
Abstract
Background:
Diagnostic imaging provides useful anatomical and morphological information of cervico-mediastinal goiters. The aim of this study was to assess the usefulness of multidetector computed tomography (MDCT) with multiplanar reformatting and volume rendering reconstructions for the preoperative evaluation of retrosternal goiters in patients for whom magnetic resonance imaging is contraindicated.
Methods:
From March 2006 to January 2009, 34 patients (20 women and 14 men; mean age, 48 years; range, 42–74 years) with suspected cervico-mediastinal goiter were assessed by MDCT after intravenous injection of contrast material. The following parameters were evaluated: morphology, size, and enhancement of thyroid lobes; presence, location, and mediastinal extension of thyroid tissue; and relations with mediastinal vessels and organs. All patients underwent thyroidectomy. A reference group of 34 patients evaluated by single-detector computed tomography was created. The two groups of patients were compared searching for operative time (OT, in hours), hospital stay (HS, in days), and morbidity rate observed after thyroid surgery in all cases.
Results:
In 29/34 patients, thyroid was enlarged with left mediastinal extension in 12 cases, right extension in 10 cases, and posterior extension in 7 cases. In 3/34 patients, a normal cervical thyroid connected to the mediastinal goiter through a thin parenchymal stripe was observed. In 2/34 patients, thyroid lobes were enlarged, without mediastinal extension. By comparing the two groups of patients for OT and HS values, a significant reduction to 3.7 ± 0.1 hours and 4.3 ± 0.1 days, respectively, was found in the group of MDCT patients, and also a trend to the reduction for morbidity rate (21%) could be recognized.
Conclusions:
MDCT represents a noninvasive tool in the evaluation of retrosternal goiters. High-quality multiplanar reformatting and volume rendering reconstructions allow an optimal analysis of the plunged gland and could reduce OT, HS, and probably the morbidity rate.
Introduction
This condition, reported as cervico-mediastinal or intrathoracic goiter, is different from ectopic goiter, which originates from ectopic thyroid tissue located into the mediastinum. Ectopic thyroid tissue does not have cervical component and shows thoracic vascularization (3).
The incidence of cervico-mediastinal goiters ranges from 1.7% to 30%, with prevalence in women and in older age group of patients (4 –6). Cervico-mediastinal goiters originating from the isthmus or inferior lobes of the gland usually extend into anterior mediastinum before recurrent laryngeal nerve and vascular structures. These goiters have an easier surgical approach. On the contrary, cervico-mediastinal goiters originating from posterior and lateral parts of the thyroid and developing into the posterior mediastinum, behind the recurrent laryngeal nerve and vascular and nervous structures, have a more difficult surgical excision (1,6,7). Clinically, 20–35% of retrosternal goiters are asymptomatic (8); 70% become symptomatic and the most common symptoms are related to compression of trachea with dyspnea, stridor, and cough; the compression of esophagus, recurrent laryngeal nerve, and superior vena cava can cause dysphagia, dysphonia, Horner's syndrome, superior vena cava syndrome, and cerebral edema (9 –12). Total thyroidectomy represents the treatment of choice for retrosternal goiters (6,10,13 –16).
Diagnostic imaging provides a preoperative evaluation of cervico-mediastinal goiters, defining the correct thyroid location, size, and mediastinal extent and showing vascular and adjacent organ involvement. Conventional chest X-ray allows the evaluation of mediastinal enlargement, calcifications, and tracheal and esophageal compression or deviation (12).
Ultrasonography (US) allows an accurate study of the thyroid gland, but it is not useful for the entire assessment of the mediastinal component.
Scintigraphy provides functional and morphological information, but it is unable to evaluate the plunged gland in the presence of an iodine-131 hypocaptation (17,18).
Recent studies have emphasized the role of single-detector computed tomography (SDCT) in the preoperative study of endothoracic goiters. For a correct therapeutic planning, some authors advocate the use of SDCT even if this modality cannot provide an appropriate multiplanar imaging (19 –25).
