
Abstract
Background:
With the advent of the formaldehyde standard law in France, and because of the impact of new methods for diagnosis and prognosis in pathology, formalin replacement in surgical pathology laboratories is currently being discussed in France. However, a set of criteria must be assessed before introducing a formalin substitute fixative. The objective of this study was to compare formalin substitute fixation with formalin fixation and cryoconservation of tissues from several benign and malignant thyroid pathologies with respect to morphology, antigenicity, and nucleic acid (RNA, DNA, microRNA) integrity.
Methods:
Calibrated specimens (200 mg, 1 cm2 each) from four conventional papillary thyroid carcinomas, four follicular variant of papillary thyroid carcinomas, three minimally invasive follicular carcinomas, four thyroid adenomas, five thyroid nodular hyperplasias, and five normal thyroid tissues were fixed for 6, 12, or 24 hours, in different fixatives (formalin, Glyo-Fixx, FineFIX, ExcellPlus, RCL2) at room temperature or at 4°C. Tissues were stained (hematoxylin–eosin, periodic acid Schiff, trichromic Masson, and Sweet-Gordon staining) and their antigenicity determined by immunohistochemistry (performed with HBME-1, galectin-3, CK19, vimentin, CD31, and KL1 antibodies). Evaluation by four pathologists was made blinded. The quantity and quality of DNA, RNA, and two representative microRNA extracted from deparaffinized sections of paraffin embedded specimen were compared with that of cryosections.
Results:
The staining and morphology were not altered by the use of different fixatives. However, formalin, FineFIX, and RCL2 gave the best results for immunohistochemistry. Moreover, FineFIX and RCL2 gave the highest amount of nucleic acids and of the best quality.
Conclusions:
All the formalin substitute fixatives used in this study provided good histomorphologic quality for the different stained thyroid tissues, but individually, some fixatives performed better for immunohistochemical and molecular biological procedures for different thyroid pathologies.
Introduction
Recently, the potential carcinogenicity of formaldehyde has been emphasized (2 –4). In 2008, the formaldehyde standard became a law in France (5). This law alerted the staff of surgical pathology laboratories and hospital employers to this potential carcinogenicity of formaldehyde and has stimulated rapid changes in the practices of pathologists (2,3). Thus, it was recommended to French surgical pathologists that they choose a formalin substitute for tissue fixation. Formalin substitute fixatives contain an aldehyde component other than formaldehyde or no aldehyde component; thereby their use eliminates exposure of laboratory staff to formaldehyde. In addition, as the integrity of DNA, RNA, and protein is not always well preserved with formalin fixation procedures the use of formalin substitute fixatives also aims to improve the analytical molecular biology of fixed-tissues and paraffin-embedded specimens (6 –9). For this purpose, many companies have produced proprietary formalin substitute fixatives for use in surgical and molecular pathology. However, before systematically replacing formalin with these substitute fixatives for diagnosis in a surgical pathology laboratory, a number of aspects must be evaluated in comparison with formalin fixation and freezing. For this purpose, it is crucial to compare specimens of similar size and weight from the same organ and pathological condition, after fixation for the same duration and at the same temperature. Finally, assessment must include morphological, histochemical, and immunohistochemical approaches, as well as analytical molecular biology that controls for DNA and RNA integrity.
The aim of this study was to compare the use of formalin substitute fixatives (with different nonformalin aldehydes [Glyo-Fixx and ExcellPlus], without aldehyde and acetic acid [FineFIX], and without aldehyde but with acetic acid [RCL2] components), formalin fixation, and snap-freezing with nitrogen in maintaining the tissue morphology, antigenicity, and nucleic acid integrity of a set of nontumoral and tumoral calibrated thyroid specimens.
Materials and Methods
Thyroid specimens, fixatives, and tissue preparation
Thyroid specimens measuring 1 cm2 and weighing 200 mg each, corresponding to four conventional papillary thyroid carcinomas (C-PTCs), four follicular variant of papillary thyroid carcinomas (FV-PTCs), three minimally invasive follicular carcinomas (FCs), four microfollicular adenomas, five nodular hyperplasias, and five normal thyroid tissues, were collected after thyroidectomy from the Department of Otorhino-Laryngology (Pasteur Hospital, Nice, France). The time period for ischemia occurring during surgery was estimated to be quite similar (15–20 minutes) for the different samples. The time between surgical resection and fixation or frozen procedure was less than 30 minutes. For each thyroidectomy, a fresh sample was immersed in the appropriate fixative for 6, 12, or 24 hours, at room temperature or at 4°C. Five fixatives were used: neutral buffered formaldehyde 10% (formaldehyde 35%, m/m, diluted 1 vol: 5 vol in distilled water) (formalin) stored at room temperature (this fixative is routinely used for diagnosis in the Laboratory of Clinical and Experimental Pathology [Pasteur Hospital]), RCL2 (Alphelys, Paris, France), ExcellPlus (Microm Microtech France, Francheville, France), Glyo-Fixx (Thermo Electron Corporation, Cergy Pontoise, France), and FineFIX (Milestone, Sorisole, Italy). After fixation, the tissues were rinsed in 70% alcohol, processed on a VIP tissue processor (Thermo Electron Corporation), and embedded in a coded paraffin block. In addition, a sample from each specimen was snap-frozen in liquid nitrogen.
