
Abstract

We read with interest the recent publication by Ozekinci et al. (1) in the September, 2009 issue of Thyroid. They reviewed 800 thyroidectomy specimens from two Turkish hospitals to ascertain the prevalence of thyroid tuberculosis (TB) and noted that TB was present in five, most with probable primary TB. Their report details the histopathological features of TB in the thyroid. Here we report a patient with the clinical features of this rare condition.
A 64-year-old man was referred to our hospital, with a preliminary diagnosis of thyroid carcinoma. His medical history was negative except for a painless swelling in the neck for about 2 years duration. There was a palpable, solid, 4–5 cm mass in the left lobe of the thyroid, which was fixed to the surrounding tissue. Thyroid function tests and other biochemical parameters such as erythrocyte sedimentation rate, C-reactive protein, white blood cell, and liver function tests were normal. Neck ultrasonography showed marked enlargement of the left thyroid gland due to multiple nodules throughout. The largest nodule was 6 × 3.5 cm and contained microcalcifications. Neck computed tomography showed a 49 × 27 × 69 mm nodule in the left thyroid gland, with borders indistinguishable from the surrounding soft tissues (Fig. 1). Fine-needle aspiration of the nodule was performed three times and all of the samples were read as colloid goiter. A left lobectomy and partial right lobectomy were performed because a medial nodule in the right lobe was identified during surgery. Histopathological examination revealed a granuloma with central caseating necrosis surrounded by epithelioid histiocytes in the thyroid tissue and lymphocytes located in the periphery of the granuloma (Fig. 2A). Hematoxylin–eosin-stained sections examined under 40 × magnification showed individual thyroid follicles with centrally located Langhans-type giant cells in areas of fibrosis and inflammation with lymphocytes (Fig. 2B). A diagnosis of thyroid TB was made on the basis of the histopathological criteria for TB. Purified protein derivative skin test was negative and chest X-ray, thoracic and vertebral computed tomography, sputum and blood cultures did not show evidence of systemic TB. As the thyroid lesion had been completely removed surgically and these tests were negative, no anti-TB medications were given. Eighteen months after thyroid surgery the patient was doing well without evidence of TB.
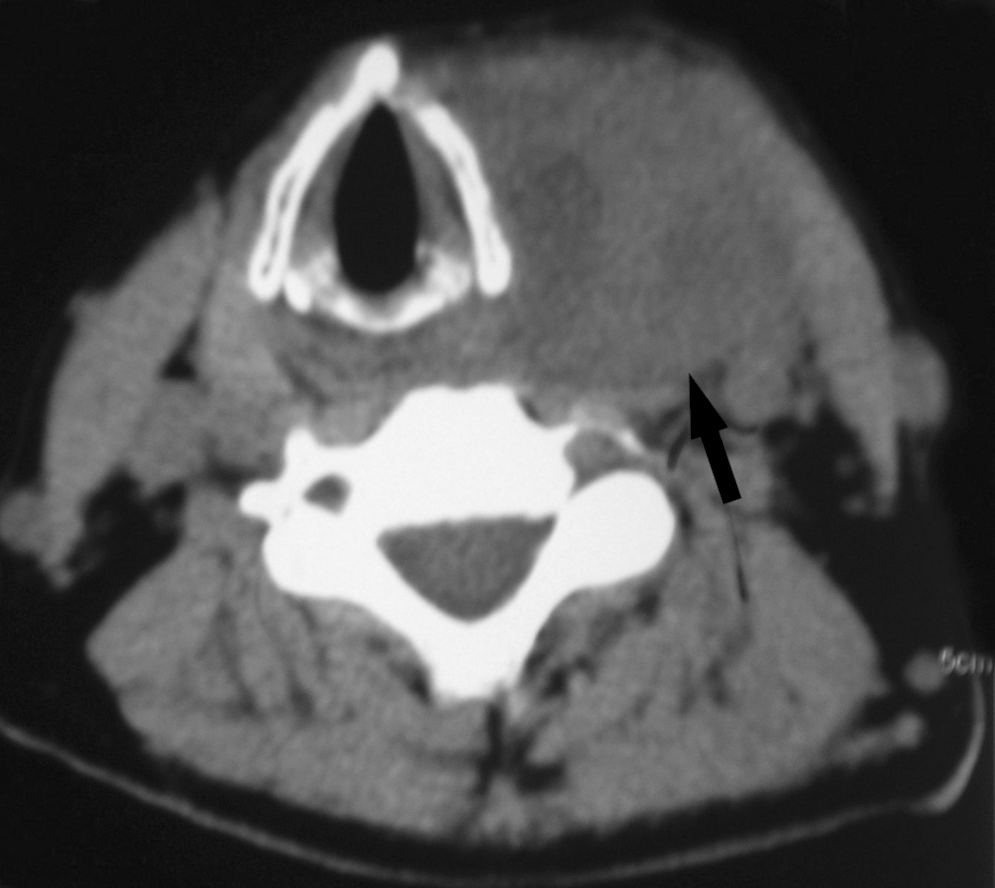
A 49 × 27 × 69 mm heterogeneous soft tissue mass is seen in the left neck on computed tomography. The mass causes the sternocleidomastoid muscle to deviate laterally.