Because of its multiplanar capabilities, magnetic resonance imaging (MRI) allows the acquirement of important elements for the anatomo-topographic evaluation of thyroid thoracic extension and adjacent nervous–vascular involvement (22,25 –27). However, this imaging technique cannot be used in patients with contraindications (19). The principal contraindications of the MRI procedure are mostly related to the presence of metallic implants in a patient, and the risk of MRI scans increases with the used field strength. Therefore, all electronically, magnetically, and mechanically activated implants, ferromagnetic active devices, haemostatic clips, and cardiac pacemakers represent absolute contraindications, and image quality could also be severely degraded because of the presence of artifacts. In addition, although the increasing availability of open MRI systems, claustrophobic and anxious patients often refuse this examination (19,28). Multidetector computed tomography (MDCT), with new improved reconstruction software, could allow to accurately study the cervico-mediastinal structures.
The aim of this study was to evaluate the diagnostic possibilities of MDCT in the preoperative assessment of mediastinal goiters.
Materials and Methods
Between March 2006 and January 2009, 34 patients (20 women, 14 men; mean age, 48 years; range, 42–74 years) with suspected cervico-mediastinal goiter underwent MDCT. All patients included in the study had MR contraindications. Twenty-nine patients had a suspected endothoracic goiter at both US and chest X-rays. In the remaining five patients, the indication to CT was given by chest X-rays in three patients and by US in two cases. For all patients, thyroid scintigraphy and clinical examination were unable to give information for a definitive diagnosis. Written informed consent was obtained from all patients in accordance with the declaration of Helsinki principles. A total thyroidectomy was performed in all patients by the same operative staff.
CT scans were obtained using a 16-row MDCT scanner (TSX-101A-Aquilion; Toshiba Medical System, Tochigi, Japan), with the following acquisition parameters: slice thickness 1 mm, increment 0.8 mm, pitch 1.75, rotation time 0.5 seconds, and 120/250 kV (peak)/(mA·s). Unenhanced scans were not performed. Contrast-enhanced multidetector row CT scans were obtained after intravenous injection of iodinated contrast material (Ultravist 370; Schering, Berlin, Germany) in a cubital vein, using a 16–18-G needle and an automatic injector (MK-IV; Medrad, Pittsburgh, PA), at a dose of 1.5 mL/kg body weight and injection rate of 3 mL/s. Scans were performed from the hyoid bone to the diaphragm with a 25-second delay after contrast material injection. The mean acquisition duration was 15 seconds. All MDCT data were transferred to a workstation (HP XW 6400) equipped with dedicated software (Vitrea 4.0; Vital Images, Minneapolis, MN) for image reconstructions. The postprocessing programs used were multiplanar reformatting (MPR) and volume rendering (VR). Transverse and reconstructed images were evaluated by two expert radiologists (A.A.S.I. and G.A.) not directly involved in the scanning and blinded to the results of chest X-rays, US, and thyroid scintigraphy. The entire image analysis was performed within 10 minutes for each patient. Differences in assessment were resolved with consensus.
In MDCT image evaluation, the following parameters were considered: morphology and size of thyroid lobes (axial and longitudinal diameters); presence, location (anterior or posterior), and mediastinal extent of thyroid tissue below sternoclavicular articulation; relations with aortic arch branches; tracheal deviation and stenosis (diameter, <1.5 cm); esophageal compression; enhancement of thyroid gland after intravenous injection of contrast material (homogeneous or inhomogeneous).
To evaluate the possible advantages of postprocessing techniques, a reference group was created. It was represented by 34 patients (with clinical and histological findings similar to the first group of patients) affected by cervico-mediastinal thyroid goiter, retrospectively searched in our computerized archive, who underwent CT scan examination in the period between March 2003 and April 2005 using a SDCT scanner (Picker PQ 5000; Marconi Medical System, Cleveland, OH) and surgically treated in all cases by the same operative staff. The two groups of patients were compared searching for the operative time (OT, in hours), the hospital stay (HS, in days), and the morbidity rate (complications) observed after thyroid surgery in all cases.
