
Abstract
Background:
Although thyroid nodules are frequently detected in patients during routine examinations, such nodules are rarely malignant. Surgical treatment of nodules is controversial because of the possible complications associated with surgery, and there is an unmet need for a minimally invasive alternative. We previously reported on a high-intensity focused ultrasound (HIFU) device that induced necrosis in ewe thyroids. This complementary study on 27 ewes evaluated the use of the device to produce thyroid lesions, characterized the HIFU-induced lesions on the thyroid and surrounding structures, and evaluated the safety and reproducibility of the method.
Methods:
A spherical 3-MHz transducer that was coupled to a 5-MHz linear array ultrasound imaging probe was used to generate powerful acoustic waves to destroy thyroid tissue. Three series of experiments were conducted: thyroid lesion experiments (10 ewes), safety experiments (4 ewes), and reproducibility experiments (13 ewes). After fixation of the ewe's neck, tissue lesions were examined both macroscopically and histologically.
Results:
First, individual pulsed acoustical waves were used to induce lesions in 19 thyroid lobes. In most lesions, there was coagulative necrosis that was replaced later by fibrosis. Macroscopic examination of adjacent organs revealed skin lesions and muscle injuries. A second series of experiments evaluated the consequences of HIFU pulsed waves on structures surrounding the thyroid to better characterize possible side effects of HIFU. Firings at the periphery of eight lobes revealed macroscopic lesions in the trachea of one ewe and superficial esophagus lesions in three ewes. The recurrent nerves were damaged bilaterally in one ewe that died from dysphagia 3 days after HIFU. Four ewes were found to have muscle injuries, but no skin lesions were observed. A third series of experiments evaluated the reproducibility of a HIFU prototype designed specifically for human use. Thyroid lesions were obtained in 25 of the 26 treated lobes. No damage to the nerves, trachea, esophagus, or muscles was observed. About 3 of the 13 ewes had superficial skin burns.
Conclusion:
The results obtained in the ewe model show that thyroid lesions with a defined volume can be induced safely and suggest that the HIFU device is now ready for evaluation in humans.
Introduction
Thyroid nodules are frequently detected during routine physical or ultrasonography examinations (6 –8). Very few of these nodules are malignant, and surgical treatment remains controversial because of complications associated with surgery, such as unsightly scarring, bleeding, and damage to recurrent nerves or to parathyroid glands (9 –12). Consequently, a minimally invasive method for precise targeted destruction of thyroid tissue would be of great interest to physicians in this field. Percutaneous ethanol injections have been proposed to treat nodules noninvasively (13), but this method is often painful and can require repeated injections. In addition, the results are uncertain. A more promising method is percutaneous laser ablation (PLA), which was evaluated in a series of 62 patients presenting with large (>5 mL) cold nodules (14). Significant nodule reduction was possible with PLA versus the drug levothyroxine or no treatment; however, only 7/21 PLA patients showed significant (>50%) thyroid reduction at 12 months. PLA is still somewhat invasive, requiring the insertion of two 21-gauge spinal needles; it is often painful, although the results are promising compared to treatment with levothyroxine.
Our previous findings (15) indicated that a modified version of the HIFU device used to induce prostate tissue necrosis could also produce well-delineated HIFU-induced necrosis in ewe thyroids. However, that device was designed for treating human prostate cancer, and the surrounding organs were unfortunately damaged by the ultrasound beam. Clearly, modifications were required to achieve safe and precise thyroid targeting and ablation.
In this study, we first developed a HIFU device that could be used to noninvasively destroy thyroid tissue in ewes. Second, we characterized the HIFU-induced lesions in the thyroid and surrounding tissues. Finally, we evaluated the safety and reproducibility of this method in the ewe model.
Materials and Methods
Animals
The ewe model turned out to be the best choice because of its cervical anatomy. The ewe's thyroid gland is easily accessible with ultrasound. It is located in the middle of the animal's neck and is relatively superficial. The dimensions of the gland and the distances from surrounding structures are about two-thirds of those in humans. As sheep do not develop thyroid nodules, the treatment involved healthy thyroid tissue.
