
Abstract
Background:
Pediatric thyroid cancer differs from adult thyroid cancer in presentation and outcome. Pediatric thyroid cancer has a higher recurrence rate and greater percentage of lymph node and pulmonary metastasis. The clinicopathologic characteristics of pediatric thyroid cancer according to the histologic subtype have not been reported, however. In this study, we determined the histological subtypes of pediatric thyroid cancer and analyzed other clinicopathologic characteristics.
Methods:
All patients with thyroid cancer who were admitted to Severance Hospital, Seoul, South Korea, were retrospectively reviewed; their age was <20 years at diagnosis, and they were seen between January 1995 and August 2008.
Results:
Sixty-eight patients were identified. The histologic types of thyroid carcinoma were papillary thyroid carcinoma (PTC) in 57 (83.8%), follicular carcinoma in 8 (11.8%), and poorly differentiated carcinoma in 3 (4.4%). There were 28 (41.2%) cases of diffuse sclerosing variant of papillary carcinoma (DSVPC), 26 (38.2%) of conventional PTC, 2 (2.9%) of follicular PTC, and 1 (1.5%) cribriform-morular PTC. In patients with PTC, there was a higher incidence of bilateral thyroid involvement (p = 0.003), extrathyroidal extension (p = 0.009), and lymph node involvement (p = 0.018), and lower recurrence-free survival (p = 0.032) in DSVPC than in non-DSVPC. Univariate regression analysis revealed that extrathyroidal extension (p = 0.025) and tumor size (p = 0.001) were positively associated with a shorter time to recurrence.
Conclusion:
DSVPC is a major subtype of PTC in the young.
Introduction
Despite an overall survival rate of >95% (3 –7), pediatric patients with thyroid carcinoma have more frequent recurrences (7,8) and a higher prevalence of lymph node and pulmonary metastasis (7). The prognostic factors in pediatric thyroid carcinoma have been poorly evaluated. Papillary or papillary–follicular histology (6) and age (3) have been significantly associated with time to recurrence after initial surgical treatment in the young. Although the histologic subtype and age are important prognostic factors in pediatric thyroid carcinoma, the clinicopathologic characteristics according to histologic subtype have not been investigated. We studied a series of pediatric patients who underwent thyroid surgery for thyroid cancer at our institution. We examined the histopathological material to determine the relative frequencies of the subtypes of papillary thyroid carcinoma (PTC) and analyzed the clinical features of the subtypes.
Materials and Methods
Patients
All patients with thyroid carcinoma who were <20 years of age and underwent surgery at Severance Hospital from January 1995 to August 2008 were retrospectively reviewed. This study included only thyroid follicular epithelial cell neoplasm, and excluded nonfollicular epithelial cell neoplasm such as medullary carcinoma. The study was approved by the Institutional Review Board of Yonsei University Severance Hospital. Clinical data were obtained from patients' medical records and included age at diagnosis, extent of surgery, postoperative radioactive iodine therapy, disease recurrence, metastasis, follow-up status, and length of follow-up. Disease recurrence or metastasis was defined as evidence of new or progressive lesions detected clinically or by imaging studies after operation of initial thyroid cancer. All data were given as mean ± standard deviation.
Pathologic examination
Formalin-fixed, paraffin-embedded tissue blocks were used to prepare slides. Hematoxylin and eosin–stained sections were reviewed by two pathologists (J.S. Koo and S.W. Hong). Thyroid cancer was classified by the criteria defined by the World Health Organization for malignant tumors (9). Pathologic parameters such as size, lymph node involvement, extrathyroidal extension, and presence of lymphocytic thyroiditis were recorded and analyzed.
Statistical analysis
Data were analyzed using SPSS for Windows, version 12.0 (SPSS Inc., Chicago, IL). To determine statistical significance among thyroid carcinoma subtypes regarding various parameters, Student's t and Fisher's exact tests were used for continuous and categorical variables, respectively. Differences were accepted to be statistically significant at p < 0.05. Kaplan–Meier survival curves and log-rank statistics were employed to evaluate time to tumor recurrence. Multivariate regression analysis was performed using Cox proportional hazards model.