Staining and immunostaining
Paraffin blocks were sectioned at 4 μm for staining and immunostaining. The sections were stained with hematoxylin–eosin, periodic acid Schiff (PAS), Masson and Gordon-Sweet silver staining. For immunostaining, TTF1 (Dako, Copenhagen, Denmark; diluted: 1/100), HBME-1 (Ventana, Illrich, France; diluted: 1/100), galectin-3 (Dako; diluted: 1/100), CK19 (Ventana; diluted: 1/100), KL1 (Dako; diluted: 1/100), vimentin (Ventana; diluted: 1/100), and CD31 (Dako; diluted: 1/100) primary antibodies were used (45 minutes) and then the sections were incubated for 1 hour with a peroxidase secondary antibody (Dako; diluted: 1/100). Slides from each specimen were coded, scrambled, and presented blind to four surgical pathologists (S.L., V.H., C.B., and P.H.). The pathologists were asked to rate the following parameters: nuclear details, cytoplasmic details, erythrocyte integrity, overall staining, intensity (a scale of 0 to 3 was applied [0: absent; 1: faint; 2: moderate; 3: intense]), tissular distribution, and the percentage of positively immunostained cells (0%; <25%; 25–50%; >50%).
Nucleic acid quantity and integrity
For whole tissue sectioning and nucleic acid extraction, 20 sections of 10 μm in thickness, from either snap-frozen tissue or paraffin-embedded tissues, were cut on a Cryotome FSE (Thermo Electron Corporation) or a Microtome (Thermo Electron Corporation). Before nucleic acid extraction, the paraffin-embedded samples were deparaffinized in 1 mL xylene for 1 minute at 65°C and centrifuged for 2 minutes. After repeating this step thrice, sections were immersed twice in 1 mL of absolute ethanol to remove the xylene and then in 75% ethanol. After decanting the supernatant, sections were incubated in an appropriate buffer for DNA or RNA extraction.
DNA, RNA, and microRNA (miRNA) extraction: for DNA extraction, sections were incubated in 260 μL of proteinase K digestion buffer (50 mmol/L Tris, pH 8.1, 1 mmol/L ethylenediaminetetraacetic acid, and 0.5% Tween 20) containing 10 μL of proteinase K (10 mg/mL) at 56°C. After proteinase K digestion, DNA was extracted by phase separation by the addition of 260 μL of phenol–chloroform–isoamyl alcohol (25:24:1 ratio) and centrifuged for 15 minutes. The aqueous upper phase was collected and then extracted by the addition of 260 μL of chloroform–isoamyl alcohol (24:1 ratio). After ethanol precipitation (1/10 sodium acetate [0.3 M, pH 5.6] and 2.5 volumes of absolute ethanol), DNA was dissolved in 20 or 50 μL of Tris-HCL ethylenediaminetetraacetic acid (EDTA) buffer (10 mM Tris-HCL, 0.1 mM EDTA).
Equivalent volumes of frozen tissue were placed into 1 mL of proteinase K (Sigma-Aldrich, St. Louis, MO) solution (20 mg/mL) and digested overnight at 55°C followed by boiling at 94°C for 7 minutes. The DNA was isolated by phenol chloroform extraction as described earlier.
The yields of nucleic acid were determined using a Nanodrop ND-1000 UV spectrophotometer (Nanodrop Technologies, Wilmington, DE). The DNA integrity in the samples was assessed by gel electrophoresis (500 ng) and visualized by ethidium bromide staining. In parallel, the quality of the DNA from all the tissue preparations was compared by polymerase chain reaction (PCR) amplification. Approximately 50 ng of extracted DNA was used to amplify a 982-base pair (bp) fragment of the human glyceraldehyde-3-phosphate dehydrogenase (GAPDH) gene using the following primers: GAPDH forward: 5′-CAT GTG GGC CAT GAG GTC CAC CAC-3′, and GAPDH reverse: 5′-TGA AGG TCG GAG TCA ACG GAT TTG GT-3′, for 25 cycles of PCR. All samples were analyzed in duplicate.
