
Abstract

Procalcitonin (PCT) is a precursor peptide from the hormone calcitonin (CT) (1). In the absence of infection, PCT is almost exclusively produced by neuroendocrine C cells of the thyroid before being processed to mature CT and stored in secretory granules (2). Microbial infection induces a ubiquitous PCT release from parenchymal tissues and differentiated cell types throughout the body (3). Several studies have identified PTC levels as indicators of the prognosis in sepsis and demonstrated that the levels of plasma PTC can provide useful information in assessing the response to treatment (4 –6). The advantage of PCT measurements over other established markers of infection (e.g., leukocyte count and C-reactive protein [CRP]) is that they are relatively specific for bacterial and fungal infections and minimally influenced by operative trauma (7). Therefore, plasma PCT measurements are being increasingly used in intensive care units (ICUs), especially in the postoperative setting.
Medullary thyroid carcinoma (MTC) is a tumor of neuroectodermal origin accounting for about 10% of all thyroid cancers (8). CT is an established marker of MTC (9). It is known that PCT and PCT cleavage products may be significantly elevated in patients with MTC (10 –12). Therefore, the absolute levels of PCT in plasma may be increased in patients with MTC even in the absence of infection. As the following case demonstrates, however, plasma PCT can be used for monitoring the course of an infection in patients with MTC, in spite of their MTC-related high plasma levels of PCT.
A 53-year-old man was treated in another hospital by total thyroidectomy and three-field lymphadenectomy for advanced MTC. He had infiltration of the left lobe of the thyroid, bilateral cervical lymph-node metastases, and infiltration of the recurrent nerve on the right side. Additionally, mediastinal lymph-node metastases and multiple liver metastases in both lobes were present. On postoperative day 6 a cervical revision was performed because of a lymphatic fistula. The remaining postoperative course in the other hospital was otherwise uneventful. Preoperative CT levels were reported to be markedly elevated to 10.5 ng/mL (normal value, <0.01 ng/mL). The patient was discharged from the hospital on postoperative day 8.
One day later, the patient was admitted to our ICU with dyspnea, faint pulse, and hypotension. He received oxygen and had fluid resuscitation on the way to the hospital. On admission he had pale extremities and faint peripheral pulses. Clinical chemistry revealed a partly compensated metabolic acidosis with a pH of 7.261 and a paCO2 of 20.5 mm Hg, elevated retention parameters (creatinine, 4.4 mg/dL [normal range, 0.7–1.3 mg/dL]; blood urea nitrogen, 30 mg/dL [normal range, 7–18 mg/dL]), elevated transaminases (alanine transaminase, 1458 U/L [normal range, 10–50 U/L]; aspartate transaminase, 1704 U/L [normal range, 10–50 U/L]), derailed coagulation (international normalized ratio 1.9; activated partial thromboplastin time 66 seconds [normal range, 26–37 seconds]), low platelets (40 G/L [normal range, 150–450 G/L]), elevated leukocyte count (17.07 G/L [normal range, 4.0–9.0 G/L]), and a high plasma CRP (24.7 mg/dL [normal value, <0.5 mg/dL]) consistent with severe sepsis. Notably, a markedly elevated plasma PCT level of 358.7 ng/mL (normal value, <0.5 ng/mL) was measured. For determination of plasma PCT, the Elecsys BRAHMS PCT automated electrochemiluminescence assay (BRAHMS AG, Henningsdorf, Germany) for the Roche Cobas e-System (Roche Diagnostics, Basel, Switzerland) was used.
A computed tomography scan on admission showed postoperative phlegmonous alterations in the thyroid bed, but no clear septic focus. Bilateral pleural effusions that did not require drainage were also noted. Empirical antibiotic and symptomatic treatment for sepsis was started. Initially, there was a further increase of plasma PCT to a maximum of 674.7 ng/mL on day 1 after admission. Thereafter, plasma PCT levels gradually declined (Fig. 1). Swabs taken on admission from the operation wound showed Staphylococcus aureus. The antibiotics were changed to cefuroxime/clindamycin after tests results for microbial resistance were returned. On the 3rd day after admission, an increasing redness spreading from the area of the operating-wound to the upper thorax and both arms could be observed. Another computed tomography scan showed growing enlargement of the right sternocleidomastoid muscle and an increasing pleural effusion on the right side. Operative revision of the cervical wound was performed the same day. The intraoperative swabs from this operation again showed S. aureus. Histological examination of the tissue specimens taken during the operation showed a phlegmonous-purulent inflammation consistent with a necrotizing fasciitis. After the operation the plasma PCT concentrations dropped markedly from a preoperative value of 432.7–274.4 ng/mL on the first postoperative day. The plasma CT concentration on day 4 after admission, measured by a solid-phase, enzyme-labeled, two-site chemiluminescent immunometric assay at a Immulite 2000 System (DPC, Los Angeles, CA), was elevated to 6.7 ng/mL (normal value, <0.01 ng/mL). The plasma CRP concentrations were determined during the first 5 days after admission. They appeared to follow, with a 1 day lag, the pattern for plasma PCT.
