
Abstract

Ectopic thyroid carcinoma is a rare phenomenon and papillary thyroid carcinoma (PTC) arising in a branchial cleft cyst is extremely rare. Here we report a patient with PTC in a branchial cleft cyst. There was no evidence of a PTC in the thyroid itself. We also discuss the utility of measuring thyroglobulin (Tg) in fine-needle aspiration (FNA) fluid.
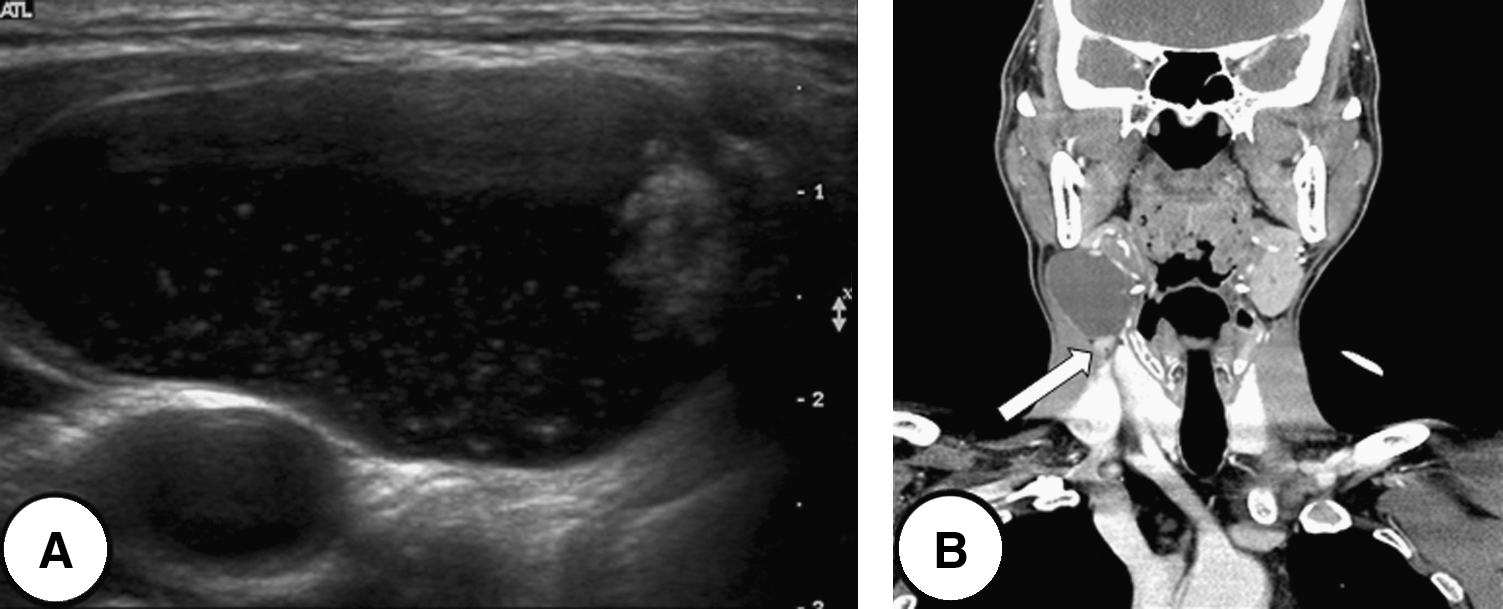
A 49-year-old man presented with a lateral neck mass that had been present for 2 months. On clinical examination, the mass measured 3 × 4 cm in diameter. Thyroid function testing revealed a euthyroid state. Neck ultrasonography showed a cystic mass with a solid component and computed tomography scans demonstrated 3.2 × 2.3 × 4.5 cm cystic mass with a focal solid component of high density in the right neck, involving levels II and III. The right submandibular gland and sternocleidomastoid muscle were compressed as a result of mass effect (Fig. 1). FNA of the cyst was performed and the needle used was immediately washed with 1 mL of normal saline for measuring Tg. FNA cytology showed scanty cellularity without any identifiable tumor cells. FNA-Tg was assayed using a monoclonal antibody immunoradiometric assay. The level of Tg in the washout fluid was 283 ng/mL. There were no pathologic findings in the thyroid gland on neck ultrasonography and computed tomography scans. The cyst was excised, and the frozen section revealed PTC. Therefore, a total thyroidectomy with selective right neck dissection was performed. Histopathology revealed that the cyst was representative of a typical branchial cleft cyst, lined by a single layer of epithelium with lymphoid tissue located beneath the epithelium. The solid component of the cyst showed papillary projections. The papillae were composed of tumor cells, demonstrating eosinophilic cytoplasm with a typical ground-glass nucleus, overlapping nuclei, nuclear grooves, and intranuclear inclusions (Fig. 2). The papillary carcinoma within the branchial cleft cyst was positive for both Tg and thyroid transcription factor-1 (TTF-1) immunostaining. Normal thyroid tissue was observed within the cyst wall adjacent to the focus of papillary carcinoma. The surgical specimen, including the thyroid gland and lymph nodes, was extensively examined, but no evidence of an occult PTC was identified. A diagnostic radioiodine whole body scan found no evidence of metastasis.