Results
Clinicopathologic characteristics of pediatric thyroid carcinoma
Table 1 shows the clinicopathologic characteristics of 68 patients with pediatric thyroid carcinoma. There were 59 (86.8%) female patients and 9 (13.2%) male patients. The age of patients at the time of diagnosis of thyroid carcinoma ranged from 4 to 19 years (15.5 ± 3.8). Tumor size was 2.3 ± 1.2 cm (range, 0.2–7.0 cm). In 22 patients (23.4%) both thyroid lobes were involved, and 46 (67.6%) patients had thyroid cancer in unilateral thyroid lobe. The types of thyroid carcinoma were PTC in 57 (83.8%), follicular carcinoma in 8 (11.8%), and poorly differentiated carcinoma (insular carcinoma) in 3 (4.4%).
PTC, papillary thyroid carcinoma.
The clinicopathologic characteristics of pediatric PTC are as follows. The subtypes of PTC were conventional type in 26 patients (45.6%), diffuse sclerosing in 28 patients (49.1%), follicular type in 2 patients (3.5%), and cribriform-morular type in 1 patient (1.8%). Tumor size was 2.2 ± 1.2 cm, and extrathyroidal extension was observed in 42 (73.7%) patients. Lymph node metastasis and distant metastasis occurred in 45 (78.9%) and 3 (5.3%) patients, respectively. The site of distant metastasis was lung in all three cases. Duration of follow-up was 54.7 ± 40.9 months and tumor recurred in 16 (28.1%) patients during follow-up.
Clinicopathologic characteristics of pediatric diffuse sclerosing variant of papillary carcinoma
Table 2 demonstrates a comparison of clinicopathologic characteristics between diffuse sclerosing variant of papillary carcinoma (DSVPC) and non-DSVPC in patients with PTC. The size of DSVPC tumors was 2.5 ± 1.3 cm. Although this mean was greater than that of non-DSVPC tumors, the difference was not significant (p = 0.052). The ages of the DSVPC and non-DSVPC patients were similar (p = 0.971). In male patients, there was a greater prevalence of DSVPC than of non-DSVPC (p = 0.039). Compared with non-DSVPC, there was a greater prevalence of bilateral thyroid involvement (p = 0.003), extrathyroidal extension (p = 0.009), lymph node involvement (p = 0.018), and the use of postoperative iodine therapy (p = 0.015) in DSVPC. There were a greater number of tumor-involved lymph nodes in DSVPC than in non-DSVPC (p < 0.001). The prevalence of lymphocytic thyroiditis was similar in DSVPC and non-DSVPC (p = 0.349). All three patients with PTC who had distant metastasis had DSVPC. The percentage of patients with recurrent tumors was greater in those with DSVPC than those with non-DSVPC, but this difference was not significant (p = 0.088).
DSVPC, diffuse sclerosing variant of papillary carcinoma.