Twenty-seven ewes (2–10 years of age; 65–87 kg) were purchased from Coredif (Le Mée-sur-Seine, France) or from the French National Institute for Agronomy Research. The ewes were transported, fed, and housed in accordance with the national guidelines for animal studies.
Procedures for anesthesia and analgesia
Anesthesia was induced by sodium thiopental injection (10 mg/kg) into the jugular vein and was maintained by halothane inhalation (1.5%). Ventilation was controlled mechanically (50% O2; 50% air; 12 L/min; 20 cycles/min) via a tracheal tube sealed with a saline-inflated balloon. An electrocardiogram oscilloscope (Hewlett-Packard 78304A, Palo Alto, CA) was used for cardiac monitoring. A 10-mm esogastric tube was inserted for gastric fluid aspiration. A 5% glucose solution containing penicillin G (1 MU) was perfused (500 mL/h). The animals were injected intramuscularly with the analgesic flumixidine (2 mL/day) for the first 3 days after HIFU delivery.
HIFU device
A modified version of the Ablatherm® device (EDAP, Vaulx-en-Velin, France) was modified further to optimize ewe thyroid targeting and ablation. A spherical 3-MHz transducer (diameter 50 × 36 mm; focal point 40 mm) was coupled to a 5-MHz linear array ultrasound imaging probe so that the center of the spherical transducer, where acoustic waves concentrate, lay precisely in the imaging plane.
The acoustic energy generated by the HIFU transducer at the focal point is calculated as follows: Acoustic power in watts/total focal surface in cm2 (16).
The focal surface is calculated using the ellipse formula (transversal width a = 0.77 and longitudinal length b =1.11 mm: π × a × b/4 = 0.68 mm2.
For example, in the last series of experiments, we used a reference power of 15.6 electric watts, with a transducer output of 75% and we obtained 11.7 acoustic watts.
The acoustic energy generated by our HIFU device is 11.7 W/68 mm2 = 1725 W/cm2.
Ablation of thyroid tissue