(

Light microscopy shows (
Ectopic thyroid tissue within a branchial cleft cyst is a rare phenomenon, and a carcinoma within this tissue is very rare. Branchial cleft cysts have been considered as the most common congenital anomalies among neck masses. However, the pathophysiology of branchial cleft cysts has become controversial. Most authors maintain that branchial cleft cysts result from incomplete involution of the branchial cleft structures during embryonic development. Conversely, a recent theory proposed that these lesions are associated with epithelial cell penetration of the lymph nodes in the branchial cleft (1). Both theories may explain the presence of thyroid tissue within a branchial cleft cyst. The traditional theory is supported by the suggestion that the fourth branchial pouch follicular cells contribute to the lateral thyroid lobes (2). The presence of persistent branchial pouch remnants that have failed to fuse with the descending thyroid may explain its location within a branchial cleft. It could account for ectopic thyroid tissue within a congenital branchial cyst. The new theory alludes to benign thyroid epithelium lying within a cervical lymph node, stimulating cystic degeneration. This theory is supported by the presence of a dense lymphoid infiltrate beneath the epithelium (3). This may also explain the presence of ectopic thyroid tissue within an acquired branchial cleft cyst. Given these points of view regarding pathophysiology, it is reasonable to assert that, as there was no primary tumor within the whole thyroid gland, and no metastatic lesion in the lymph nodes despite extensive histological examination, our patient had a PTC arising in ectopic thyroid tissue within a branchial cleft cyst.
PTC frequently manifests as a cystic nodal mass mimicking a cyst. In up to 20% of patients with thyroid carcinoma, the primary diagnosis is made by lateral cervical cyst evaluation (4). In clinical settings, FNA cytology is routinely performed for the evaluation of cysts. However, cysts yielding inadequate/nondiagnostic FNA cytology could be misinterpreted as benign cervical cystic masses or simple branchial cleft cysts, thereby delaying correct diagnosis and appropriate treatment if a PTC is present (5). In previous reported cases of PTC (6,7) within a branchial cleft cyst, FNA cytology did not reveal PTC in the cysts. Therefore, only the cysts were surgically resected and it was not until after histologic evaluation that the PTCs were identified and thyroidectomies were performed. In our patient, FNA cytology also showed scanty cellularity without diagnostic information. However, Tg was also measured in the FNA washout fluid with the result strongly suggesting metastatic differentiated thyroid carcinoma. Tg may be detected in FNA washout fluid from reactive nonmetastatic cervical lymph nodes, but there are no reported false-positive results for PTC when the Tg is greater than 100 ng/mL in the Tg washout fluid (8). In such cases, the tumor is generally considered to be a cystic nodal metastasis from an occult PTC rather than malignant transformation of benign thyroid tissue within a cyst (9). In our patient we decided to perform a total thyroidectomy with lateral neck dissection that included the cyst because of the elevated Tg in the FNA sample, even though the preoperative imaging studies of the thyroid gland were negative. During surgery, a frozen section of the cyst confirmed PTC.
It is difficult to determine if a PTC in a branchial cleft cyst represents metastatic thyroid carcinoma with missed primary tumor or ectopic thyroid carcinoma arising in a branchial cleft cyst. In our patient, there was neither an occult primary carcinoma within the whole thyroid gland nor evidence of metastasis in 27 regional lymph nodes, despite extensive histologic examination. Currently, only one patient with ectopic PTC in a branchial cleft cyst without evidence of a PTC within the thyroid has been reported (6). However, there was no comment regarding lymph node dissection and pathology in that report. To our knowledge, ours is the only report of a PTC in a branchial cleft cyst without evidence of a primary tumor in the thyroid gland and no metastasis in lymph nodes.