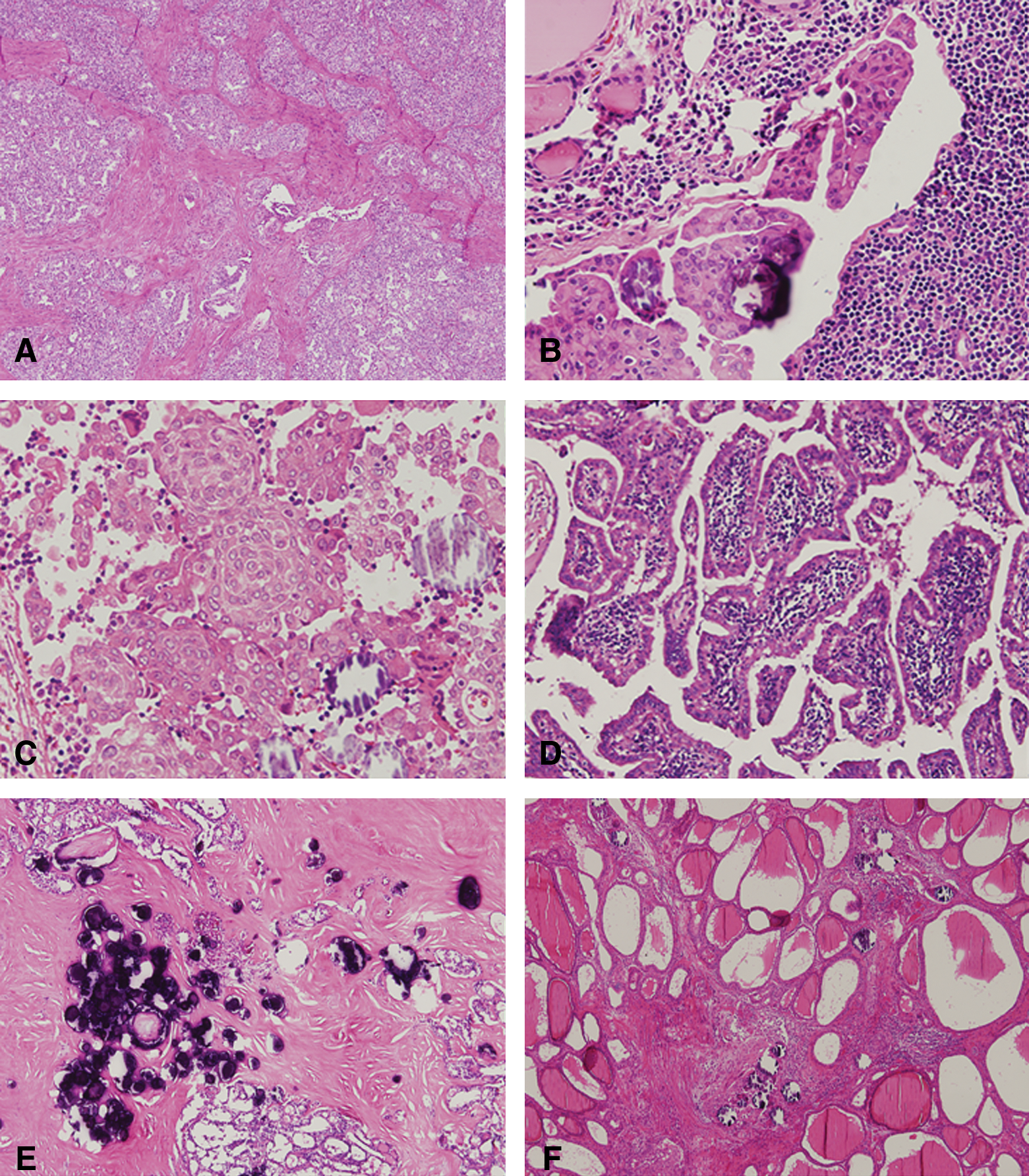
Histological features of DSVPC
Figure 1 shows the histological features of tumors in patients classified as having DSVPC. All cases had areas of conventional papillary carcinoma that revealed papillary architecture and characteristic nuclear features of papillary carcinoma. These areas of conventional papillary carcinoma merged with follicle-forming papillary carcinoma. Prominent fibrosis and sclerosis were observed in intratumoral areas with somewhat of a radiating pattern, creating a multinodular appearance (Fig. 1A). The histopathology of slides classified as DSVPC were characterized by multifocal tumor emboli in the lymphatic channel, forming micropapillary architecture (Fig. 1B). This feature was noted in the main tumor mass and surrounding normal-looking thyroid parenchyma. Tumor cells of DSVPC demonstrated extensive squamous metaplasia with varying degrees (Fig. 1C). This feature was frequently observed in tumor glands located in sclerotic stroma and lymphoplasmacytic infiltration. Lymphoplasmacytic infiltration was associated with DSVPC and formed lymphoid follicles in some areas, creating a warthin-like appearance (Fig. 1D). The large number of psammoma bodies was another characteristic of DSVPC. The psammoma bodies were noted in mainly sclerotic and fibrotic stroma (Fig. 1E). However, diffuse scattered psammoma bodies were observed in surrounding normal-looking thyroid parenchyma. Interestingly, two cases showed extensively scattered psammoma bodies in the diffuse sclerotic and fibrotic background involving the entire thyroid lobe with hardly identifiable papillary carcinoma cells (Fig. 1F). Diffuse involvement of the thyroid lobe in the pattern of psammoma bodies and tumor emboli in lymphatic channel made it difficult to precisely evaluate tumor size. In this study, there was a trend for DSVPC to have dominant tumor mass in one thyroid lobe and diffuse scattered psammoma bodies and tumor emboli in the lymphatic channels of the other thyroid lobe.