RNA was extracted using the MagnaPure Compact RNA Isolation Kit (Roche, Paris, France) or using the Trizol procedure. Sections were incubated in 500 μL of lysis buffer (MagnaPure; Roche). After 30 minutes, the samples were centrifuged for 5 minutes at 17,000 g and 350 μL of supernatant was transferred to a MagnaPure automate (Roche). RNA was eluted in a final volume of 50 μL of kit buffer. The RNA extracted with the Trizol procedure was purified using a RNeasy MinElute Cleanup Kit (Qiagen, Valencia, CA) and DNase treatment was done with a Ambion TURBO DNA-free kit (Ambion, Austin, TX). The quality of the RNA was examined by capillary electrophoresis on an Agilent Bioanalyzer 2100 (Agilent, Palo Alto, CA) and Agilent 2100 Expert software was used to calculate the RNA integrity number of each sample. To check the integrity of the RNA, an RNA 6000 Nano Assay kit with 1 μL of RNA solution and an Agilent 2100 Bioanalyzer were used.
To assess the feasibility of performing miRNA techniques when using different fixative substitutes, we examined the accessibility of two representative miRNAs [one that is highly expressed in C-PTC (miR-222) and another one that shows the ubiquitous, but just moderate expression (miR-16)] by real-time quantitative PCR for C-PTC specimens. Briefly, total extracted RNA using Trizol procedure was quantified with the ND-1000 NanoDrop spectrophotometer (Nanodrop Technologies), resuspended in 20 μL of H2O, and treated with 30 U DNAse, 10 U RNase Inhibitor, both from Roche Diagnostics (Mannheim, Germany), for 30 minutes at 37°C. Human total RNA (35 ng) was reverse transcribed in a 10 μL volume using the Taqman miRNA reverse transcriptase kit (Applied Biosystems, Forster City, CA), according to the manufacturer's recommendations. Three microliters of the reverse transcription reaction was used in each of the real-time PCR assays using the Taqman miRNA Assay-kit (Applied Biosystems) following the manufacturer's instructions.
Data normalization and statistical evaluation
A standard curve of every assay in each run was generated to ascertain the specific amplification efficiency to avoid quantification bias. To determine the amount of miR-16, a dilution series of total RNA in five steps was performed. Fixation kinetics of thyroid specimens and experiments with different fixatives were normalized using miR-16 as a reference, and this was followed by calculating the specific calibrated miR-222 expression of each C-PTC sample. The mean values of normalized miR-222 levels of snap-frozen thyroid tissues or after 6 hours of formalin fixation served as calibrators, respectively. A Student's t-test was performed for statistical analysis of the data achieved by real-time PCR after testing the normal distribution with one-sample Kolmogoroff–Smirnov test. Values were expressed as the mean ± standard error of the mean of n number of experiments. A p-value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS 14.0.1 software (SPSS, Chicago, IL).
Results
Morphological analysis
Thyroid specimens fixed in different aldehyde-based fixative substitutes macroscopically looked like formalin-fixed tissues. In contrast, those fixed in nonaldehyde-based fixatives remained soft and turned red-brown. Glyo-Fixx- and FineFIX-fixed tissue blocks sectioned well after cooling, despite minor tissue contraction. The RCL2 and ExcellPlus-fixed tissue blocks sectioned moderately well after cooling. The overall effectiveness of each fixative was evaluated by microscopy and the formalin-fixed tissues gave the best results. The overall histological results for formalin were significantly better than those for RCL2 and ExcellPlus, and better than those for Glyo-Fixx and FineFIX, although the difference was not significant. All fixatives showed nuclear integrity, which leads to diagnosis of C-PTC and FV-PTC (Fig. 1A). All fixatives allowed assessment of capsule invasion by thyrocytes in minimally invasive FC. These results were obtained for the different times of fixation and for preparation at both room temperature and 4°C without major differences.