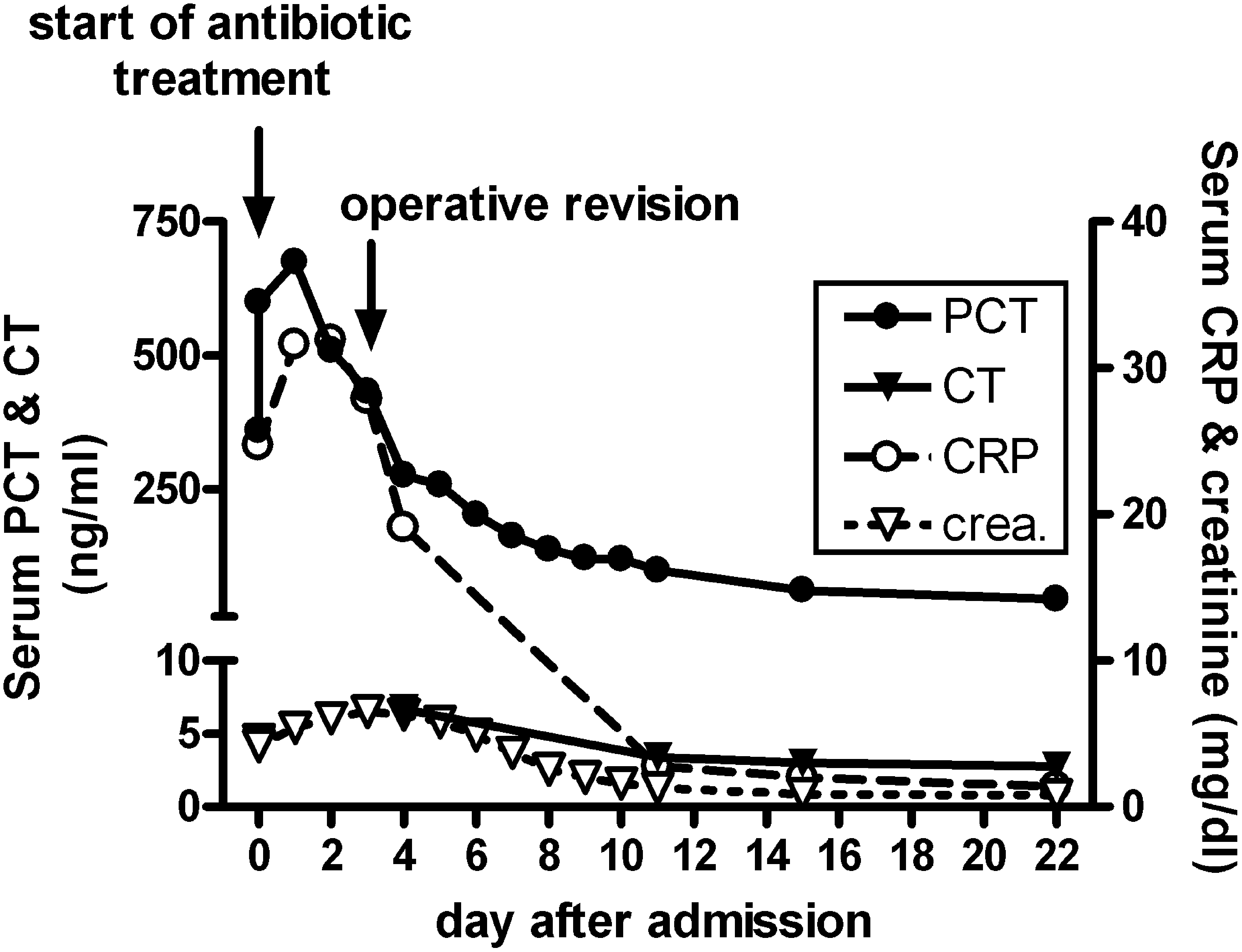
Course of plasma procalcitonin (PCT), C-reactive protein (CRP), and plasma creatinine during hospital stay.
After this the course was uneventful and stepwise removal of the wound-drains and chest-tube was performed. The patient's renal function recovered and, in parallel, PCT and leukocyte counts declined further. The patient was transferred off the ICU on day 11 and discharged 21 days after admission. At the time of discharge the plasma PCT concentration was 97.6 ng/mL, and plasma CT had declined to 3.4 ng/mL. The decline in plasma CT was attributed to improved renal function (see plasma creatinine in Fig. 1).
