnetic resonance imaging showed a recurrent goiter growing through the tracheal wall. She was treated in a multidisciplinary approach; at first she underwent transtracheal laser surgical removal of the intratracheal mass followed by conventional completion thyroidectomy and radioiodine remnant ablation. Thorough histological analysis did not find any signs of malignancy. Currently the patient is disease- and complaint free. As far as we could ascertain, no patient with a recurrent benign goiter growing through the tracheal wall has been reported before.
Conclusion:
Recurrent benign goiter with intratracheal growth is extremely rare and requires a multidisciplinary approach.
Introduction
Intratracheal growth of thyroid tissue has been previously reported (2 –4); however, these reports concerned patients with ectopic thyroid tissue without physical contact with the thyroid. Alternatively, aggressively growing differentiated or anaplastic thyroid carcinoma may infiltrate and eventually break through the tracheal wall (5). Here we report a patient with a recurrent benign goiter that grew through the tracheal wall.
Patients
A 41-year-old female was referred to our hospital with complaints of dyspnea and a suspicion of recurrent goiter. She had undergone a subtotal thyroidectomy for benign goiter twice at ages of 21 and 36. As a complication of these procedures she had recurrent laryngeal nerve palsy on the right side. She had taken levothyroxine, but only intermittently, to prevent goiter recurrence. Otherwise the patients' history was unremarkable.
On initial presentation we saw a healthy 41-year-old female. Physical examination revealed a thyroidectomy scar and an inspiratory stridor. Thyroid parameters at the time of presentation showed subclinical hypothyroidism (thyrotropin [TSH]: 7.1 mU/L [normal range 0.3–4.0], free triiodothyronine: 5.5 pmol/L [normal range 2.7–7.6], free thyroxine: 16.6 pmol/L [normal range 11.0–23.0]), elevated thyroglobulin levels (102 μg/L), and undetectable calcitonin levels. Thyroid peroxidase- and thyroglobulin antibodies were also not measurable.
