
Abstract
Background:
The best biochemical marker of Graves' disease (GD) is the presence in serum of autoantibodies to the thyroid-stimulating hormone receptor (hTSHR-Ab). The aim of this study was to evaluate the performances of two sensitive hTSHR-Ab assays with a specific focus on the clinical importance of differences in results. Both assays are competitive in nature but employ quite different types of ligands. In the “M22-pTSHR” assay, hTSHR-Ab competes with a labeled monoclonal antibody (M22*) against the thyrotropin (TSH)-receptor for binding to porcine TSH receptors. In the “bTSH-rhTSHR” assay, hTSHR-Ab competes with labeled bovine TSH for binding to recombinant human TSH receptors.
Methods:
bTSH-rhTSHR and M22-pTSHR were measured in patients from a population study: 106 had new hyperthyroidism due to GD, 93 had multinodular toxic goiter, 100 had new primary autoimmune hypothyroidism, and 100 were healthy controls.
Results:
Receiver operating characteristic curves indicated a high sensitivity and specificity of both assays (area under curve, bTSH-rhTSHR: 0.977 [confidence interval: 0.954–1.00]; M22-pTSHR: 0.979 [confidence interval: 0.957–1.00]). The two assays identified nearly the same patients who were hTSHR-Ab positive, though large differences in hTSHR-Ab values were obtained in a number of individual patients (ratio bTSH-rhTSHR/M22-pTSHR, range: 0.33–6.5 in patients positive with both assays). Values were in average 2.5 times higher with the bTSH-rhTSHR assay compared with the M22-pTSHR assay, corresponding to the difference in recommended clinical cut-off values (1.0 IU/L and 0.4 u/L). The bTSH-rhTSHR assay had a considerably lower intraassay coefficients of variation of 3.8%; for M22-pTSHR, it was 9.5% (p < 0.01).
Conclusions:
Both assays had a high sensitivity and specificity for diagnosing GD. hTSHR-Ab values were in average 2.5 times higher with the bTSH-rhTSHR assay compared with the M22-pTSHR assay. In individual patients, the ratio between results obtained using the two assays varied widely. Thus, results obtained using one assay cannot be quantitatively transformed to values obtained using the other assay. bTSH-rhTSHR had a considerably lower intraassay coefficients of variation and it may be better suited for longitudinal studies of hTSHR-Ab.
Introduction
hTSHR-Ab can be measured by bioassays and by competitive TSH binding assays. The competitive binding assays are the only validated routine assays for measuring hTSHR-Ab but they do not differentiate between stimulating and blocking hTSHR-Ab. The sensitivity and specificity of the competitive binding assays have improved remarkably during the last 10–15 years (9,10).
Several studies have been performed in recent years to compare the performance of various types of hTSHR-Ab assays. It was concluded that an assay based on competition between labeled monoclonal antibody M22 (M22*) (raised against human TSH receptor) and hTSHR-Ab for binding to porcine TSH receptors had a higher diagnostic accuracy than an assay in which labeled bovine TSH competed with hTSHR-Ab for binding to porcine TSH receptors (11). Further, an automated M22-pTSHR assay performed similar to or better with regard to the diagnosis of GD compared with four other commercial hTSHR-Ab assays (12). In another study, an automated M22-pTSHR assay had a high diagnostic specificity and sensitivity and performed very similar to a number of manual assays based on hTSHR-Ab and labeled bovine TSH competition with recombinant or purified porcine TSH receptors (13). Most studies comparing different hTSHR-Ab assays have included sera from patients referred to hospitals or thyroid clinics.
The aim of the present study was to compare the performance of two assays for hTSHR-Ab that are routinely used in Denmark in patients with newly diagnosed GD, multinodular toxic goiter (MNTG), and primary autoimmune hypothyroidism (PAH) and in controls. The principles of the assays are shown in Figure 1. Notably, these assays differ in both label and TSHR employed. We studied whether the same diagnosis was obtained by both the assays and whether the results obtained by both the assays could be used interchangeably in patients. The participants were included consecutively from epidemiological studies, thus avoiding referral bias and ensuring participation of patients with a more variable degree of disease than patients selected from clinics.