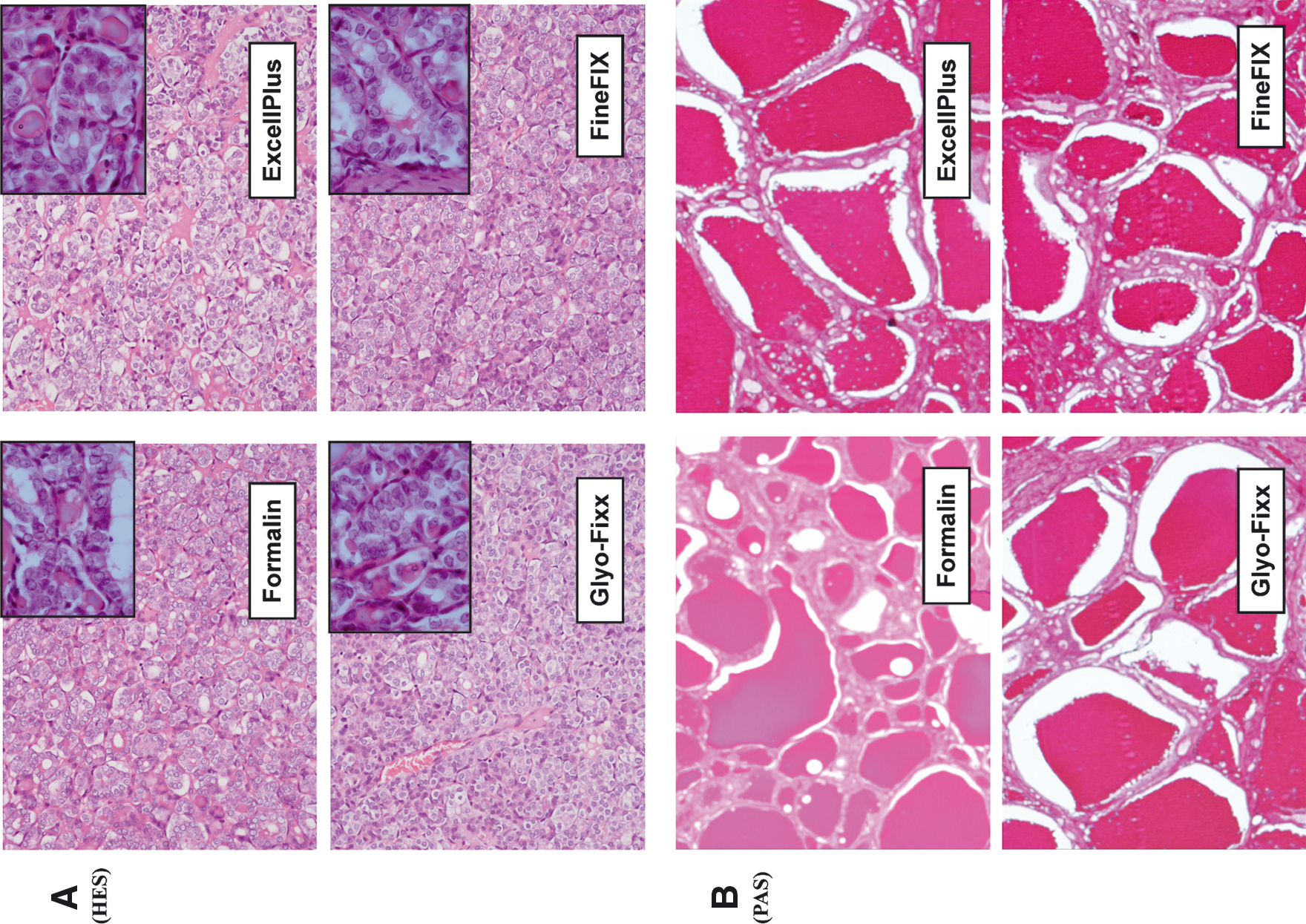
Histomorphologic assessment of different formalin substitute fixatives for diagnostic surgical thyroid pathology. (
Histochemical and immunohistochemical analysis
The morphological features of samples stained with PAS, Masson, or Sweet-Gordon silver staining were the same with all fixatives. However, nonaldehyde fixatives invariably showed a darker PAS coloration (Fig. 1B). For immunostaining, some fixatives were positive for some antibodies (HBME-1, CK19, KL1, CD31, vimentin), but gave a different score (Table 1). For a few antibodies (HBME-1, CK19, CD31), the scores were similar to those obtained with formalin fixation, whereas for others (CK19 and vimentin) the scores were lower when using Glyo-Fixx and ExcellPlus (Fig. 2). For some antibodies (TTF1 and galectin-3), certain fixatives (Glyo-Fixx and ExcellPlus) gave no signal for the different specimens used in our study (Fig. 2). The results were similar for different times and temperatures of fixation.
