
Abstract
Background:
Iodine intake is often measured by a surrogate measure, namely urine iodine excretion as almost all ingested iodine is excreted in the urine. However, the methods for urine collection and the reporting of the results vary. These methods, and their advantages and disadvantages, are considered in this article.
Summary:
There are two main ways in which urine can be collected for iodine measurement. The first is the collection of urine over a period, usually 24 hours. The second is the collection of a spot urinary sample. Urinary iodine values can be expressed as the content or concentration and reported without modification or as a function of creatinine in the same sample. The 24-hour urine for iodine measurement is often considered as the “reference standard” for giving a precise estimate of the individual iodine excretion and thereby iodine intake. As 24-hour collections are difficult to perform for large number of persons, single spot urinary samples are preferable to the 24-hour urinary collections in population studies. The iodine concentration in urine depends on the intake of both iodine and fluid. This, and the fact that there is a considerable variability in the daily iodine intake, makes the iodine measurement in spot urine samples unreliable for evaluating individuals for iodine deficiency, though they can be used to screen for exposure to large amounts of iodine from sources such as amiodarone and certain radiographic contrast agents. In populations of at least 500 subjects, the median value of spot urinary iodine concentration is a reliable measure of the iodine intake in the population as there is a leveling out of the day-to-day variation in iodine intake and urinary volume. Expressing the urinary iodide concentration as a function of urinary creatinine is useful in correcting for the influence of fluid intake. When doing so, it is recommended to adjust for the age- and sex-specific creatinine excretion in the given population.
Conclusion:
In studies of iodine intake, the correct choice of the method for collecting urine and the format for expressing the results of urine iodine measurement is essential to avoid misinterpretation of data on the iodine status of a population or individuals.
Introduction
It is cumbersome to reliably measure habitual iodine intake from foods and supplements in a large number of persons. UI measurements, however, are the most suitable methods for assessing dietary iodine intake. A relatively large fraction of iodine excretion is via the urine (4 –7). The minor portions are excreted in the feces, about 5–10%, and through perspiration (5,6,8). Iodine from ingested food initially circulates as iodide. After ingestion iodine is either excreted in the urine, mostly within 24 hours of ingestion, or taken up by the thyroid. If taken up by the thyroid it is incorporated into thyroid hormones but eventually excreted in the urine as thyroid hormones are secreted and degraded.
UI is typically measured in a pool of urine collected over a 24-hour period. At the start of the collection, the subject voids and that sample is discarded. Urine that is voided over the next 24 hours is pooled and the subject voids at the end of the 24-hour period and adds that sample to the pool. This pool represents the 24-hour urine sample, reflecting the renal production of urine during this period. The so-called “spot urine” is a sample collected during a single voiding. If 24-hour collection is used, the concentration of iodine is measured and the iodine content of the pool sample calculated and reported. If single spot urine sampling is used, the iodine concentration is measured and reported. In addition, the creatinine concentration of the urine can be measured and the iodine concentration reported as a function of the creatinine concentration. A further possibility discussed below is to use the measured iodine and creatinine in a spot urine to estimate the 24-hour iodine excretion using age- and sex-specific data for 24-hour creatinine excretion.
There has been an ongoing discussion on the correctness and suitability of the various measurements and methods for iodine estimation (9 –13). Each has advantages and disadvantages for different types of studies and study conditions (Table 1).
UI excretion may vary between seasons in some but not all healthy adults, children, and animals (14). In some cases this is most likely caused by a higher intake of iodine from milk in the winter (15,16). Milk is a rich source of dietary iodine especially in the winter, where iodine is added to the cattle feed. In the study of Als et al. (17), there was a larger seasonal variation in UI among children than their parents due, it was thought, to seasonal variation in iodine concentration in milk. Thus, in a population study, it is important to ensure that there are not likely to be seasonal variations in the iodine content of the diet of the population, or to perform urine sample collections across seasons.
UI Measurements
24-hour urine collections for iodine measurement
The 24-hour UI collection is considered the “reference standard” for the measurement of the iodine intake in an individual as it gives a more precise estimate than the spot urine collection. It is often used to validate other measurements of iodine intake (11 –13). A single 24-hour urine collection, however, is a poor index of habitual iodine intake since dietary iodine intake varies considerably from day to day. In individuals there may be as much as a threefold variation in day-to-day 24-hour UI excretion (11). Moreover, as may be apparent from the description of how the 24-hour pooled sample is collected, the collection is demanding and therefore the compliance rate is low. Thus, as an estimate of the iodine intake in a population, the collection of 24-hour urine is subject to selection bias, as only some individuals are able to carry out the collection properly. Even in the most committed participants, incomplete sampling occurs. Therefore, validation of the completeness of the 24-hour urine samples is desirable. One method of validation is the use of para-aminobenzoic acid (PABA), where recovery of PABA is measured in the urinary samples after ingestion of PABA tablets during the collection period (18). In our studies of 24-hour urine samples in which we employed PABA, 10% to 20% of the samples were excluded because they were not complete collections (11,19,20).