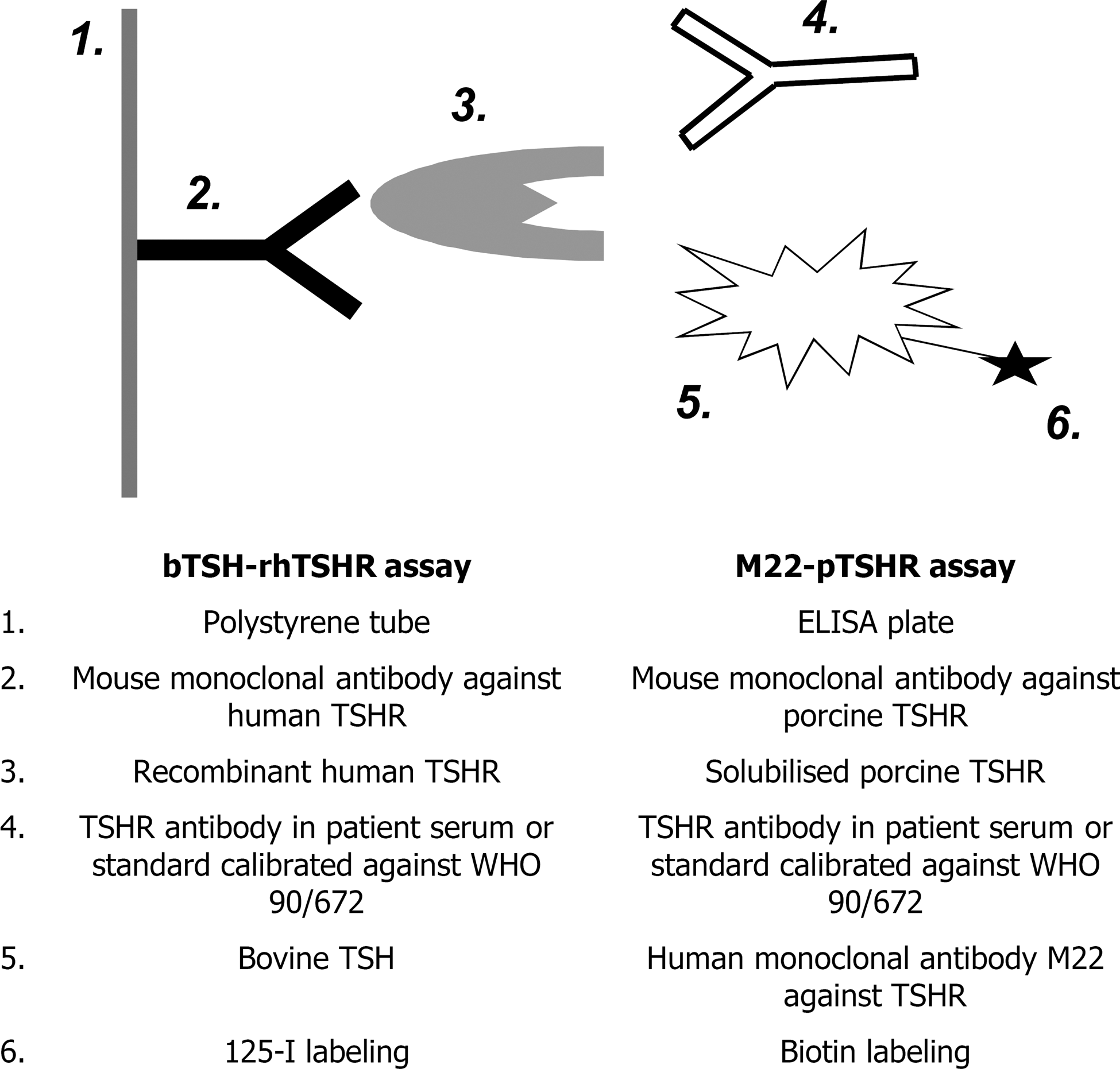
Principles of the two TSH receptor autoantibody assays evaluated in the study. In both assays, the overall principle is competition between compound 4 and compound 5 on binding to immobilized TSH receptors (compound 3). TSH, thyrotropin; TSHR, TSH receptor; WHO, World Health Organization.