An anesthetized ewe was placed in a supine position on an operating table (Fig. 1). Its neck was carefully shaved using an electric razor and all remaining hair was removed using depilatory cream. Ultrasound guidance was used to accurately position the device over the right or left lobe of the thyroid. Various parameters relating to lesion induction were defined: beam intensity, pulse duration, intervals between firings, and the position and size of the target. The settings were based on values obtained in our previous feasibility study and depended on the thicknesses of cutaneous, subcutaneous, and muscle tissues as well as on the depth of the thyroid lobe and the desired volume of necrosis to be produced. A computer controlled the ultrasound beam, the movements of the device head containing the transducer, and the ultrasonography probe.
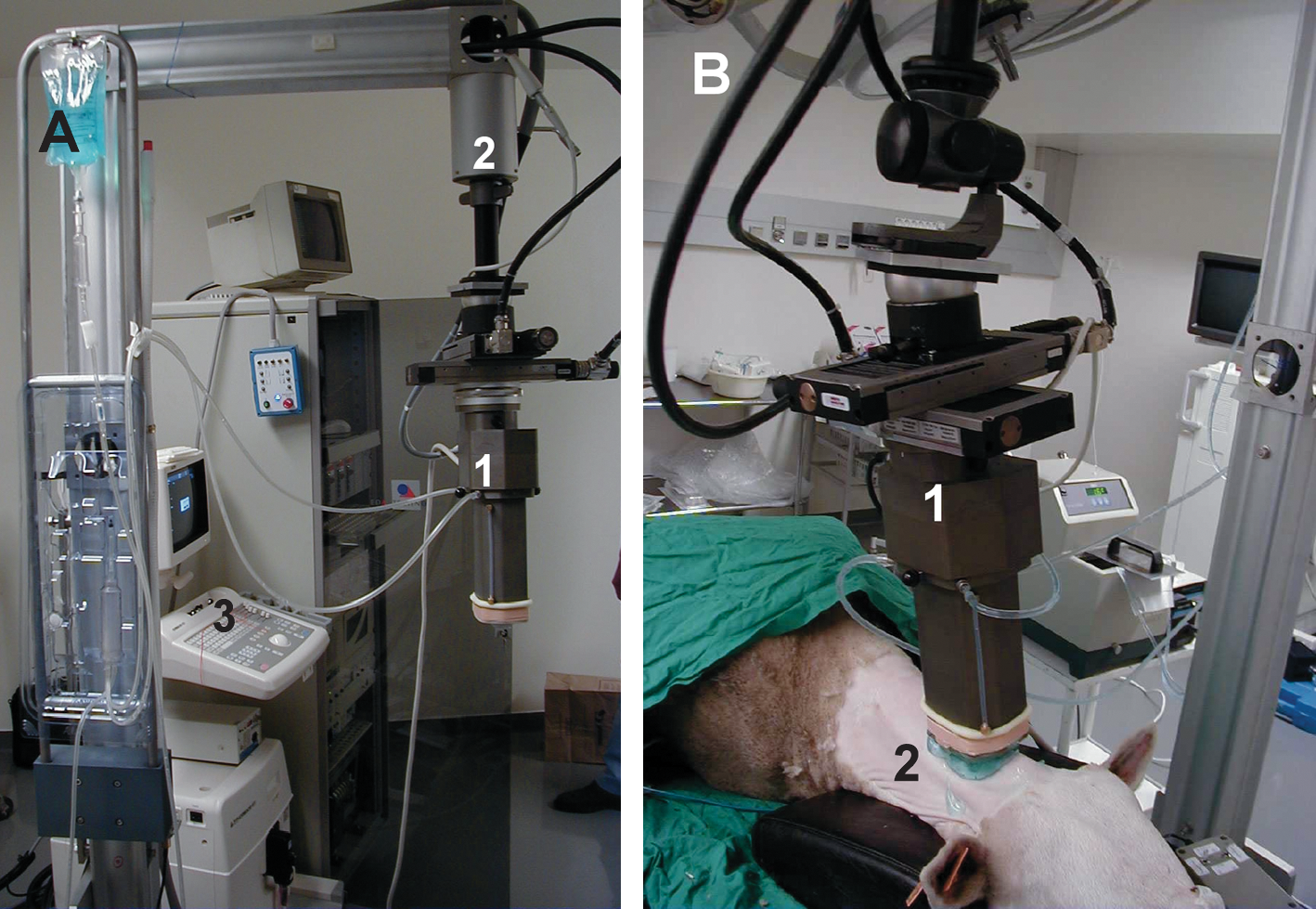
Prototype of the HIFU instrument developed for human thyroid ablation. (
Evaluation of tissue following HIFU treatment
Immediately following HIFU treatment, the animal's skin was examined for external damage. Over the next few days, the ewe was closely monitored to detect possible side effects such as fever, wheezing, dyspnea, roaring, or eating difficulties. At a defined time, a lethal dose of sodium pentobarbital (40 mL) was injected intravenously into each ewe. The animal was bled via a femoral catheter, after which the anterior part of the neck was removed and fixed in a large volume of formalin. The specimens were large enough to include both superficial and deep structures. All the anatomical structures were examined macroscopically, including thyroid lobes, trachea, esophagus, muscles, and recurrent nerves. The thyroid gland was then removed and processed for microscopic analysis.
Each thyroid specimen was oriented, weighed, and measured. After 12 hours of formalin fixation, serially numbered longitudinal sections, 3- to 5-mm thick, were prepared from the whole lobes and the sections encompassing the HIFU-treated area were measured. The thyroid tissue sections were paraffin embedded. The microscopic analysis on 3-μm tissue sections stained with hematoxylin–eosin was performed by a single pathologist (B.F.).