Statistical analysis
t-Test was used to compare the two groups of patients for the OT and the HS mean values. Chi-square test was applied to evaluate the two groups for the morbidity rate observed after thyroid surgery. In both statistical tests, all variables were considered statistically significant for p-values of ≤0.05. Interobserver agreement between the two radiologists was evaluated using weighted k statistics. A k-value of more than 0.81 was considered to represent almost perfect agreement and values of 0.61–0.80 and 0.41–0.60 to represent substantial and moderate agreement, respectively. NCSS 2007 software was used for statistical analysis.
Results
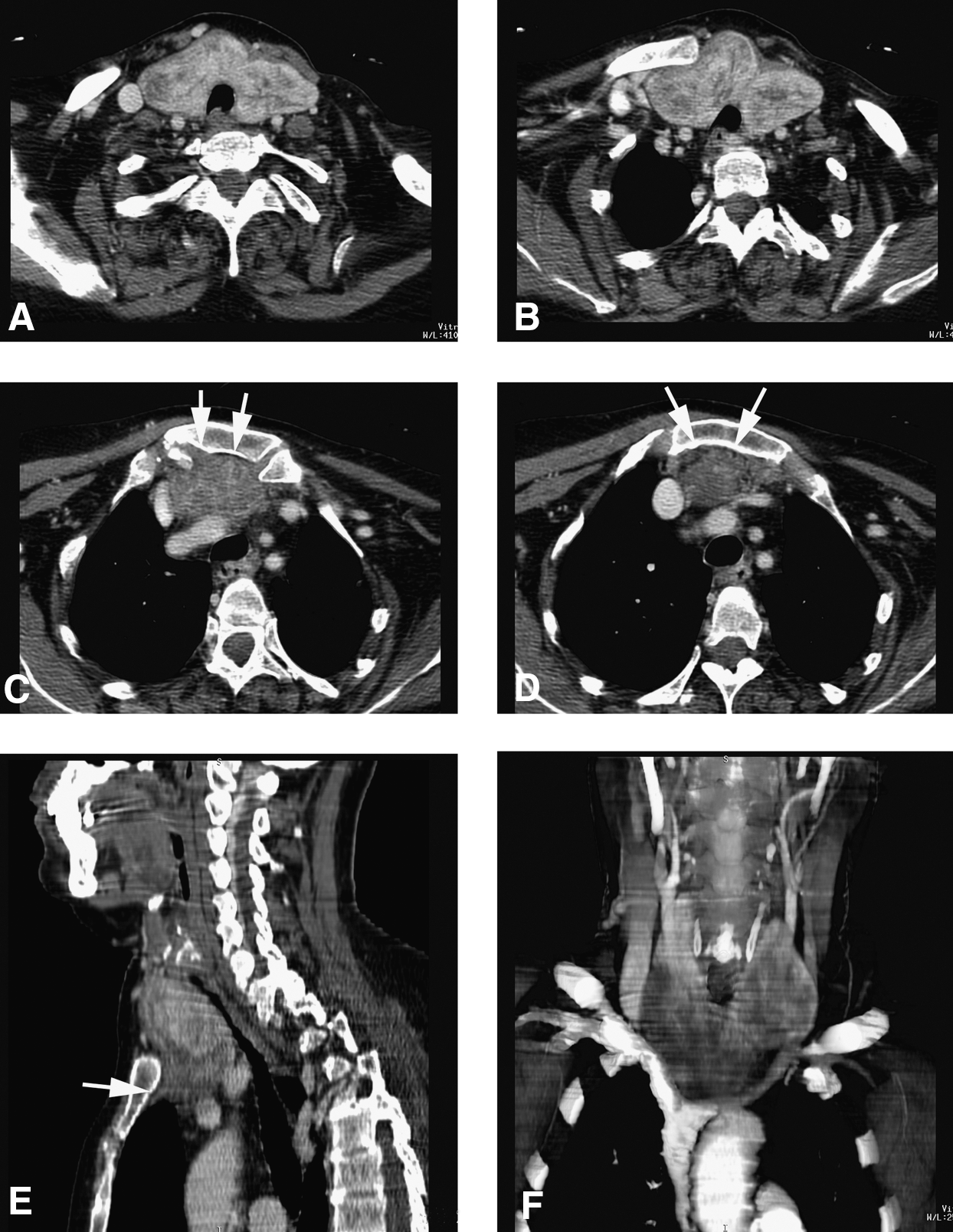
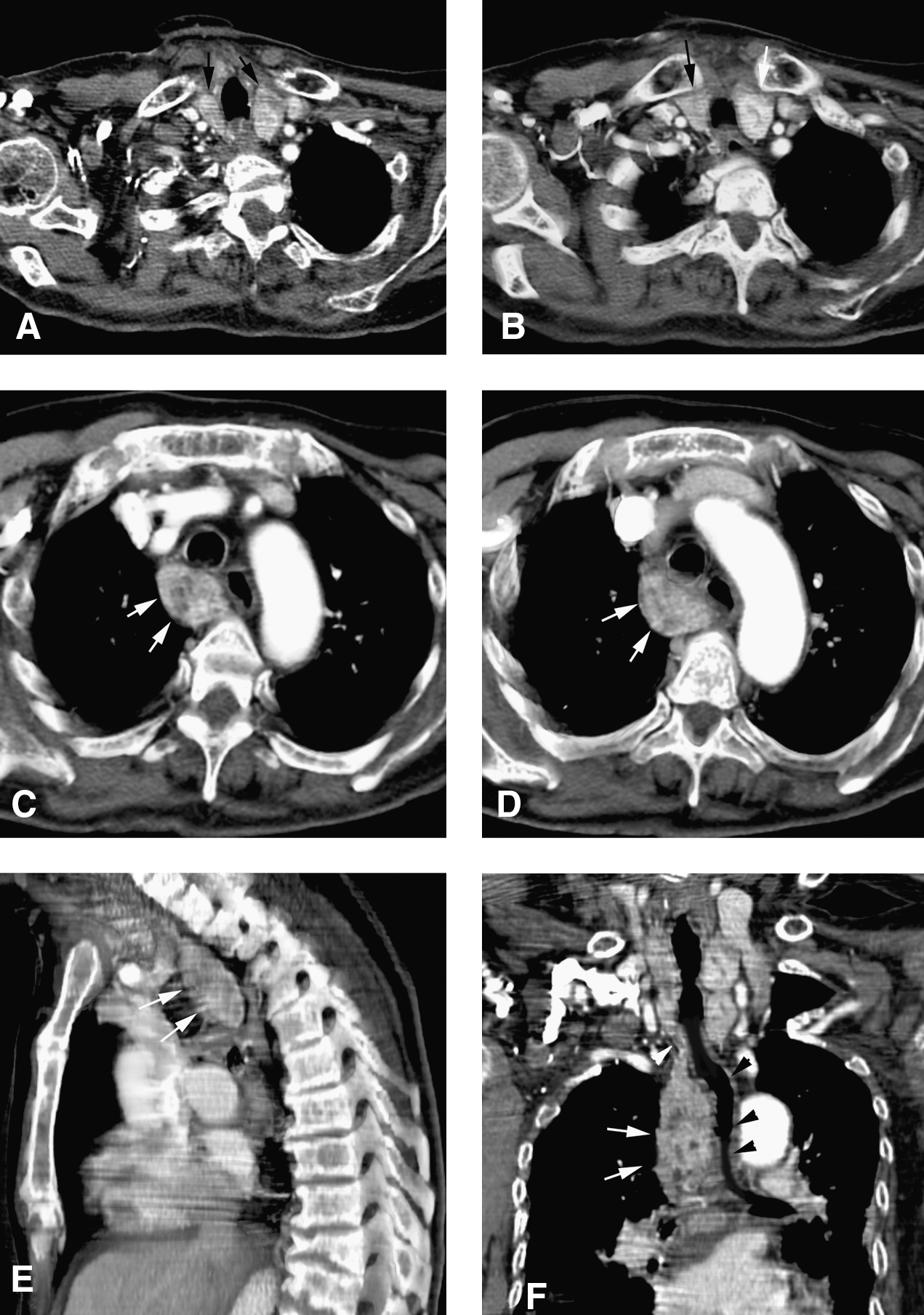
Depending on CT findings detected in the group of 34 patients who underwent MDCT examination, 29/34 (85%) had enlarged thyroid lobes. In 12/29, thyroid had a left mediastinal extension. In five cases, thyroid tissue extended into the anterior mediastinum involving the common carotid artery, whereas in seven patients the gland had a posterior mediastinal extension (Fig. 1), involving the common carotid artery and subclavian artery that were displaced anteriorly. The trachea was shifted to the right side with a normal lumen in eight patients; in the other four patients, tracheal lumen stenosis was detected. Esophageal compression and right postero-lateral displacement were found in six cases. In 10/29 cases, the thyroid had a mediastinal extension along the right side. In four cases, thyroid tissue was located in the anterior mediastinum (Fig. 2), involving the right common carotid artery; in six cases, it was located in the posterior mediastinum reaching the carotid artery and the brachiocephalic trunk. The trachea was shifted to the left side with a normal lumen in seven patients; in three cases, MDCT showed lumen stenosis. Esophageal compression and left postero-lateral displacement were found in five cases. In 7/29 patients, the thyroid lobes extended into the posterior mediastinum without vascular displacement or esophageal and tracheal deviation or compression.