Materials and Methods
Participants were included from two epidemiological surveys performed as part of the monitoring of the iodine supplementation program in Denmark: A register study was conducted in which all new cases of hyper- and hypothyroidism in a well-defined population plus a cross-sectional comparative population study including 4649 randomly selected subjects from two regions in Denmark were registered and examined. The participants in both studies have been described in detail earlier (14,15).
Consecutive patients from the population with hyperthyroidism due to GD (n = 106) and MNTG (n = 93) as well as patients with spontaneous primary hypothyroidism judged to be caused by autoimmunity (PAH) (n = 100) were included from the register study. Hyperthyroidism was diagnosed from a suppressed serum TSH combined with an elevated serum triiodothyronine (T3) and/or serum thyroxine (T4). Hypothyroidism was diagnosed from a high serum TSH combined with a low serum T4. Controls were included from the cross-sectional study.
Patients with hyperthyroidism were categorized into nosological diagnoses based on clinical features and thyroid imaging, as described in detail earlier (16). In brief, patients with GD had clear signs of Graves' orbitopathy and/or a completely homogeneous thyroid gland by scintigraphy and/or ultrasonography. Patients with MNTG had multinodular glands with a mixture of hot and cold areas by scintigraphy. All scintigraphies were categorized by agreement between four doctors, two consultants in endocrinology and two senior registrar doctors trained in evaluation of thyroid scintigraphies. Thyroid volume was calculated by ultrasonography as length × width × depth × π/6 for each lobe (14).
Many of the patients had received medication by their general practitioner for a short period before blood samples for hTSHR-Ab measurements were drawn (treated/untreated: GD, 84/21; MNTG, 46/48; and PAH, 72/28). In general, blood samples were taken within 1–2 months after the first blood test that indicated thyroid disease. For every third GD, MNTG, and PAH patient, an age- and sex-matched control person (n = 100) from the same population was chosen randomly.
Blood samples were stored at −20°C. The bTSH-rhTSHR assay was performed about 1 year after the blood samples had been drawn, whereas the M22-pTSHR assay was performed about 8 years after blood sampling. To evaluate whether storing time had influenced the test result, bTSH-rhTSHR was reanalyzed in 32 randomly selected samples with bTSH-rhTSHR values in different ranges. The results showed good agreement and correlated with a coefficient at 0.947 (p < 0.01).
bTSH-rhTSHR was analyzed in duplicate in 71 samples. All 400 samples were measured in duplicate with the M22-pTSHR assay. Duplicate measurements were performed in independent assays. The results from the second measurement were only used to calculate coefficients of variation (CV). Both assays were manual (nonautomated) and performed by skilled technicians who had performed the assays on a routine basis for more than 1 year. The technicians were blinded with respect to the nature of the individual samples and pairing of duplicates.
Assays
The bTSH-rhTSHR assay was DYNO® TRAK human by BRAHMS Diagnostica (Berlin, Germany). The principle of the assay is competition between hTSHR-Ab in a serum sample (from patients or standard preparations) and radio-iodinated bovine TSH for binding to human recombinant TSH receptors immobilized on coated tubes (Fig. 1). Assay cut-off given by the manufacturer, positive ≥1.0 IU/L, was confirmed by us, as previously reported (16). The M22-pTSHR assay was TSH Receptor Autoantibody 3rd Generation ELISA kit from RSR Ltd. (Cardiff, UK). In this assay, hTSHR-Ab in patient serum or standard preparations compete with a biotin labeled human monoclonal antibody M22 (M22*) against the TSH receptor for binding to immobile porcine TSH receptors. The assay cut-off given by the manufacturer was ≥0.4 u/L. According to the manufacturers, both assays had been standardised/calibrated to the international standard for TSHR autoantibodies derived from patients' sera (90/672 from the National Institute for Biological Standardisation and Control, Potters Bar, UK) (WHO 46th Report, No. 872).