Spot urine collections for iodine measurement
In population-based studies of iodine intake, the reliable and feasible collection of the 24-hour urine samples is usually not possible. Therefore, spot urine collections are used. Collection of spot urine samples is far less cumbersome than the 24-hour urine collections, enabling a large number of individuals to be studied. The World Health Organization recommends that the median values of UI concentration (UIC) be used to report and evaluate the iodine status of a population (2). Thus, medians are used for primary reporting in most publications on iodine intake, including our own studies (19,20). It has been suggested by some investigators that mean UI excretion is a better measure of iodine status than median UI excretion in a population, at least as far as it is a determinant of thyroid status (21). It was reasoned that the thyroid is able to store iodine (in an organified form) and occasional intake of extra iodine by otherwise iodine-deficient individuals will benefit thyroid status and be better reflected by mean than by median UI excretion. However, if mean values are used, people with excessive iodine intake should be excluded; even a few samples with extraordinarily high values may considerably influence mean values and thus not reflect the iodine status of the whole population. To avoid this problem we advocate the use of median values for determination of the iodine status of a population.
Whereas the median iodine concentration in spot urinary samples is a suitable measure for the iodine nutritional status of a population, a single spot urine concentration cannot be used in studies of individuals. An exception is the clinical use of a spot urinary sample in screening for exposure to a large amount of iodine from an unknown source in a patient with low or absent thyroid uptake of isotope given for diagnostic purposes.
Though interindividual variation in iodine content exceeds the intraindividual variation (22), the latter is still very high (11,14,23,24). In fact, Andersen et al. (25) calculated that, for an individual estimate, at least 12 separate urine samples are needed for a precision range of ±20%. Both the inter- and intraindividual variations in spot urine iodine concentration are caused not only by differences in iodine intake but also by large variations in daily urinary volume. Interestingly, the mean daily urinary volume may differ considerably among populations. For example, a study from New Zealand found daily urinary volumes around 1.4 L in men and 1.3 L in women (26), whereas the Danish National Dietary Study demonstrated a daily fluid intake around 3.4 L suggesting daily urinary output above 2 L (11). These findings mean that the variation in urinary volume (as also reflected by the different creatinine concentrations in urine) may account for the major part of the differences between the subjects in the iodide concentration of the 24-hour urine samples. Pertinent to this is a study by Als et al. (13). They found, in a group of 13 subjects, that the variation in urinary volume and creatinine largely accounted for differences between the subjects in the iodide concentration of the 24-hour urine samples.
A further consideration in the use of spot urine samples for studies of iodine excretion is that there may be a diurnal variation in UIC. A considerable proportion of iodide absorbed from the gut after a meal is excreted in the urine within a few hours and dilution depends on the intake of fluid. Thus, the UIC varies over the day depending on the diet, and systematic differences in the median values depending on the time of collection have been observed in some studies. In particular, the iodide concentration in a fasting morning urine sample tend to be lower than the concentration in a 24-hour urinary collection (23,27).
Regardless of when the sample is collected, it is important to account for the differences in the time of urine collection when comparing data regarding iodine nutritional status. In particular, it should be recognized that using fasting morning urinary samples will give relatively lower values of iodine in all of the subjects. When samples are collected through the day in populations, this consideration is of minor importance as the possible effect will be reduced by the tendency of large numbers of participants to choose at random the time to collect their spot urine. It has been calculated that the spot UICs from more than 500 individuals are needed to describe the population iodine excretion with a precision range of ±5% (25). If subgroups of the population are studied in more detail (e.g. different age groups), each subgroup should optimally include 500 individuals or there will be a decrease in precision.
Using UICs in spot urine samples, it is also not possible to identify individuals or fractions of the population with iodine deficiency. A low iodine concentration might just represent the nadir value for the person and could be considerably higher on other days, or it might represent an individual with a habitual high fluid intake and consequently diluted urine. It is inappropriate, therefore, to conclude that because 20% of the population had UIC values below 50 μg/L, the prevalence of iodine deficiency in this population is 20%. It is best to remember that World Health Organization recommendations are almost always population based. For example, a statement that a UIC of >100 μg/L is consistent with iodine sufficiency is intended for the population as a whole, rather than individuals, and usually refers to the median value for the population. As noted, assessment of iodine sufficiency in individuals is difficult. At this time there are no well-established guidelines for measuring dietary iodine intake in individuals (25). This is in contrast to the solidly based literature and guidelines on the recommended dietary iodine intake for various segments of populations, most importantly, the iodine nutrition guidelines for pregnant women (2,28).