Left retrosternal goiter. Axial scans (
Right retrosternal goiter. Axial scans (
In 3/34 (9%) cases, MDCT revealed a mediastinal goiter in patients with a normal cervical thyroid. In these patients the mediastinal thyroid tissue was connected to the gland through a thin parenchymal stripe. In 2/3 patients, a right posterior mediastinal extension was observed (Fig. 3), with a left tracheal deviation and moderate esophageal compression, whereas in one patient the thyroid extended into the left posterior mediastinal inlet with a right tracheal deviation and normal esophagus lumen.
Right thyroid goiter with normal size and location of the thyroid lobes. Axial scans (
In 2/34 (6%) patients, enlarged thyroid axial and longitudinal diameters without a clear mediastinal involvement were found. In these patients, tracheal lumen was regular with left deviation in one case. No sign of esophageal compression was identified.
In all cases, the thyroid cervical component showed an inhomogeneous enhancement due to calcifications and necrotic areas. In 32 patients with mediastinal extension, the same pattern was found.
In all cases, MPR and VR reconstructions allowed an optimal evaluation of vascular structures and contiguous organs and were useful in defining vascular relations when the thyroid mass caused a considerable displacement of adjacent structures and an infiltrating lesion was suspected. After total thyroidectomy, histopathological examinations revealed a nodular hyperplasia in 30 cases and nodular lesions with atypical cells in the other 4 cases. The mean OT value for these patients was 3.7 ± 0.1 hours standard error (SE) and the mean HS value was 4.3 ± 0.1 days SE. The morbidity rate (seroma/hematoma, transient hypoparathyroidism, and transient unilateral recurrent nerve palsy) was 21% (7/34 patients). As reported in Figures 4 and 5, comparing these patients to the SDCT reference group for the OT and the HS values, a statistically significant difference was found (OT = 4.7 ± 0.1 hours SE; HS = 5.9 ± 0.2 days SE, for the reference group), with p-values of <0.001 for both variables. A morbidity rate of 38% (13/34 patients) was found in the reference group. By comparing these values, no statistically significant difference was found (p = 0.13). Almost perfect agreement between the two readers was found (k = 0.87).