According to the time duration between the HIFU treatment and the ewe sacrifice, several different morphological features were encountered. The following features were considered as HIFU related: early necrosis, (Fig. 2B, C), coagulative necrotic areas (either confluent or separated), multiple pure fibrotic scars separated by normal thyroid tissue (identified as “peripheral fibrosis”), or single or multiple necrotic areas circumscribed by a fibroinflammatory rim with or without reactive epithelial hyperplasia. In latter lesions “mummified colloid areas” appeared (Fig. 2A) with or without central fibrosis, and inflammatory or not. In addition, foreign body–like giant cell reaction engulfs or surrounds the fragmented colloid and is accompanied with reactive epithelial hyperplasia. When lesions occurred outside the HIFU-targeted areas, they were identified as “peripheral necrosis” that were a result of peripheral dispersion of the HIFU beam and dissemination of its targeted heat.
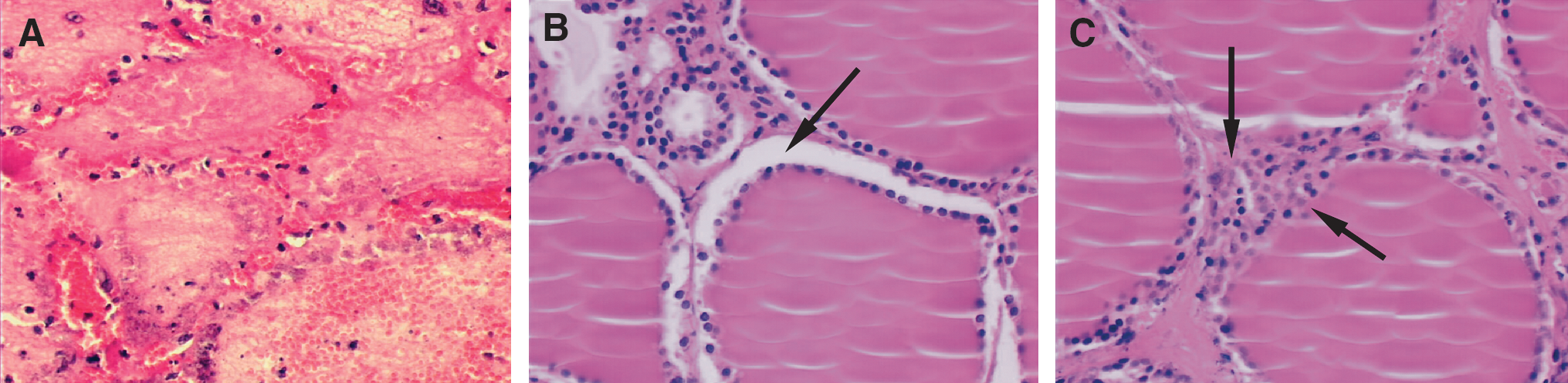
Representative microscopic HIFU-induced thyroid lesions. (
We finally performed a score to evaluate the HIFU performance on the treated thyroid. Three parameters were taken into account: the location of the lesion ranked: 1 if the target was reached or 0 if it was not reached; the type of the lesion ranked: 2 if there was confluent destruction and/or scars, 1 if we observed several destroyed areas separated by apparently normal thyroid tissue; 0 if necrosis made further observation difficult; the intensity of the lesion ranked: 1 intense, 0 faint.
The performance was considered as optimal (i.e., efficient destruction of targeted tissue). if the sum of the three tested parameters was 3, intermediate if it was 2, poor if it was 0 to 1one.
Results
Development of the HIFU device
The HIFU device used initially was progressively modified as results were obtained. The head was modified for more precise positioning, and a 5-MHz linear array imaging probe was used for transverse and longitudinal imaging. Both transducers were enclosed in a thin envelope, and refrigerated circulating liquid allowed acoustic contact of the transducers with the skin while the transducers were cooled. The treatment visualization unit was motorized on two axes, allowing for computer-controlled focusing on the target.