μg iodine/g creatinine ratio
To minimize the variation caused by variation in the urinary volume, use of the μg iodine/g creatinine ratio has been suggested (29), as creatinine is excreted at a relatively constant rate. However, in countries with low protein intake, the use of the μg iodine/g creatinine ratio will lead to overestimation of iodine intake compared with the 24-hour iodine excretion, due to low daily creatinine production and excretion (30). In industrialized countries, the use of creatinine to express results will lead to an underestimation of iodine excretion compared with the 24-hour iodine excretion in populations with low protein intake. Further, creatinine excretion varies considerably with sex, cultural or genetic background (see next section), and age (31). In a large study of the renal creatinine clearance in a Belgium population, Kesteloot and Joossens found a 1.5 times higher value in males than in females and a decline in creatinine excretion with age (32). Konno et al. demonstrated the same pattern with a steeper decrease with age in females, causing a distortion in the iodine excretion results if the simple iodine/creatinine ratio was used (9). The use of μg iodine/g creatinine ratio as a population measure accordingly is dependent on the representativeness of the sample in relation to the age and sex distribution in the population. Thus, the use of μg iodine/g creatinine ratio as an individual measure is doubtful. In fact, there is a poor correlation between μg iodine/g creatinine ratio and 24-hour iodine excretion (12,30,33). In some studies this was even poorer than the correlation between 24-hour iodine excretion and the UIC (30,33). In summary, the variation caused by dilution is diminished when introducing the correction for creatinine excretion. However, this introduces error related to variation in daily creatinine excretion among individuals. The variations related to creatinine excretion might be reduced considerably by stratifying the data for sex and age (see below) if reliable information is available.
Estimating the 24-hour UI excretion
An early recommendation was that the ratio of iodine to creatinine concentrations in urine as an estimate of the 24-hour urine iodine excretion could be improved by introducing a correction for sex (34,35); more recently a similar recommendation with both sex and age as factors to take into account has been made (12,14). In contrast to the large variation in creatinine between different age groups (32), there is little variation in urinary creatinine excretion within individuals and between individuals belonging to the same sex and age groups. This statement is more applicable to industrialized countries than to developing countries where correction for creatinine excretion among children may distort the results due to large individual variation in creatinine excretion (30). Clearly, the correction factor based on creatinine excretion depends on the population under study. This was emphasized by a study of a Greenland population, where the Inuit population had a lower creatinine excretion than an age-matched group of Caucasian Danes indicating genetic or cultural differences, the latter perhaps relating to dietary protein intake. This is another factor to be considered in the adjustment of UI excretion as it relates creatinine excretion (36).
In industrialized countries, the 24-hour UI excretion in adults can be estimated from spot urinary samples using expected 24-hour creatinine excretion as suggested by Knudsen et al. (Table 2) (12). The expected 24-hour creatinine excretion values used are based on a large Belgian population study (32). In the table some of the age groups from the original study have been combined as the differences are minor. The estimated 24-hour UI excretion is calculated as follows: iodine (μg/L)/(creatinine (g/L) × expected 24-hour creatinine (g/day). In a study including 112 24-hour urine samples from 31 Danish individuals, the estimated 24-hour UI correlated well with the 24-hour iodine excretion (r = 0.62). The estimated values, however, were slightly lower than the actual 24-hour collection values (p = 0.03) (12). This has since been confirmed in two other studies (11,20).
The relatively large spread in UICs in a population is reduced when an adjustment for age- and sex-specific creatinine excretion is done. This is suggested by Figure 1 comparing variation in crude UIC with variation in the estimated 24-hour iodine among 16 healthy males examined during a 12-month period (14). Moreover, the estimated 24-hour urine iodine excretion appears to be a superior predictor of the likelihood of stigmata of iodine deficiency. In a large population study performed as a part of the Danish Investigation of Iodine Intake and Thyroid Disease (DanThyr), the estimated 24-hour urine iodine negatively correlated with thyroid volume and prevalence of thyroid enlargement (p < 0.001), whereas this was not the case for UIC in spot urine samples (p = 0.4) (37).