After an infectious stimulus, plasma PCT levels rise sharply with a latency of 2 hours, reaching peak values within 12–24 hours in the form of a plateau. After 48–72 hours the values slowly start to decline (4,13,14). Plasma PCT has a half-life of approximately 20–24 hours (4,15), and this is hardly prolonged in patients with impaired kidney function (14,16), thereby providing an adequate diagnostic window for a routine clinical use. Unlike other established markers for systemic infection like leukocyte count, blood sedimentation rate, and CRP, plasma PCT levels are only minimally influenced by operative trauma. A sterile surgical wound does not provide a sufficient stimulus for PCT induction, but major operations or intestinal procedures may trigger a rise in plasma PCT. However, even after extended surgery, including abdominal surgery, only moderately elevated PCT values rarely exceeding 2 ng/mL have been noted (17,18). These characteristics make plasma PCT a competitive marker for monitoring treatment of an infectious focus (7).
In patients with MTC, CT levels have been found to correlate with the tumor load (19), and postoperative levels >0.5 ng/mL are indicative of metastatic disease (20). In addition, the CT prohormone PCT and PCT cleavage products were found to be significantly elevated in patients with MTC, and a tendency of the PCT/CT ratio to augment with higher CT levels was observed (10 –12). Notably, the PCT produced during septicemia is reported to be slightly smaller in size than the PCT produced in MTC patients. While in MTC patients intact PCT(1-116) is processed into CT(1-32), katacalcin C-terminal flanking peptide (PDN-21), and N-terminal flanking peptide (PAS-57), in septicemia, PCT(3-116) is the predominant protein product together with 8 and 10 kDa PCT fragments that presumably occur through N-terminal truncation (12). The automated PCT assay used for analysis of the present case is a sandwich electrochemiluminescence assay based on monoclonal antibodies against epitopes on PDN-21 and CT epitope. Hereby, a streptavidin-coupled monoclonal antibody against the PDN-21 epitope and a ruthenium-marked monoclonal antibody against the CT epitope are employed. Consistent with data reported by Ittner et al. (12), commercially available assays will detect not only PCT(3-116) and the 8 and 10 kDa cleavage products released in septicemia, but also intact PCT(1-116) and the 6 kDa fragment found in MTC patients (Fig. 2).

PCT and PCT cleavage products in patients with medullary thyroid carcinoma (MTC) and septicemia detectable by commercially available assays.
Considered together with the findings of the present study, these observations suggest that PCT can also be used for monitoring infections in MTC patients, because the tumor load and therefore the production of CT and its prohormones can be expected to remain stable over a certain period of time. However, it has to be considered that there is an offset in plasma levels due to PCT produced by the tumor, independent from the PCT derived from an infectious focus.
The patient presented in this report exhibited a high preoperative calcitonin level of 10.5 ng/mL and showed a severe MTC tumor burden in the staging work-up. Therefore, it can be assumed that the tumor load was only partly removed by the debulking operation, consistent with a still significantly elevated plasma CT of 2.8 ng/mL at discharge. Bihan et al. reported a PCT/CT ratio of 7.6 in MTC patients (10). Therefore, an offset in plasma PCT of roughly 21 ng/mL could be expected in the present case, which is still well below the PCT plasma level of 43.2 ng/mL measured at discharge. However, Bihan et al. also observed a tendency for the ratio of PCT to mature CT to augment as mature CT levels became higher. In a patient with advanced metastatic disease PCT levels more than 42-fold greater than those of mature CT were found (10). In spite of exceptionally high plasma levels, PCT followed the clinical course of the patient. Remarkably, plasma CT also dropped after admission, even though tumor load could be expected to remain stable during that time. Since CT is eliminated renally, however, this can be attributed to the improvement of kidney function during the hospital stay: the patient exhibited a significantly impaired calculated glomerular filtration rate of 15 mL/min on admission, which had reached normal values again (>60 mL/min) at discharge.
In conclusion, PCT can be used for monitoring infection and the efficacy of antimicrobial therapy in patients with MTC, in spite of the interfering PCT produced by the tumor, irrespective of the tumor burden. The offset in plasma levels resulting from tumor-derived PCT has to be considered, which may vary with the extent of the disease. Therefore, changes in plasma PCT levels rather than absolute values should be used to draw prognostic conclusions.
It has to be kept in mind, however, that this is a report of a single case and that further experience with the use of PCT as a marker for systemic infection in MTC patient is needed to draw definite conclusions. To our knowledge, hitherto, this is the only report dealing with this issue. For further information about state-of-the-art treatment of MTC the Management Guidelines of the American Thyroid Association should be consulted as a comprehensive review (21).
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.