Generation of thyroid lesions using HIFU (series 1)
The first series of experiments were designed to assess the lesions induced by HIFU in thyroid tissue. Toward this end, 19 thyroid lobes in 10 ewes were targeted with HIFU pulses. The pulses lasted 4.5 seconds, with a 10-second interval between pulses. The other HIFU parameters are listed in Table 1. The ewes were sacrificed 1 (n = 2), 2 (n = 3), or 4 (n = 5) weeks after the HIFU treatment.
Three series of experiments were conducted: series 1, thyroid lesion experiments; series 2, safety experiments; and series 3, determination of reproducibility.
Results are given as the mean ± SD [min.–max.].
HIFU, high-intensity focused ultrasound; SD, standard deviation.
HIFU-induced lesions were observed in all 19 thyroid lobes examined; macroscopic examination (Fig. 3) revealed no tracheal or laryngeal lesions. However, 1 superficial esophageal lesion, 9 skin lesions, and 18 muscle injuries were observed on the 19 examined lobes and surrounding structures. Histological examination and scoring of the 19 lesions (as described in the Materials and Methods section) indicated that the lesions fell into three groups based on the characteristics of the thyroid lesions: optimal (11 lobes), intermediate (3 lobes), and poor (5 lobes).
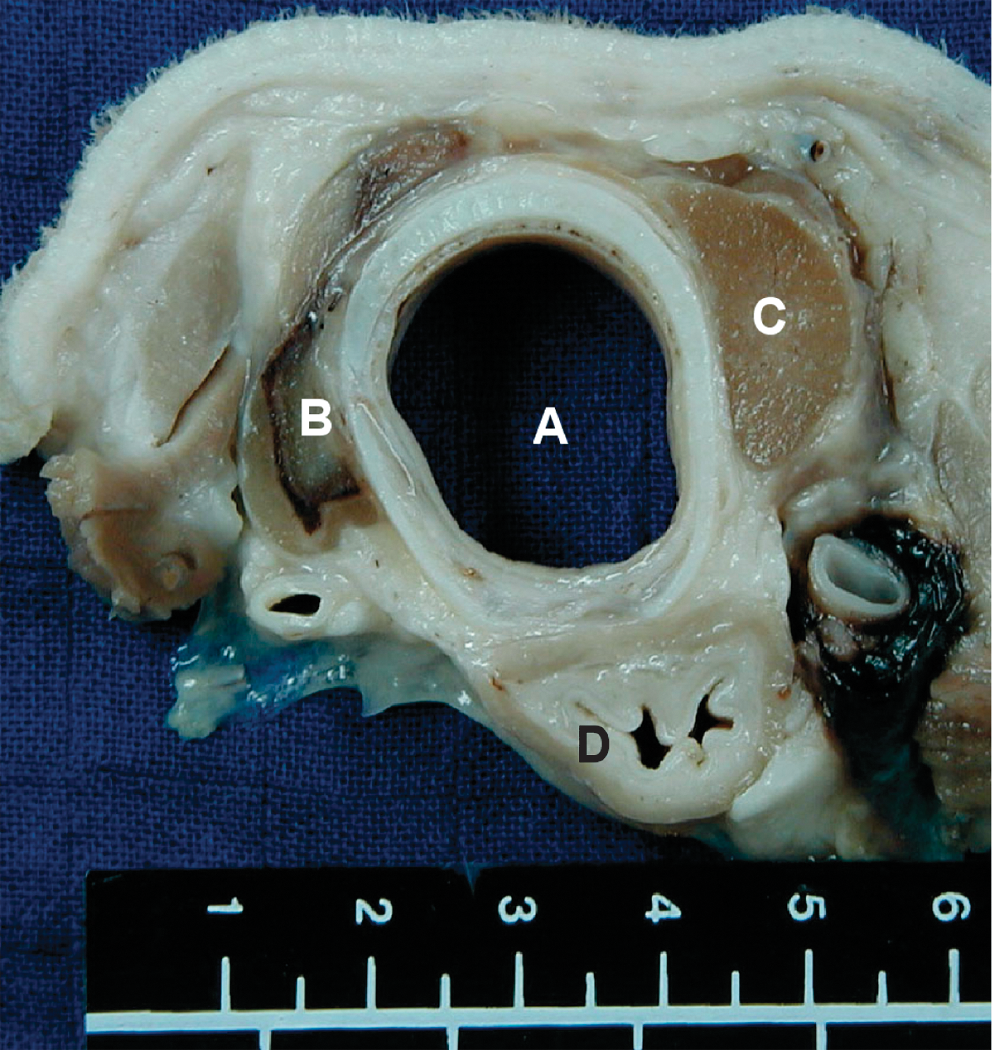
Macroscopic view of the anterior part of the ewe's neck 1 week after HIFU was used to induce a lesion on the thyroid. There is a central area of necrosis (9 × 4 mm) in the right lobe (
Effect of HIFU on peripheral structures (series 2)
In a second series of experiments in four animals (eight lobes), we targeted the structures surrounding the thyroid and analyzed the clinical and pathological consequences of repeated HIFU pulses. The entire lobe, including the periphery and the recurrent nerves, was exposed to the HIFU. The treatment parameters are shown in Table 1. To reduce at the same time the occurrence of skin burns, two ewes were injected subcutaneously with saline or plasma substitute before HIFU delivery in an attempt to increase the distance of the skin from the target so that the acoustic beam was more widely spread over the skin. Reducing the acoustic pulse power or the pulse duration resulted in a 0.7 energy reduction in two other ewes.