DSVPC. (
Clinicopathologic factors relating to tumor recurrence and time to recurrence
The results of univariate analyses of clinicopathologic factors on tumor recurrence in the total pediatric thyroid carcinoma group revealed a statistical significance in only two parameters, tumor size (p = 0.001) and extrathyroidal extension (p = 0.025). There was no relationship in other parameters, age (p = 0.657), sex (p = 0.288), lymph node involvement (p = 0.100), or histologic subtype (p = 0.195), with tumor recurrence in the 68 patients with thyroid cancer.
The results of univariate regression analyses of clinicopathologic factors on time to recurrence in the total pediatric thyroid carcinoma group revealed a statistical significance in two parameters, extrathyroidal extension (p = 0.005) and tumor size (p = 0.002) when tumor size was analyzed as a categorical (<1, 1–4, and >4 cm) variable. However, multivariate Cox regression analysis revealed no significant association. Age (≤10 years vs. >10 years; p = 0.366), sex (p = 0.256), lymph node involvement (p = 0.204), and histologic type (p = 0.251) were not associated with time to recurrence in this study population.
When univariate regression analysis of clinicopathologic factors on time to recurrence was performed in only pediatric papillary carcinoma, there was a statistical significance in three parameters, histologic subtype (DSVPC vs. non-DSVPC; p = 0.032), extrathyroidal extension (p = 0.032), and tumor size (<1, 1–4, and >4 cm; p = 0.002). However, multivariate Cox regression analysis revealed no independent significant variables. Figure 2 shows Kaplan–Meier estimates of recurrence-free survival between DSVPC and non-DSVPC.