Statistical analyses
Data processing, including receiver operating characteristic curves, nonparametric correlation coefficients, and logistic regression models, was performed with SPSS 13.0 software (SPSS, Chicago, IL). The association between the ratio of bTSH-rhTSHR/M22-pTSHR (2.5 or below vs. above 2.5) (outcome variable) and the independent variables: age, sex, and smoking habits (daily smoking, occasional smoking, nonsmoking); level of hTSHR-Ab (bTSH-rhTSHR: 1–2.9; 3.0–9.9 or ≥10 IU/L); thyroid volume (females: 0–18 mL, >18 mL; males: 0–25 mL, >25 mL); and subtype of thyroid disease (GD, MNTG, and PAH) was analyzed in logistic regression models for dichotomous variables. The CV's were compared by Bartlett's test for homogeneity of variance. The level of significance was set at 5%.
The study was approved by the regional Ethics Committee in Northern Jutland and Copenhagen.
Results
To evaluate the threshold for positive hTSHR-Ab values given by the manufacturers, a receiver operating characteristic plot analysis was made for both assays based on patients with GD and controls (Fig. 2) (17). The bTSH-rhTSHR assay gave an area under curve of 0.977 (95% confidence interval: 0.954–1.00), and the M22-pTSHR assay gave an area under curve of 0.979 (confidence interval: 0.957–1.00), thus indicating a high sensitivity and specificity of both assays when the recommended cut-offs were applied.
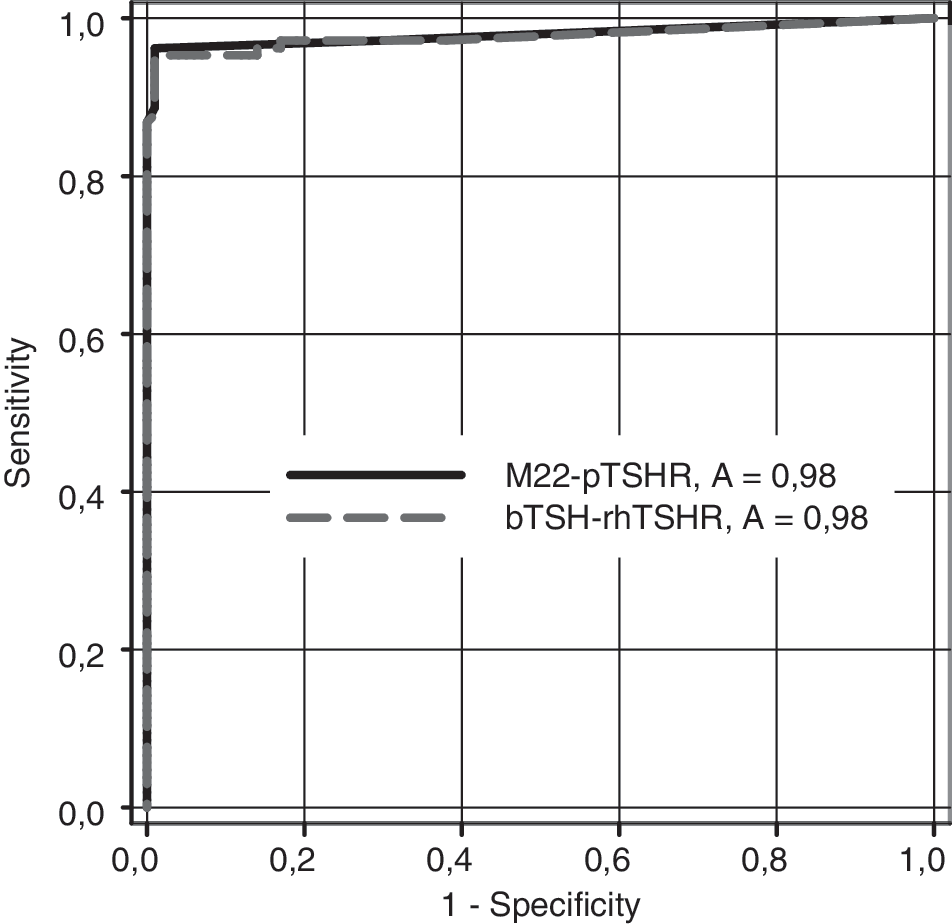
Results of the receiver operating characteristic analyses indicating an identical high sensitivity and specificity of the bTSH-rhTSHR assay and the M22-pTSHR assay when the cut-off values recommended by the manufacturer were used. Only patients with Graves' disease (GD) and controls are included.