In this second series of experiments (Table 1), two ewes died of dysphagia 2 and 3 days after HIFU. The other ewes were sacrificed at 2 weeks (n = 1) or 3 weeks (n = 1). No skin lesions were observed, and there were fewer muscle lesions compared to the first series. This can probably be attributed to the use of subcutaneous injections and the lower energy that was used for the pulses. Macroscopic examination revealed a tracheal lesion in one ewe and superficial esophageal lesions in three ewes. The recurrent nerves were damaged bilaterally in the ewe that died 3 days after HIFU, which accounted for the fatal dysphagia.
Reproducibility of a modified HIFU prototype device (series 3)
Having optimized treatment conditions in the first two series of experiments, we adapted the acoustic energy to levels that should induce lesions but avoid side effects (Table 1). The reproducibility of the method was evaluated in 13 animals (26 lobes) sacrificed at 2 weeks (n = 5) or 4 weeks (n = 8). In this series, the mean lobe size dimensions were as follows: length = 41.1 mm, height = 10.2 mm, and width =8.8 mm with a mean standard deviation of 3.6, 2.6, and 3.7 mm respectively.
By this time, electronic changes had been made to adapt the HIFU prototype for use in humans, and the prototype met the technical standards required for use in humans (Fig. 1). Subcutaneous fluid injections were not performed in this study.
After HIFU treatment (Table 2), lesions consisting of fibrotic replacement of necrosis were present in 25/26 lobes. In one ewe, no lesion was observed in the thyroid or surrounding tissues. In 23 lobes, the fibrotic lesions were small and plurifocal, with each spot of fibrosis corresponding to one pulse hit. These plurifocal lesions were surrounded by normal tissue. The lesions were large and unifocal in the two remaining lobes (Fig. 4). No damage was seen in the nerves, trachea, esophagus, or muscles (Table 1), and only three superficial skin burns were observed. These results show that using the correct parameters, the method can be tested safely on humans, although the spacing between the pulses should be reduced to avoid damaging surrounding tissue and to obtain unifocal lesions.