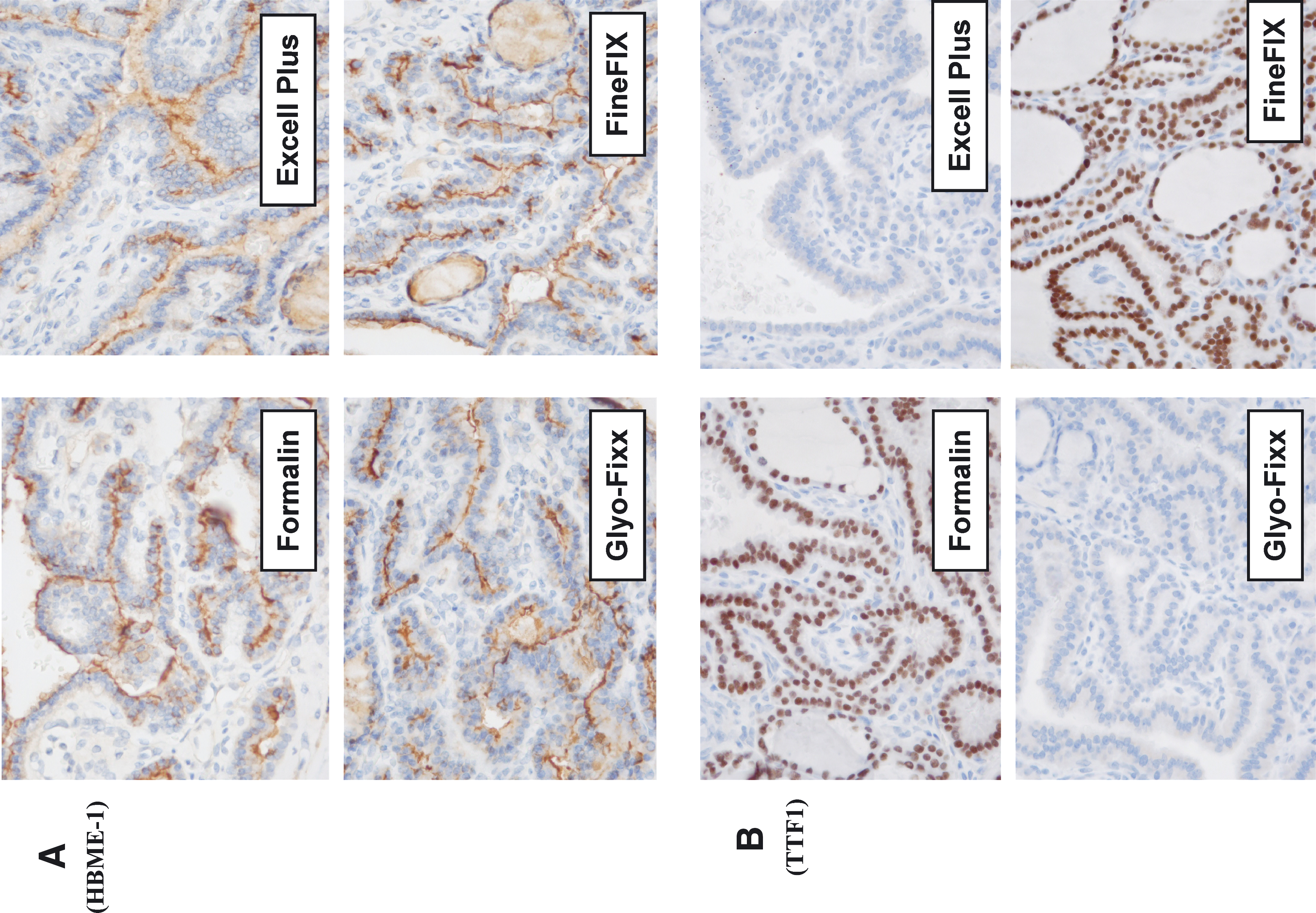
Immunohistochemical assessment of different formalin substitute fixatives for diagnostic surgical pathology. Immunohistochemistry with HBME-1 (
Nucleic acid integrity
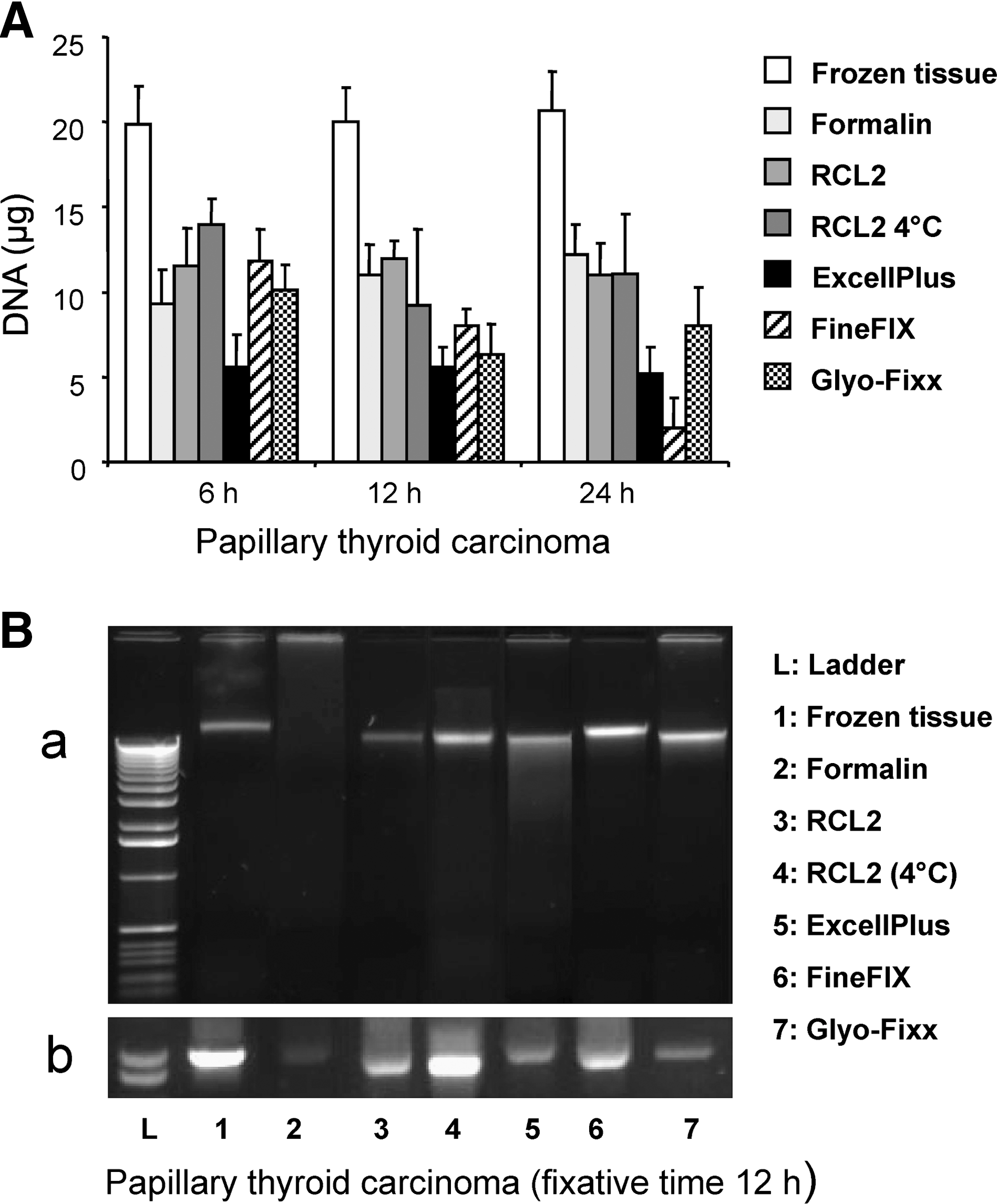
The quantity of DNA obtained from the different fixed samples was quite similar for the different fixatives, but always lower than that obtained from frozen samples. An example of a C-PTC is shown in Figure 3A. The quality of the DNA in the samples was assessed by gel electrophoresis and PCR amplification. A perfect migration pattern was observed from frozen samples without any signs of DNA degradation (Fig. 3B, lane 1). The DNA from the different substitute fixative fixed samples migrated on an agarose gel as a smear, showing fragments ranging in size from several hundred bp to a few kbp (Fig. 3B[a]). However, the quality of the DNA was superior to that recovered from formalin-fixed tissues. PCR amplification of the DNA from the substitute fixative fixed tissues consistently gave a stronger signal than that of formalin-fixed tissue (as an example, see Fig. 3B[b]). Similar results were obtained for the different specimens of the same category of thyroid pathology, and for the different pathologies fixed for 6, 12, or 24 hours at room temperature or at 4°C with the substitute fixatives used in this study (not shown).
(
The quantity of RNA was assessed by UV spectrophotometry and the concentration was given in micrograms. The aldehyde-based fixatives gave very low yields; the highest average yield (ExcellPlus) did not exceed 2.2 μg after 6 hours of fixation (Fig. 4A). While the average yield for Glyo-Fixx was approximately 15 μg after 6 hours of fixation, RCL2 gave an average yield close to 35 μg for the same fixative time. No statistically significant (p < 0.05) difference was found for the mean quantity of RNA for the different specimens after 12 and 24 hours of fixation; the quantity was much lower after 24 hours of fixation for all the fixatives used in this study. Similar results were obtained for the different pathologies fixed for 6, 12, or 24 hours at room temperature or at 4°C (Fig. 4A).