The diagnostic sensitivities of the two assays were calculated from the 106 patients with GD and the specificities from controls. Using manufacturers' cut-off, the following were the findings: bTSH-rhTSHR, sensitivity: 95.3%, specificity: 99.0%; M22-pTSHR, sensitivity: 94.3%, specificity: 99.0%. Thus, the overall diagnostic performance of the two assays differed only minimally, as shown in Table 1. Among the patients, one patient with GD had a low but positive bTSH-rhTSHR concentration (1.1 IU/L) and was just below the cut-off with the M22-pTSHR assay (0.3 u/L). Being negative with the bTSH-rhTSHR assay, the five patients with GD were also negative with the M22-pTSHR assay. Two patients with PAH were slightly positive with the bTSH-rhTSHR assay (1.2 IU/L in both) but were below the cut-off with the M22-pTSHR assay (0.3 u/L in both). On the other hand, one patient with PAH was positive with the M22-pTSHR assay (0.7 u/L) but negative with the bTSH-rhTSHR assay (0.5 IU/L). In the remaining 97 patients with PAH, there was concordance between the positive/negative results given by the two assays. In the case of MNTG that was primarily diagnosed in 93 patients, there was concordance between the positive/negative results given by the two assays. One control subject being euthyroid but with a strong family history of thyroid disease was hTSHR-Ab positive with both assays (Table 1).
Number (percent). Cutoff values, bTSH-rhTSHR: ≥1.0 IU/L; M22-pTSHR: ≥0.4 μ/L.
The bTSH-rhTSHR assay gave, in general, higher values (IU/L) than the values (u/L) obtained by the M22-pTSHR assay. The mean of the ratio between the bTSH-rhTSHR and the M22-pTSHR values in participants with positive hTSHR-Ab by both assays was 2.53 (GD: 2.50; MNTG: 2.83; PAH: 2.22). This is similar to the ratio between the cut-off values used in the present study and those given by the manufactures at 1.0 IU/L and 0.4 u/L, respectively. The geometric mean of the ratio between the bTSH-rhTSHR and the M22-pTSHR values in participants with positive hTSHR-Ab was calculated to be 2.26.
In individual patients with positive hTSHR-Ab, the ratio between bTSH-rhTSHR and M22-pTSHR varied between 0.33 and 6.50. The correlation between the bTSH-rhTSHR and the M22-pTSHR values in participants with positive hTSHR-Ab at different levels of hTSHR-Ab is illustrated in Bland-Altman plots (Fig. 3). For comparison, the M22-pTSHR u/L values have been multiplied by 2.5 to achieve the IU/L values. In the low, middle, and high range of hTSHR-Ab, considerable variation was observed with no systematic difference. In sera with higher hTSHR-Ab values, however, there was a tendency of more negative than positive points, indicating that the values had been measured relatively higher with the M22-pTSHR assay than with the bTSH-rhTSHR assay.

Bland–Altman plots of bTSH-rhTSHR versus M22-pTSHR in different ranges of bTSH-rhTSHR concentration. Only patients with both positive bTSH-rhTSHR and M22-pTSHR are included. The M22-pTSHR values were multiplied with 2.5. In the range of high values of bTSH-rhTSHR, there was a tendency that the M22-pTSHR values were systematically relatively higher than the bTSH-rhTSHR values. Three outliers were excluded (bTSH-rhTSHR/M22-pTSHR [not multiplied with 2.5]: 59.8/102.0; 44.9/137.0; 70.1/158.0).