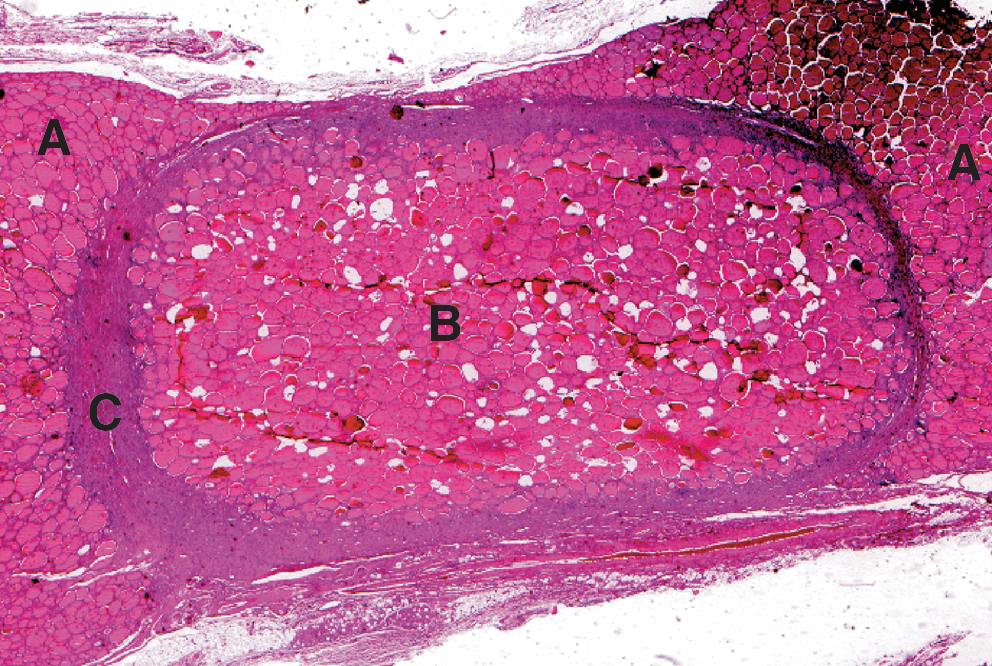
A typical HIFU-induced microscopic lesion in thyroid tissue 1 week after the treatment. Note the coagulative necrosis (
In series 3, the desired lesions were produced in thyroid tissue without any damage to surrounding structures. All the lesions were correctly centered in the thyroid lobe at macroscopy. The number of HIFU pulses and lesion sizes are summarized in Table 3.
NA, not available; R, right lobe; L, left lobe.
Discussion
This study evaluated a HIFU device designed specifically for ablation of ewe thyroids with the aim of adapting the device for use in humans. To optimize safety, we evaluated the limits of this technique by varying the firing parameters (e.g., beam intensity, intervals between pulses, and pulse duration). We were able to obtain local destruction of the thyroid without hits to neighboring tissues. Accurate targeting and a better understanding of the HIFU technique resulted in better tissue destruction compared to laser therapy or ethanol injections. The diffusion of lesions was slight because the total acoustic energy delivered was minimal (see Table 1); therefore, there was no damage to surrounding tissues. Figures 3 and 4 show that pulses may be fired adjacent to the trachea without producing lesions. Due to the minimal diffusion of the energy into surrounding tissue, the safety distance with HIFU is much smaller than with other techniques such as ethanol or lasers for which the minimal distance is at least 1.5 cm (17).
Based on these results, we conclude that it is possible to target and destroy local foci of thyroid tissue using the HIFU treatment without side effects. However, some limitations of the animal model should be kept in mind when extrapolating these data to humans. The dimensions of the ewe thyroid and the distances from surrounding structures are about two-thirds shorter than in humans. The risk of skin burns is likely to be lower in clinical trials in humans because the human thyroid is located deeper than its counterpart in the ewe. The HIFU parameters will have to be adjusted to deliver the optimal energy to the area to be destroyed. Moreover, due to the absence of thyroid nodules in the ewe, the device has been tested only on healthy thyroid tissue. It remains unknown whether HIFU will be as effective in destroying human thyroid nodules, which may have a different density and structure than normal tissue: The diffusion of energy in such nodules is not known. These characteristics will have to be determined before human trials. As with the other methods, precise targeting is essential to prevent damage of adjacent structures.
In conclusion, the modified HIFU device designed to induce thyroid lesions was able to induce coagulative necrosis in the targeted thyroid tissue of ewes. These experiments indicate that noninvasive HIFU-induced ablation of human thyroid nodules is a promising possibility in the near future and merits further study.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.