(
The quality of the isolated RNA is given as an example for a C-PTC specimen in Figure 4B and C. RNA from optimum cutting temperature (OCT)-embedded thyroid specimens was slightly fragmented, but gave distinct 28S and 18S peaks, although the ratio varied between 1.4 and 1.8 (Fig. 4B). Between and to the left of these peaks, the baseline was high, which indicated partially degraded RNA. Some RNA fragments were up to and above 6000 bases long, however, the majority of the RNA was of high molecular size. Of all the fixatives, RCL2 (at room temperature and at 4°C) yielded the most intact RNA, but it was more fragmented than that from OCT-embedded tissue. Peaks corresponding to 28S and 18S RNA were still apparent after 6 or 12 hours of fixation in RCL2 and FineFIX, but were considerably reduced for OCT-derived RNA (Fig. 4B). The majority of the fluorescence was observed between 400 and 3000 bases. In Glyo-Fixx the 28S peak was absent but a small 18S peak remained. The majority of the RNA was between 25 and 2000 bases. The RNA of formalin and ExcellPlus samples was the most fragmented, with broad spectra and without rRNA peaks, indicating that the majority of the fragments had sizes between 25 and 200 bases or were extensively fragmented. Finally, all specimens fixed for 24 hours showed highly fragmented RNA for all the fixatives used in this study. Estimation of the RNA integrity number, under the same conditions as those described in Figure 4A, showed that the RNA was preserved best in frozen specimens and in RCL2 fixative-fixed specimens fixed for 6 and 12 hours (both at room temperature and at 4°C) (Fig. 4C). Similar results were obtained for different cases of the same category of thyroid pathology and for different pathologies (not shown).