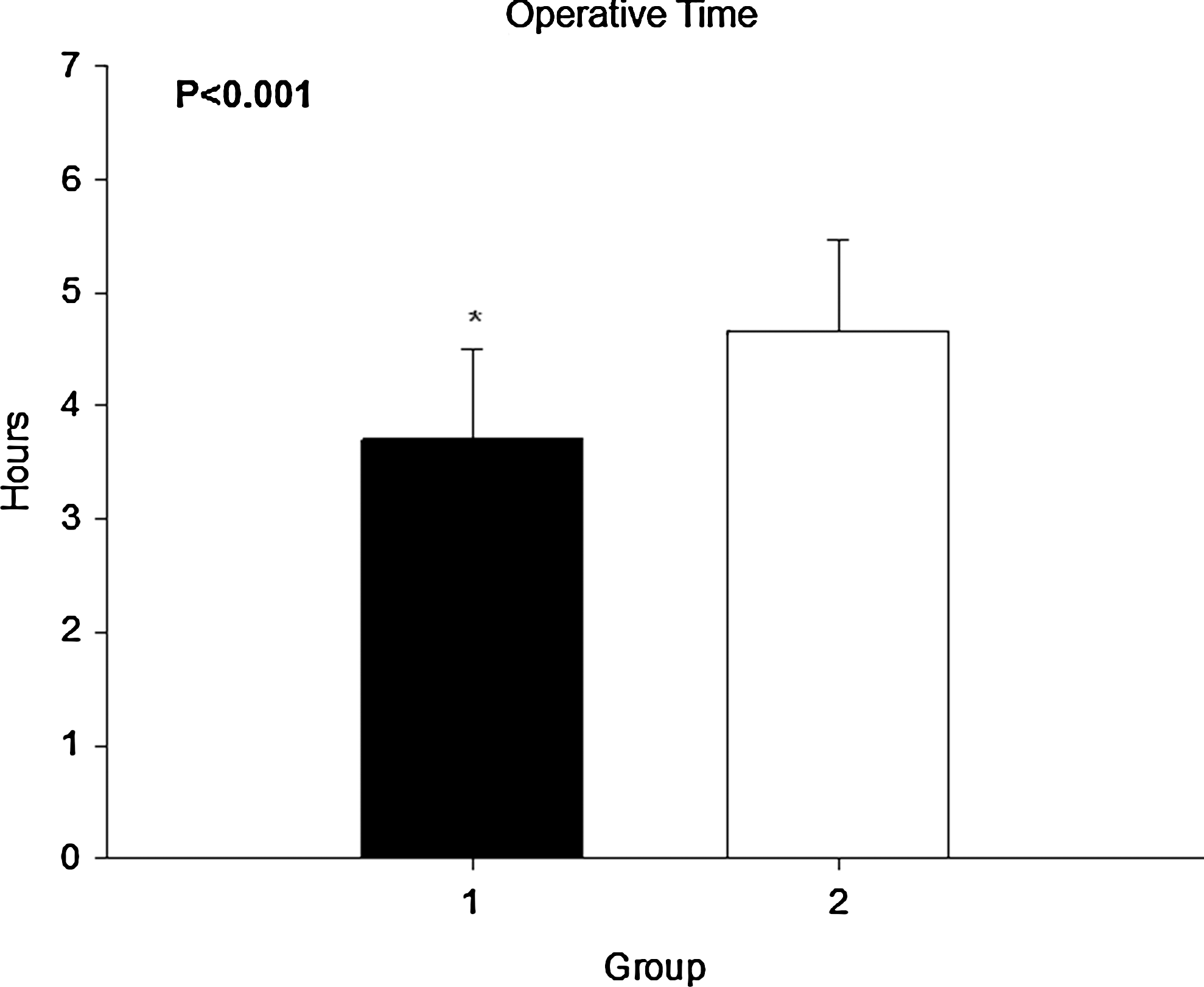
Operative time (in hours) for the two groups of patients (1, multidetector computed tomography; 2, single-detector computed tomography; *, p < 0.001).