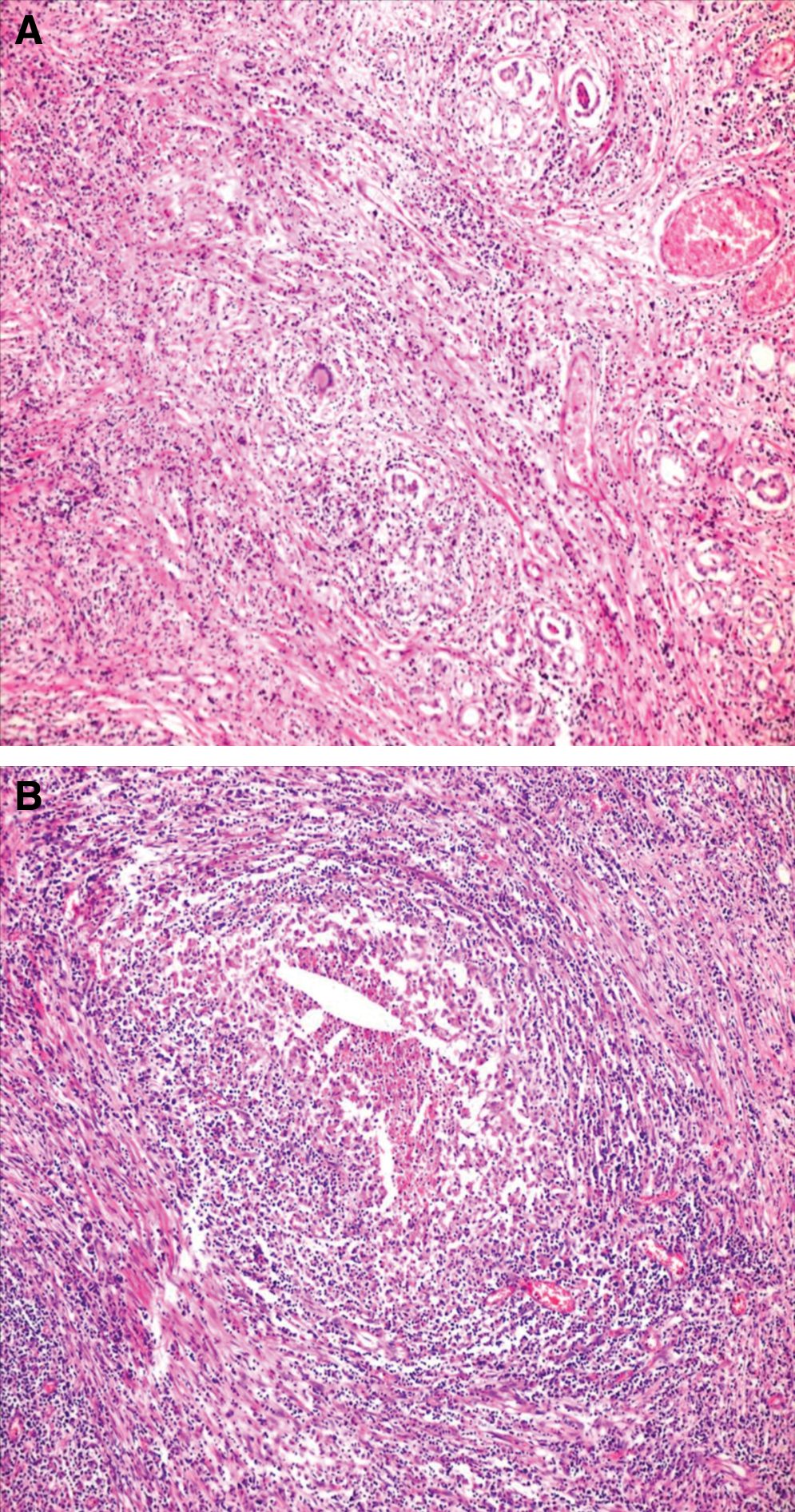
Fibrosis and lymphocytic inflammation within individual thyroid follicles. Langhans-type giant cells are seen in the middle (hematoxylin–eosin; × 40 magnification) (
Although there is an impression that thyroid TB is common in Turkey (2), this diagnosis was assigned to only one of 2780 thyroidectomy specimens in our hospital. This prevalence is even less than the 0.6% noted by Ozekinci et al. (1). As extrathyroidal TB is not present in primary thyroid TB, it is possible that in some patients with this condition the diagnosis is missed because it is less likely to be suspected, even if they have had thyroid surgery. We postulate that in primary thyroid TB the thyroid is infected by the hematogenous route but clinically evident seeding does not occur in other organs (1). Based on the clinical information available, most of the five patients reported by Ozekinci et al. (1) probably had primary thyroid TB because, except for one patient with relapsing fever, they did not have systemic symptoms or signs. In a large series of 76 patients with thyroid TB reviewed by Bulbuloglu et al. (3), 65 were primary and 11 were secondary (3), consistent with the predominance of primary thyroid TB in the study of Ozekinci et al. (1). In the report by Ozekinci et al. (1), all had a thyroid mass as their presenting symptom but, in contrast to the patient reported here whose mass was quite large, their thyroid masses were quite small, ranging from 1 to 2 cm.
In summary, thyroid TB is a rare cause of thyroidal masses. Fine-needle aspiration cytology is useful but, as noted in our patient, not completely reliable. The possibility of thyroid TB must be considered when patients present with thyroid masses in areas where TB is endemic, even those who do not have features of systemic TB. We recommend surgical removal and anti-TB medications if residual TB in the thyroid is likely or extrathyroidal TB is present.
Footnotes
Acknowledgment
This work was performed at the Diyarbakir Education and Research Hospital, Diyarbakir, Turkey.
Author Contributions
S.A., I.G., and B.C. contributed to writing the article and literature review as well as comprehensive literature search; S.A. and B.C. contributed to design and manuscript preparation; A.T.A. and A.S. provided histopathological information.
Disclosure Statement
The authors declare that they have no competing interests.