Ultrasound of the neck showed a 5 mL thyroid remnant on the left side and 8 mL on the right side. A hypoechoic lesion was not clearly separated from the trachea on the left side. For this reason magnetic resonance imaging with gadolinium was performed. Imaging demonstrated that the thyroid had clearly broken through the tracheal wall and obliterated more than 50% of the tracheal lumen (Fig. 1), leaving an open airway measuring 9 × 6 mm over a length of approximately 2.5 cm. An ultrasound-guided fine-needle aspiration biopsy was taken from this lesion that showed diffuse, degeneratively altered thyrocytes consistent with the diagnosis of a thyroid nodule with regressive changes.
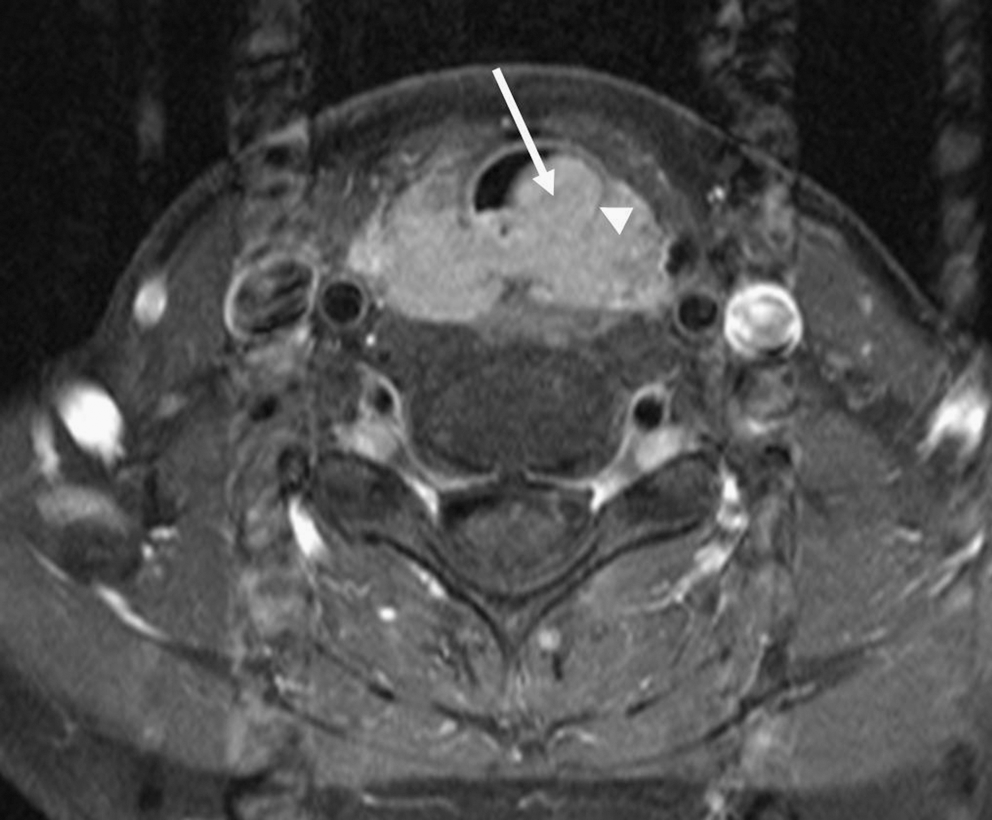
Contrast-enhanced transverseT1-weighted turbo spin-echo magnetic resonance imaging of the neck obtained with fat saturation (thickness 4 mm) depicts strong and homogeneous contrast enhancement of the thyroid mass breaking through the tracheal wall (arrow). The thyroid mass complete encircles the left tracheal cartilage (arrowhead).
Subsequently intratracheal debulking was performed using laser surgery followed by thyroidectomy, leaving 3 mL (ultrasound measurement after surgery) of thyroid tissue on the left side to spare the remaining recurrent laryngeal nerve. Histology from both procedures showed findings of diffuse and nodular goiter with regressive changes as well as microadenomatose hyperplasia without signs of malignancy (Fig. 2).
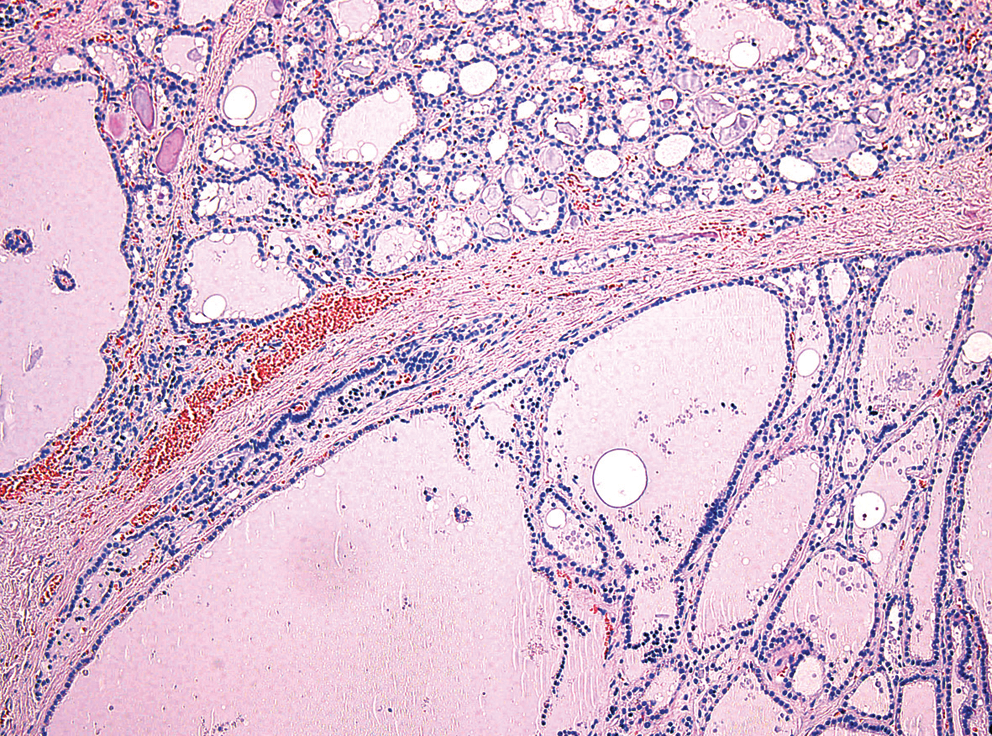
Representative detail of the resected thyroid tissue showing the typical morphological picture of a diffuse and nodular goiter with the coexistence of dilated follicles lined by flattened epithelium and smaller follicles (hematoxylin and eosin, 100×). Color images available online at
To prevent a future goiter recurrence the patient was subsequently treated twice with a total of 1363 MBq (37 mCi) I-131 to achieve thyroid remnant ablation, as well as put on a TSH-suppressive therapy with 175 μg of levothyroxine per day. On follow-up the patient was complaint free and euthyroid.