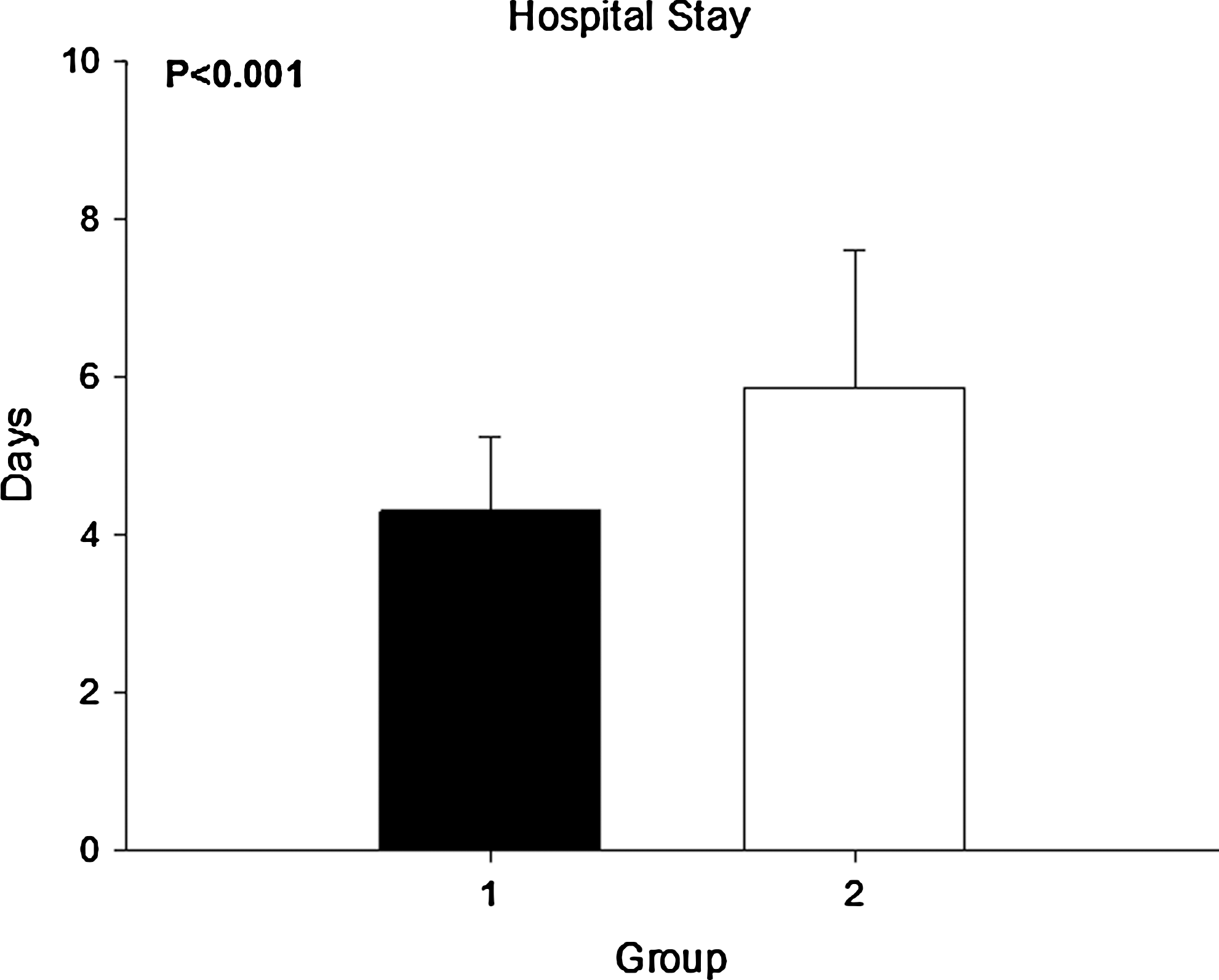
Hospital stay (in days) for the two groups of patients (1, multidetector computed tomography; 2, single-detector computed tomography).
Discussion
Mediastinal extension of large multinodular goiters is a relatively common condition that is caused by the anatomic continuity of cervical with thoracic cavity (6). When a retrosternal goiter is clinically suspected, the aim of any imaging tool is to provide the maximum information for therapeutic planning. Neck and chest X-rays as well as barium studies give indirect evidence of intrathoracic extension of the gland. Mediastinal enlargement, tracheal deviation, and esophageal compression represent the main radiological findings (1,4,12).
US plays an essential role in the study of thyroid disease; it is noninvasive and relatively cheap and it does not require any particular preparation for patients, also permitting cytologic examination with fine-needle aspiration sampling. In cervico-mediastinal goiters, US cannot correctly evaluate retrotracheal and retrosternal components of the disease (29).