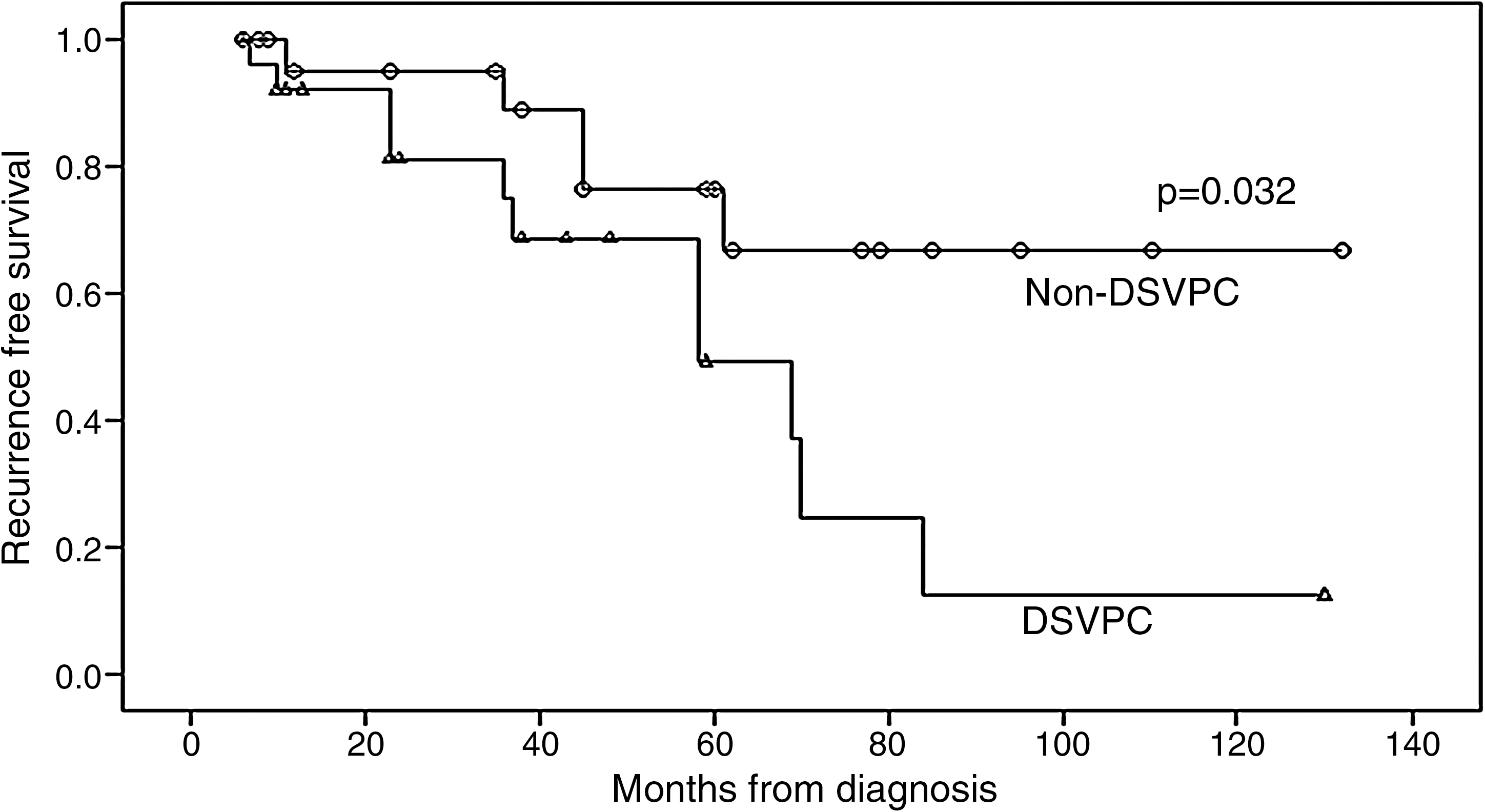
Recurrence-free survival according to histologic subtype in papillary thyroid carcinoma.
Discussion
Generally, pediatric thyroid carcinoma shows different tumor characteristics compared with adult thyroid carcinoma. Pediatric thyroid carcinoma has larger tumor size and higher incidence of lymph node metastasis, lung metastasis, and tumor recurrence than adult thyroid carcinoma does (7,8). However, paradoxically, the prognosis of patients with pediatric thyroid carcinoma is much better than that of adults (3 –7). Namely, pediatric thyroid carcinoma demonstrated aggressive tumor presentation and excellent prognosis, but the reason for this discrepancy could not be explained until now. Zimmerman et al. suggested that this was related to the high incidence of nondiploid DNA contents in adult thyroid carcinoma compared with pediatric thyroid carcinoma (7). Another possible reason is that pediatric thyroid carcinoma is more dependent on thyroid-stimulating hormone; therefore, postoperative thyroid-stimulating hormone suppression with thyroid hormone replacement is more effective, and dedifferentiation from well-differentiated to poorly differentiated carcinoma does not often occur in pediatric thyroid carcinoma (10).