The CV's of samples measured in duplicate and correlations between the measurements are shown in Table 2. The bTSH-rhTSHR assay had a low interassay CV% of 3.8%. This was higher for the M22-pTSHR assay (CV%: 9.5%) (p < 0.001). When the hTSHR-Ab values obtained by the two different assays were compared, they correlated significantly (p < 0.01) (Table 2), but the interassay variation was high (CV%: 32.9%).
M22-pTSHR values were multiplied with 2.5.
Number of cases with hTSHR-Ab values above the cut-off.
Coefficients of variation were calculated from results obtained by two independent measurements using the bTSH-rhTSHR assay; two independent measurements using the M22-pTSHR assay; a single measurement using the bTSH-rhTSHR assay; and a single measurement using the M22-pTSHR assay.
Correlation coefficient (Spearman's rho). All correlations were significant, p < 0.01.
To evaluate whether the relatively high difference between bTSH-rhTSHR and M22-pTSHR values seen in some patients was associated with different patient characteristics as age, sex, smoking, thyroid volume, subtype of thyroid disease, and level of hTSHR-Ab, data in hTSHR-Ab positive participants were analyzed in logistic regression models with the ratio of bTSH-rhTSHR/M22-pTSHR as outcome. The only significant association was between a low ratio of bTSH-rhTSHR/M22-pTSHR (below 2.5) and a high concentration of hTSHR-Ab. This confirmed the pattern seen in the Bland–Altman plots (Fig. 3).
Discussion
We compared the performance of two commercially available sensitive assays for in vitro measurements of TSH-receptor autoantibodies in serum. Both assays are used for routine measurements of hTSHR-Ab in Denmark, and one important question to evaluate was whether hTSHR-Ab values obtained with the two assays are comparable. A major difference in reagents between the two assays is the use of labeled bovine TSH for competition with hTSHR-Ab in one of the assays (bTSH-rhTSHR assay), in contrast to the labeled monoclonal antibody against the TSH receptor that is used in the other assay (M22-pTSHR). Both the assays showed a high sensitivity and specificity for diagnosing GD, and patients in whom MNTG had been primarily diagnosed were subsequently found to be hTSHR-Ab positive with the bTSH-rhTSHR assay and also positive with the other assay. The same was observed in patients with PAH and in healthy controls. Around 5% of patients with GD were hTSHR-Ab negative with both assays. They had a mild degree of hyperthyroidism, and the percentage of patients who tested negative for hTSHR-Ab is in concordance with other studies on patients newly diagnosed with GD (18).
Despite the indication by both manufacturers of calibration against the international standard preparation National Institute for Biological Standardisation and Control 90/672, hTSHR-Ab values obtained using the two assays were in average 2.5 times higher with the bTSH-rhTSHR assay compared with the M22-pTSHR assay. When corrected for this difference, the cut-off values (clinically positive vs. negative) recommended and used in the present study for the two assays were identical. However, in individual patients the ratio between results obtained by the two assays varied widely (range bTSH-rhTSHR/M22-pTSHR: 0.33–6.50). Thus, results obtained using one assay cannot be quantitatively transformed to values that would have been obtained using the other assay.
The so-called “second generation” hTSHR-Ab assays are often based on recombinant human TSH as ligand and have a higher sensitivity and specificity compared with the “first generation” assays (19,20). It has been speculated whether this improvement is due to the recombinant human TSH receptors or is the result of differences in technical performance between the two generations of assays (16,21,22). Zöphel et al. compared two “second generation” hTSHR-Ab assays based on porcine and humane TSH receptors, respectively (20,23). Both assays had a high sensitivity, thus the authors concluded that there was no clinical relevant difference between the two assays and that it was the assay system with immobilization of the TSH receptors rather than the origin of the TSH receptors that was important.