The amount of miR-16 in matched samples of snap-frozen and fixed specimens in different fixatives from a total of five patients with C-PTC was assessed (Fig. 5). miR-222 was chosen as a highly expressed miRNA in C-PTC. In the formalin-fixed and formalin substitute fixative-fixed tissues, the expression of both miRNAs closely mimicked that of snap-frozen tissue (Fig. 5). However, the miRNAs were preserved best in frozen specimens and in RCL2 fixative-fixed specimens fixed for 6 hours. We also compared fixation times of 6, 12, and 24 hours in formalin and in the other fixatives used in this study. We showed that the fixation in different fixatives for different time periods does not significantly alter the levels of miRNA expression in the PCR assay (Fig. 5). Fixation in nonformalin fixatives resulted in different miRNA yields, but was similar for each fixative and causes only slight variations in relative expression levels compared with buffered formalin fixation.

Formalin-fixed paraffin-embedded versus formalin substitute fixatives versus snap-frozen samples of C-PTC. (
Discussion
Currently, the morphological analysis of the phenotypic characteristics of diseased thyroid tissues is the basis of diagnostic thyroid pathology (1). Immunohistochemical analyses may also provide additional information on a routine basis (1,10). Because of the development of molecular biology, particularly PCR techniques, genetic profiling and gene expression of thyroid tissues have become part of routine analysis (1). More recently, microarray technologies have been developed in thyroid pathology, which increase the possibility of analyses of both gene expression and monitoring genetic changes (11 –14).
Despite the fact that several studies showed that methods in molecular biology can be applied to formalin-fixed tissues, a lot of these methods have been developed from frozen tissues (15 –18). However, frozen tissues are not always available in surgical pathology laboratories, and thus, some of these methods cannot be routinely developed. In this regard, the use of formalin substitute fixatives in a surgical pathology laboratory may increase the possibilities of developing molecular biology approaches for diagnosis and prognosis. Moreover, the replacement of formalin by substitute fixatives will reduce considerably the risk of exposure of the laboratory staff to the potential carcinogenicity of formaldehyde, a now well-documented genotoxic substance for human cells (19).
The number of available formalin substitute fixatives is considerable, but the main criteria for the choice of such a fixative should be always evaluated before using it in routine practice (see the list of criteria in Table 2). Moreover, to evaluate and compare the different fixatives it seems preferable to target a single organ and different nontumoral and tumoral pathologies of this organ. For this reason we studied different benign and malignant thyroid pathologies using calibrated tissue specimens (size and weight).
HE, hematoxylin–eosin.
Different categories of fixative are available to the surgical pathologists—formalin, other aldehyde-based fixatives (such as ExcellPlus and Glyo-Fixx), fixatives without aldehyde and acetic acid components (such as FineFIX, HOPE fixative, and Molecular Fix), the fixatives without aldehyde but with acetic acid (such as Hydrosafe and RCL2), and other fixatives made with different solutions comprising methanol, acetone, or chloroform (7,20 –30). Some studies have demonstrated that certain formalin substitute fixatives are potentially better than formalin when using molecular methods, whereas others are less efficient (31 –36). However, currently, the ideal fixative does not exist. Such a fixative, as well as being nontoxic, should preserve morphology and antigenicity to the same extent as formalin and should give results with molecular biology protocols that are similar to those obtained from frozen tissue. In this regard, each fixative has positive and negative attributes. Moreover, pathologists are more accustomed to examining formalin-fixed tissue sections and are less used to the morphological changes induced by other fixatives.