Discussion
As far as we could ascertain, this is the first report of a patient with intratracheal growth of a benign goiter originating outside of trachea. Previous reports of intratracheal goiter mostly concerned growth of ectopic thyroid tissue without a connection to the thyroid itself (4), unlike the current patient in whom the extrathyroidal origin of the intratracheal goiter component was clearly established on magnetic resonance imaging.
Recurrent goiter is a familiar phenomenon for any clinician in the field of thyroidology. Several factors may contribute to the occurrence of recurrent goiter.
The first contributing factor is the surgical technique. Whereas subtotal thyroidectomy may result in recurrence rates up to 40% (6), total thyroidectomy in one group led to only 10 of the 3044 patients requiring surgery for recurrent goiter (7). It has to be considered, however, that total thyroidectomy may carry a somewhat greater risk of complications such as recurrent laryngeal nerve palsy (8).
In the case of subtotal or near-total thyroidectomy, most recurrences will occur in the thyroid bed itself, whereas with total thyroidectomy nearly all recurrences will occur in the pyramidal or thyrothymic tract (7). This illustrates an important cause of recurrent goiters: remnants of embryonic thyroid development may give rise to new sites of thyroid tissue growth after thyroidectomy. Pyramidal tract tissue may give rise to goiter tissue occurring anywhere between the base of the tongue and the thyroid bed (9). Ectopically located intratracheal tissue may cause intratracheal goiter with potentially life-threatening airway obstruction (4). And embryonic thyroid remnants along the thyrothymic duct may well be responsible for a number of intrathoracic goiter recurrences (9 –11).
The level of thyroidal iodine availability and the levels of expression of local growth factors such as transcription growth factor beta 1 (12) have been reported as important factors in goiter growth; further molecular biologic data that may explain why some goiters progress to rapid and/or large reccurences after prior thyroid surgery were unfortunately not found in the literature.
In the present patient the main risk factors for goiter recurrence were the two subtotal thyroidectomy procedures. Perhaps contributing to the goiter recurrence in this patient was the subclinical hypothyroidism, indicative of either insufficient prior care or lack of patient compliance. Management of this patient was complicated by the preexistent recurrent laryngeal nerve palsy on the right side, making a radical surgical removal of the affected left thyroid lobe highly undesirable in the absence of malignant thyroid pathology. Therefore, adjuvant I-131 therapy was used to eradicate any remaining functioning thyroid tissue.
Infiltration of the trachea is a feature almost exclusively associated with a poor prognosis of differentiated thyroid carcinoma (5,13); surgery may be associated with extensive surgical morbidity. In that light it has to be considered that a pathologic misdiagnosis of benign goiter is a possibility in spite of extensive work-up of the resected material. Should this have been the case, the patient has already received adequate treatment in the form of I-131 remnant ablation and TSH-suppressive levothyroxine therapy.
To our knowledge no patient with histologically benign goiter breaking through the tracheal wall has been reported in literature so far. The cause of this breakdown of the tracheal wall can only be speculated about. This patients does, however, illustrate that an intratracheal thyroid lesions need not always be malignant.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.