More recently, a hTSHR-Ab assay based on human monoclonal autoantibodies to the TSH-receptor (M22) was described and called “third generation” hTSHR-Ab assay (24). The authors found a higher sensitivity of this new assay compared with a “second generation” assay based on inhibition of biotin labeled TSH binding to TSH receptor coated wells. This finding has been confirmed in later studies of patients with new GD (11,12), including a large international multicenter trial (13) in which the sensitivity of a new, rapid, and fully automated electrochemiluminescence immunoassay based on M22 was 97% in patients with newly diagnosed GD compared with a sensitivity of the sum of the other assays at 94%. On the other hand, when Liu et al. (25) compared a corresponding “third generation” hTSHR-Ab assay also based on M22 with the conventional bTSH-rhTSHR assay in 84 patients with GD, the diagnostic sensitivities were 92.9% and 95.2%, respectively. In the study by Liu, the between-run CV of the M22-pTSHR assay was unacceptably high at 28.2%. When a higher cut-off was chosen for the M22-pTSHR assay corresponding to a CV at 20%, the sensitivity decreased to 85.7%. The majority of the 84 patients were on prolonged antithyroid drug therapy.
In the present study, we found a significantly higher CV of the M22-pTSHR assay compared with the values obtained by the bTSH-rhTSHR assay. On the other hand, it has been reported that an automated M22-pTSHR assay has a lower CV% than the values obtained by the M22-pTSHR ELISA used in the present study (13).
The practical consequences for clinical use of the two assays compared in the present study are several. We previously evaluated the possible clinical use of hTSHR-Ab measurements, as outlined in Table 3 (26). From the present study, the two assays would apparently be equally suited for evaluation of patients with newly diagnosed hyperthyroidism (Table 3). Due to the lower CV% of the bTSH-rhTSHR assay, however, it seems to be preferable in the longitudinal follow-up of patients. Even if there are no specific studies on the performance of different hTSHR-Ab assays in patients with Graves' orbitopathy, it would be expected that the assay would be equally suited for diagnosing this condition in patients with euthyroid. Concerning evaluation of the risk for fetal and neonatal hyperthyroidism, it should be taken into account that the two assays give results that are systematically quite different. Thus, if a hTSHR-Ab limit of risk of 5 IU/L is used for the bTSH-rhTSHR assay, this limit should probably be lower with the M22-pTSHR assay, because this assay gives in average values that are 2.5 times lower.
Validity of measurements of bTSH-rhTSHR and M22-pTSHR in clinical thyroidology.
hTSHR-Ab measurements have a relatively low predictive value for relapse of hyperthyroidism in GD in many (7,8) but not in all studies (6). More studies are needed as indicated by:?
Studies are needed as indicated by:?
There is no indication of a difference in quality of assays for these purposes, but usefulness is an assumption as no systematic studies have been performed using the assays.
Even if results obtained by the two assays correlated significantly and they identified nearly the same patients as being hTSHR-Ab positive, large differences in results were obtained in individual patients. Thus, if hTSHR-Ab measurements are used on a longitudinal basis to follow a gradual remission of GD during therapy, as in patients with orbitopathy, hTSHR-Ab values should be obtained using the same assay. For such serial use, the bTSH-rhTSHR assay might be optimal due to the low CV (CV%: 3.8) of this assay compared with the values obtained by the M22-pTSHR assay (CV%: 9.5), as mentioned earlier.
In conclusion, both assays had a high sensitivity and specificity for diagnosing GD. hTSHR-Ab values were in average 2.5 times higher with the bTSH-rhTSHR assay compared with the M22-pTSHR assay. In individual patients, the ratio between results obtained using the two assays varied widely. Thus, results obtained using one assay cannot be quantitatively transformed to values obtained using the other assay. The bTSH-rhTSHR assay had a considerably lower intraassay CV than the M22-pTSHR assay and may be better suited for longitudinal studies of hTSHR-Ab.
Footnotes
Acknowledgments
We are grateful to Jens Johnsen and Kirsten Hald for expert technical assistance and to BRAHMS Diagnostica for assistance with reagents for the present study.
Disclosure Statement
The authors declare that no competing financial interests exist.