Previous studies (1,3 –8,11 –13) of pediatric thyroid carcinoma are collectively summarized in Table 3. In our study, the male-to-female (M/F) ratio of pediatric thyroid carcinoma was 1:6.5, which showed more female predominance than the previous reports, in which the range was 1:1 to 1:3.3. In addition, the rate of extrathyroidal extension in our study (67.6%) was higher than that of the previous studies (14.6–42.1%). However, the rates of papillary carcinoma (83.8%), lymph node involvement (69.1%), tumor recurrence (23.5%), and metastasis (4.4%) were similar to those of previous studies. One important result of our study is that DSVPC (49.1%) was the most prevalent subtype of pediatric papillary carcinoma. The previous literature on pediatric thyroid cancer did not include a precise classification of tumors. The most prevalent type of pediatric thyroid cancer was papillary carcinoma; however, histologic subtypes of papillary carcinoma were not evaluated in detail in most studies (1,3,4,6 –8,11 –13). Harach and Williams (5) did report, however, that PTC in children under the age of 15 showed 42% of classical type, 33% of childhood (solid/follicular) type, 10% of DSVPC, and 6% of oxyphil type.
When DSVPC was compared with conventional papillary carcinoma, it showed similar predilection for female sex, younger age at tumor presentation, and higher incidence of cervical lymph node involvement and lung metastasis (14 –19). In our study, compared with the pediatric non-DSVPC group, DSVPC demonstrated bilateral involvement (p = 0.003), extrathyroidal extension (p = 0.009), lymph node involvement (p = 0.018), and increased number of tumor-involved lymph nodes (p = 0.000) with statistical significance. Additionally, all three cases with lung metastasis were DSVPC. One of the reasons that DSVPC was associated with extended disease status is probably the widespread scattered tumor emboli in the intrathyroidal lymphatic channels, which are a characteristic pathologic feature of DSVPC. The DSVPC cases in our study were generally characterized by one thyroid lobe having a dominant tumor mass and the surrounding thyroid parenchyma having multiple tumor nodules and lymphatic tumor emboli. Two cases of DSVPC in our study had widespread scattered psammoma bodies with hardly identifiable carcinoma cells. Therefore, careful examination is required to ascertain the presence of tumor involvement in these cases. It has been reported that there is no difference in the M/F ratio of DSVPC and conventional papillary carcinoma (14,18). In our study, the M/F ratio of DSVPC was 1:3.7 and that of non-DSVPC was 1:28, showing a relative female predominance in non-DSVPC. The prevalence of DSVPC among all papillary carcinomas in all age groups has been reported to range from 0.7% to 5.3% (15). We noted that 49.1% of pediatric papillary carcinoma patients had DSVPC. This is consistent with studies that the mean age of patients with DSVPC at presentation ranged from 18.0 to 34.7 years (14,16 –19), which is about 10–30 years younger compared with that of conventional papillary carcinoma (45–50 years). Notably, patients with DSVPC had larger tumor size and more bilateral neck lymph node involvement likely leading them to seek medical attention at a younger age. This alone is unlikely to explain the higher prevalence of DSVPC in pediatric papillary carcinoma. Radiation exposure, iodine content for diet, familial predisposition, and associated syndromes such as familial polyposis syndrome in the cribriform morular type of papillary carcinoma could be possible contributing factors. DSVPC has been reported to have no BRAF mutation but has RET/PTC rearrangements (20). In other reports, childhood PTC in general was characterized by a relatively high prevalence of RET/PTC rearrangements with predominance of RET/PTC type 1 rearrangements (21,22).
There is no consensus on the prognosis of DSVPC. In one report, DSVPC had a relatively poor prognosis as its disease-specific death rate of 3.6% was higher than the 0.6% of pure PTC (23). In other reports, however, the 5- and 10-year survival rates of DSVPC were 95% (19) and 93% (17), respectively, a survival similar to conventional PTC. In our study, although recurrence-free survival rate of DSVPC was lower than that of non-DSVPC (p = 0.032), there was no difference in overall survival rate. However, the follow-up (mean, 55 months) in our study was probably too short to assess survival.
In conclusion, our study showed that DSVPC is a major subtype of PTC in the young. In the pediatric population with PTC, the prevalence of bilateral thyroid involvement in DSVPC is higher than in non-DSVPC, as is extrathyroidal extension and lymph node metastasis. Further, the recurrence-free survival rate is lower in DSVPC than in non-DSVPC. Therefore, we recommend aggressive surgical treatment and close follow-up in DSVPC in the young because of these features.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.