Nuclear scintigraphy is a complementary technique for retrosternal goiter and ectopic thyroid; it provides useful anatomical, functional, and metabolic information using technetium 99m and iodine-131 captation. However, it is more expensive than US, requires radioisotopes, and sometimes (10–30%) is unable to recognize pathologic thyroid tissue and areas with no tracer uptake (17,18).
Because of its multiplanar imaging property and high-contrast resolution, MRI has been considered the most accurate and the less-invasive diagnostic procedure in the preoperative evaluation of retrosternal goiters; MRIs allow images on axial, sagittal, and coronal planes to be obtained, permitting the evaluation of cervical and mediastinal thyroid components and their relations with vessels and adjacent organs. According to some authors, MRI is more accurate than CT in the anatomical evaluation of thyroid tissue with a 100% accuracy (22,26 –28,30). However, MRI cannot be used in patients with contraindications such as pacemakers, vascular clips, and suffering from claustrophobia.
Some reports described the contrasting role of SDCT in the preoperative evaluation of retrosternal goiters, which is also related to the different scanners used (20 –22,30). SDCT allows an accurate evaluation (86%) of the thyroid tissue, defining location, size, and relations with mediastinal structures (27). The introduction of new MDCT scanners, with the possibility of studying wide volumes by thin slice thicknesses and the improved quality of postprocessing reconstructions due to isotropic voxels, provides a more accurate evaluation of retrosternal goiters. As far as we know, few studies (31,32) focused on the use of MDCT in the evaluation of plunged thyroid. In our experience, MDCT allowed an optimal morphovolumetric study of the gland in all patients; moreover, this technique permitted the identification of plunged thyroid tissue and its relationship with vascular structures and adjacent organs in 94% of cases, excluding an intrathoracic component in the remaining 6%. Cervical gland and plunged thyroid presented the same inhomogeneous enhancement due to calcifications and fluid areas. This finding, associated with the continuity of cervical gland with plunged thyroid, can differentiate retrosternal goiters from other diseases with a mediastinal location (24). However, the enhancement is not useful to distinguish areas of nodular hyperplasia from atypical cellular areas in the plunged thyroid tissue.
To reduce the radiation dose, no unenhanced CT scan was used, and all data were obtained using a single phase after contrast material injection.
In our experience, isotropic reconstructions obtained by MDCT raw data for the evaluation of thyroid disease provide a synthetic and anatomic visualization to the surgeon, particularly on coronal planes that simulate the habitual surgical approach to the gland.
VR and MPR images also allow a panoramic evaluation of vessels in their whole course, especially when a vascular displacement is present. Because of postprocessing, anterior or posterior plunged tissue location and mediastinal structure compression or dislocation were accurately defined. In fact, in 72% of cases, thyroid tissue was localized in posterior mediastinum and the vessels in strict relationship with recurrent laryngeal nerve were displaced anteriorly. The evaluation of these relations is useful to avoid some iatrogenic consequences such as dysphonia and paralysis of vocal cords (16). The possibility to localize plunged tissue in posterior mediastinum and to evaluate the displacement of vessels can provide an indirect location of the recurrent laryngeal nerve, reducing surgical risk.
Our results suggest that the use of isotropic images obtained by MDCT scanners can reduce the OT and the HS of patients undergoing total thyroidectomy for mediastinal goiters by providing useful preoperative information to the surgeon, especially when other clinical and instrumental tools cannot allow a complete evaluation of the disease. In fact, the treatment of retrosternal goiters is clearly surgical and most often medical therapy is ineffective (32); MDCT imaging could modify the operative management of these patients by suggesting a cervical or intrathoracic surgical approach based on the mediastinal extent up to the aortic arch or right atrium (33). Although the analysis of morbidity rate was nonstatistically different between SDCT and MDCT in our experience, an important trend to the reduction of complications could be recognized using MDCT images. Further studies are needed in this field to verify these data and to reduce the risk of any therapeutic approach in patients affected by retrosternal goiters. In conclusion, MDCT represents a noninvasive tool performed in selected cases that are characterized by a difficult approach with other imaging techniques. High-quality MPR and VR reconstructions could allow an optimal evaluation of the plunged gland, giving useful information to the surgeon and reducing the OT, the HS, and probably the morbidity rate.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.