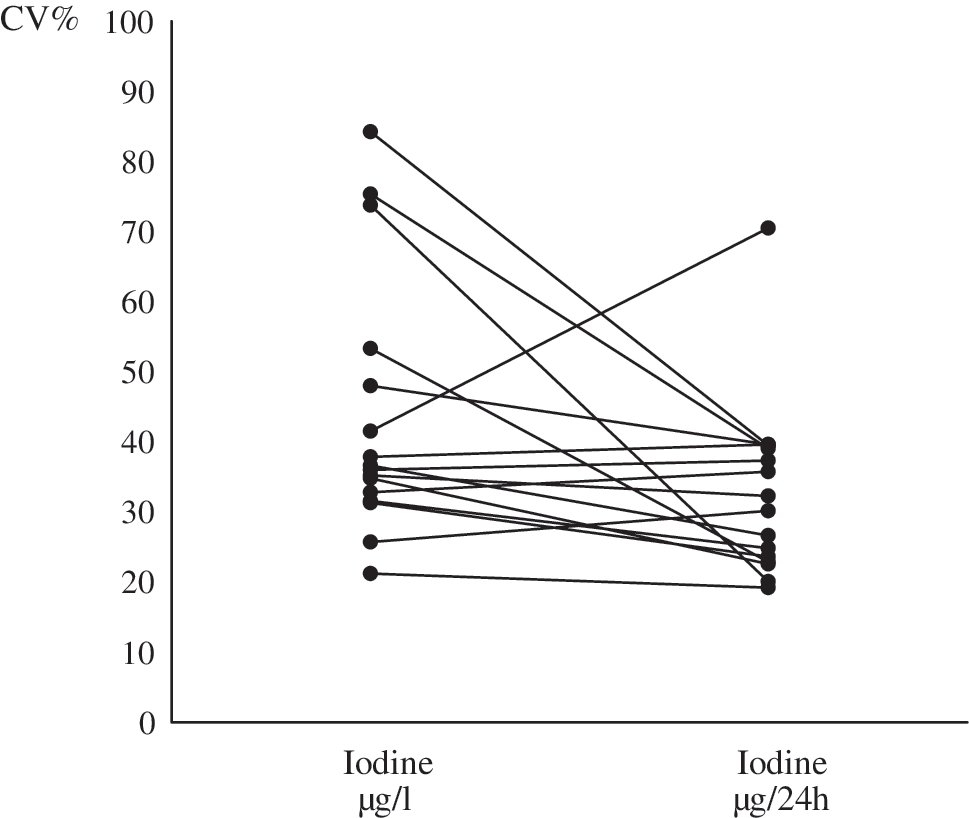
Comparison of the variation in two measures of urinary iodine (UI) excretion. A spot urine sample was collected monthly in 16 nonfasting healthy men. They lived in Randers, Denmark, an area with mild to moderate iodine deficiency. Iodine and creatinine concentrations were measured in each sample and 24-hour UI excretion estimated using the equation: (iodine concentration × creatinine concentration/24 hour creatinine excretion in age- and sex-matched individuals). In each individual, variation in UI concentration (dots to the left) and in the estimated 24-hour UI excretion (dots to the right) were calculated (CV% [coefficient of variance] of 12 monthly values: standard deviation/mean). Variation in the estimated 24-hour UI excretion was markedly lower than that of the UI concentration (34.9% vs. 47.3%, p < 0.01 by Bartletts test). Data are from reference (14).
In conclusion, the choice of a surrogate measure for iodine intake depends on the purpose of the study and is influenced by the subject and population characteristics. Though 24-hour urine iodine measurements might be appropriate in small groups as a more direct measure of iodine nutrition, and are also helpful to validate more indirect estimates of iodine intake, this method is difficult to carry out in population studies. For the estimation of the iodine intake in a population, the median iodine concentration from spot urinary samples is suitable provided there are at least 500 subjects in each group or, if the study uses subgroups, 500 subjects in each subgroup. If stratification of the population according to iodine excretion is desired, an estimate of the 24-hour iodine excretion adjusting for age- and sex-specific creatinine excretion is recommended. For individuals, there is a paucity of data regarding the best way to use urine measures to establish that a particular person is iodine deficient.
Footnotes
Acknowledgments
This study was supported by grants from the Copenhagen Hospital Cooperation Research Foundation, the 1991 Pharmacy Foundation, the Danish Medical Foundation, the Health Insurance Foundation, Tømmerhandler Vilhelm Bang Foundation, North Jutland County Research Foundation, and The Danish Food Industry Agency.
Disclosure Statement
The authors declare that no competing financial interests exist.