In this study, we examined a variety of thyroid specimens fixed with four formalin substitutes and compared the results with those obtained from formalin-fixed and frozen specimens. We used fixatives with different nonformalin aldehydes (Glyo-Fixx and ExcellPlus), a fixative without aldehyde and acetic acid (FineFIX), and a fixative without aldehyde but with acetic acid (RCL2). We did not use fixatives made with methanol, chloroform, or acetone because these solutions are toxic and have to be used at low temperature. To perform a strict comparison, we took care to select similar thyroid specimens (weight and size) from different pathologies and used similar times of fixation, both at room temperature and at 4°C. Moreover, we took different cases of the same category of thyroid pathology and for different pathologies to check the reproducibility of the results. Gross examination showed that nonaldehyde-fixed thyroid specimens were paler and softer than formalin, Glyo-Fixx, and ExcellPlus-fixed thyroid specimens. However, the capsule and the edge of different thyroid nodules were always observed, allowing accurate selection of the specimens of interest for microscopic examination. The selection on gross macroscopic examination of small tumors (such as papillary thyroid microcarcinoma or medullary thyroid microcarcinoma) is less convenient with nonaldehyde-containing fixatives. Moreover, these fixatives are also less convenient when building tissue microarrays because of the difficulty of setting up different core tissue in new paraffin blocks. Microscopically, no significant alteration in tissue morphology was noted. Particularly, the characteristics of nuclei, one of the most important criteria in making the diagnosis of frequently detected thyroid neoplasms (C-PTC, FV-PTC, and thyroid tumors of uncertain malignant potential) were similar for different fixative-fixed specimens. Moreover, invasion of the capsule in FC was easily observed in all fixative conditions, without induced fixation artifacts. The results of histochemical staining were quite similar for different fixatives. However, further comparative work should be performed using a larger panel of staining protocols (such as those used for mucosecretion and pathogen detection). Immunohistochemical comparison using the main antibodies currently used for epithelial thyroid tumors diagnosis showed major differences for different fixatives. Particularly, the immunostaining for TTF1 and galectin-3 gave negative results when using ExcellPlus and Glyo-Fixx. Moreover, some fixatives gave a fainter signal on immunostaining. FineFIX or RLC2 fixation gave excellent immunostaining in comparison to formalin fixation for all the antibodies used in this study. This is important because the diagnosis of some primary and secondary thyroid tumors can sometimes be largely oriented when using antibodies such as those to TTF1 (10,37). Interestingly, the time and temperature of fixation used in this study did not alter the immunostaining.
The integrity of nucleic acids was not the same for the different fixatives and was always lower then that obtained for frozen specimens. Moreover, some formalin substitute fixatives, FineFIX and RCL2, gave better results than those obtained with formalin, Glyo-Fixx, and ExcellPlus. This was accentuated when specimens were fixed at 4°C. However, the RNA integrity was always low after 24 hours of fixation for all fixatives. The RNA integrity varied substantially for nonaldehyde- and aldehyde-containing fixatives. Fragmentation of RNA was always present in the different specimens fixed in formalin and Glyo-Fixx, under all conditions of fixation. ExcellPlus also gave a substantial amount of fragmented RNA. In contrast, fixation for 6 hours with RCL2 and FineFIX at 4°C gave the best results. This could be important for the application of certain molecular biology analyses requested for thyroid specimens. However, in a surgical pathology laboratory, it is not convenient to fix specimens for a short period of time and at 4°C. Finally, in the study presented herein, we demonstrated that miRNA accessibility was not affected by prolonged formalin fixation during routinely performed tissue processing, confirming the results of a previous study (38). Moreover, our data reveal that the accessibility of miRNA from formalin-fixed thyroid tissues and from the specimens fixed in different alternative fixatives used in this study was comparable to snap-frozen material. The time of fixation up to 24 hours did not significantly alter miRNA detection by real-time PCR.
Alternative fixatives to formalin can deliver better results than formalin in terms of RNA quality or detection of specific expression markers. However, we found that the formalin substitute fixatives used in this study gave different results with different thyroid pathologies. This is particularly marked for immunohistochemistry and RNA integrity. In this regard, we believe that further studies are needed to (1) extend these experiments to a larger panel of stains and antibodies, (2) compare results from different surgical pathology laboratories, and (3) repeat these experiments on the same tissue blocks used for the initial evaluation but after a few months (at least 1 and 2 years after), because different biomarkers may be lost with time (39). We feel strongly that before replacing formalin with another fixative in a surgical pathology laboratory, different criteria of evaluation must be examined to maintain the high standard of diagnosis that is required to determine appropriate treatment. The cost of formalin substitute fixatives must also be taken into consideration. Moreover, we have to keep in mind that even though most of these substitutes are less toxic than formalin, they always contain components that are potentially toxic for humans and are also inflammable. Finally, the present study demonstrated that the best way to validate a new formalin substitute fixative is to target a single organ and a representative pathology using calibrated specimens, because the methodological conditions and criteria are numerous and hence evaluation is expensive and time consuming.
Footnotes
Acknowledgment
The authors thank Ms. Rollin (Thermo Corporation, Paris, France) for her help.
Disclosure Statement
The authors declare that no competing financial interests exist.