
Abstract
Background:
The occurrence of recurrent papillary and follicular thyroid carcinomas is not unusual. Numerous studies have reported the association between risk factors of initial surgery and recurrence of papillary and follicular thyroid carcinomas. However, we do not have sufficient data to analyze the time of postoperative recurrence associated with therapeutic results and cancer mortality. We hypothesized that an early recurrence of papillary and follicular thyroid cancers implies a rapid growth of cancer resulting in high mortality rate.
Methods:
We conducted a retrospective study in a medical center in northern Taiwan. The investigation included 2148 cases of papillary and follicular thyroid carcinoma, including 325 recurrent cases during the period between 1977 and 2006. The studied cases were categorized into early or late recurrence groups. Cases with an early recurrence were defined as those in which recurrence occurred in the first year following thyroid surgery.
Results:
Tumor size, radioactive iodide treatment, multifocality, and tumor-node metastasis stage were independent predictors of recurrence. After a mean follow-up of 8.7 ± 0.1 years, death due to thyroid cancer was observed to occur in 105 (32.3%) recurrent cases. Among the 325 recurrent cases, early recurrence was detected in 185 cases, and late recurrence was detected in 140 cases. Early recurrence was mostly observed in older male patients; a high mortality rate was associated with these cases. Distant metastases were observed in about 80% of the cases in the early recurrence group, whereas localized metastases in the neck region were observed in more than half the cases in the late recurrence group. The percentage of patients with a non–disease-free status and distant metastases in the early recurrence group was higher than that in the late recurrence group. The 10-year disease-specific survival rates were 52.5% and 85.1% for the early and late recurrence groups, respectively.
Conclusions:
Early recurrent papillary and follicular thyroid carcinomas are associated with high mortalities. Tumor size and multifocality deserve consideration as indicators of recurrence. Therefore, patients whose primary follicular or papillary thyroid carcinoma has features associated with early recurrence should probably receive more aggressive initial treatment.
Introduction
Materials and Methods
During the period between 1977 and 2006, 2148 patients with papillary or follicular thyroid cancers were treated at the Chang Gung Memorial Hospital in Linkou, Taiwan. All patients were followed closely, and detailed information was available for each patient. Of these subjects, 1910 had papillary and 238 had follicular thyroid carcinomas. Patients who had previously received surgical treatment(s) for thyroid cancer at another hospital were excluded. Tumors were staged using the International Union Against Cancer (UICC)–Tumor-Node Metastasis (TNM) criteria (6th edition) (8). Pathologic review was performed for all thyroid carcinomas according to the standards of the World Health Organization (9). For comparison purposes, patients were categorized by clinical class (10). Long-term thyroid hormone replacements or suppressive treatments were provided following surgery. Radioactive iodide (131I; 2–5 mCi) whole body scans and chest X-rays were performed to identify local or distant recurrences. Serum thyroglobulin (Tg) values were determined at 6–12-month intervals.
Cases with suspected recurrence received neck ultrasonography with fine-needle aspiration biopsy and cytology (FNAC) (11) computed tomography scans, fluorine-18 fluorodeoxyglucose positron emission tomography (FDG-PET), or other noninvasive diagnostic imaging studies, such as bone scans or 201Tl scans, depending on clinical condition. Recurrence was stratified according to a cytologically or histologically diagnosed group (A), a 131I diagnostic group (B), or another imaging diagnostic group (C). Cases recurring postoperatively were further classified into the early or the late recurrent group. The early recurrent group was defined as comprising patients with cancer tissue that persisted following surgery or other adjuvant therapy. This group included patients with distant metastases detected by a 131I whole body scan within 1 year after thyroid surgery. By contrast, the late recurrent group comprised patients with cancer recurring at more than 1 year after primary thyroid surgery and 131I ablation therapy. Of the 325 recurrent cases, 149 received external radiotherapy.
Postoperative serum Tg concentrations were measured with an IRMA kit (CIS Bio International, Gif Sur Yvette, France). Surgery, 131I therapy, or external radiotherapy was performed upon detection of metastatic or recurrent lesions. At the end of the analytical period, lack of relapse was defined as a negative 131I whole body scan and no local or distant metastasis was identifiable via noninvasive examinations. The study was approved by the Institutional Review Board Chang Gung Memorial Hospital. All data are expressed as means ± standard error of the mean. Univariate and multivariate statistical analyses to determine the significance of various factors were performed using the Kaplan–Meier method and the log-rank test (12). The level of statistical significance was set to p < 0.05. Additionally, survival rates were calculated using the Kaplan–Meier method, and differences in survival rates were examined using the Breslow and Mantel–Cox tests.
Admission records were surveyed and coded in computer for the following data (13): age, gender, primary tumor size, ultrasonographic findings, fine-needle aspiration cytology results, surgical methods, histopathologic findings, TNM staging, 1-month postoperative serum Tg levels, presence of Tg antibody, results of investigations, therapeutic 131I scanning, 131I accumulated dose, postoperative recurrence, analysis of distant metastases as detected by noninvasive radiological and nuclear medical studies, treatment outcomes, causes of death, and survival status. Patients with recurrence were identified from the established database.
Results
Table 1 lists the clinical features of 2148 patients with papillary and follicular thyroid cancer. Subjects with follicular thyroid carcinomas were older than those with papillary thyroid carcinomas, but no gender difference was observed as thyroid carcinoma type. Of the 2148 patients with papillary or follicular thyroid carcinomas, the tumor was confined to the thyroid in 1390 cases (64.7%). Mean tumor size was 2.60 ±0.04 cm; however, follicular thyroid carcinomas were significantly larger than papillary thyroid carcinomas (4.10 ± 0.20 and 2.40 ± 0.04 cm, respectively; p < 0.0001). The presence of follicular thyroid cancer was associated with higher cancer-specific mortality when compared with papillary thyroid carcinoma (18.5% and 3.5%, respectively). Postoperative recurrence was observed in 15.1% (325 cases) of the 2148 cases of follicular and papillary thyroid carcinoma after a mean follow-up period of 9.0 ± 0.4 and 8.1 ± 0.1 years, respectively.
Case number.
Serum thyroglobulin without thyroxine treatment.
TNM, tumor-node metastasis; Post-op, postthyroidectomy; Tg, thyroglobulin.
Figure 1 illustrates the subcategorization of the recurrent early and the recurrent late groups according to the region of recurrence and the mortality rates associated with each subcategory. Nearly 80% of cases in the early recurrent group had distant metastases, whereas more than half of cases in the late recurrent group had cancers detected in the local-regional neck area. Distant metastases were associated with highest mortality rates (47.8%) in the early recurrent group, whereas local with distant metastases were associated with highest mortality rates (42.3%) in the late recurrent group. Figure 2 presents the distribution of patients with early and late recurrent thyroid cancer into subgroups according to the method of diagnosis. The diagnostic method employed depended on the clinical condition of the patient. Over half of the cases (173/325; 53.2%) were confirmed by cytological or histological examinations. Most histological or cytological diagnoses were confirmed by local-regional neck surgery. Cytopathological or 131I scans were used to diagnose 283 of 325 cases (87.1%). Only 42 cases were detected by imaging methods other than 131I scan; of these 42 cases, all presented with elevated serum Tg values.
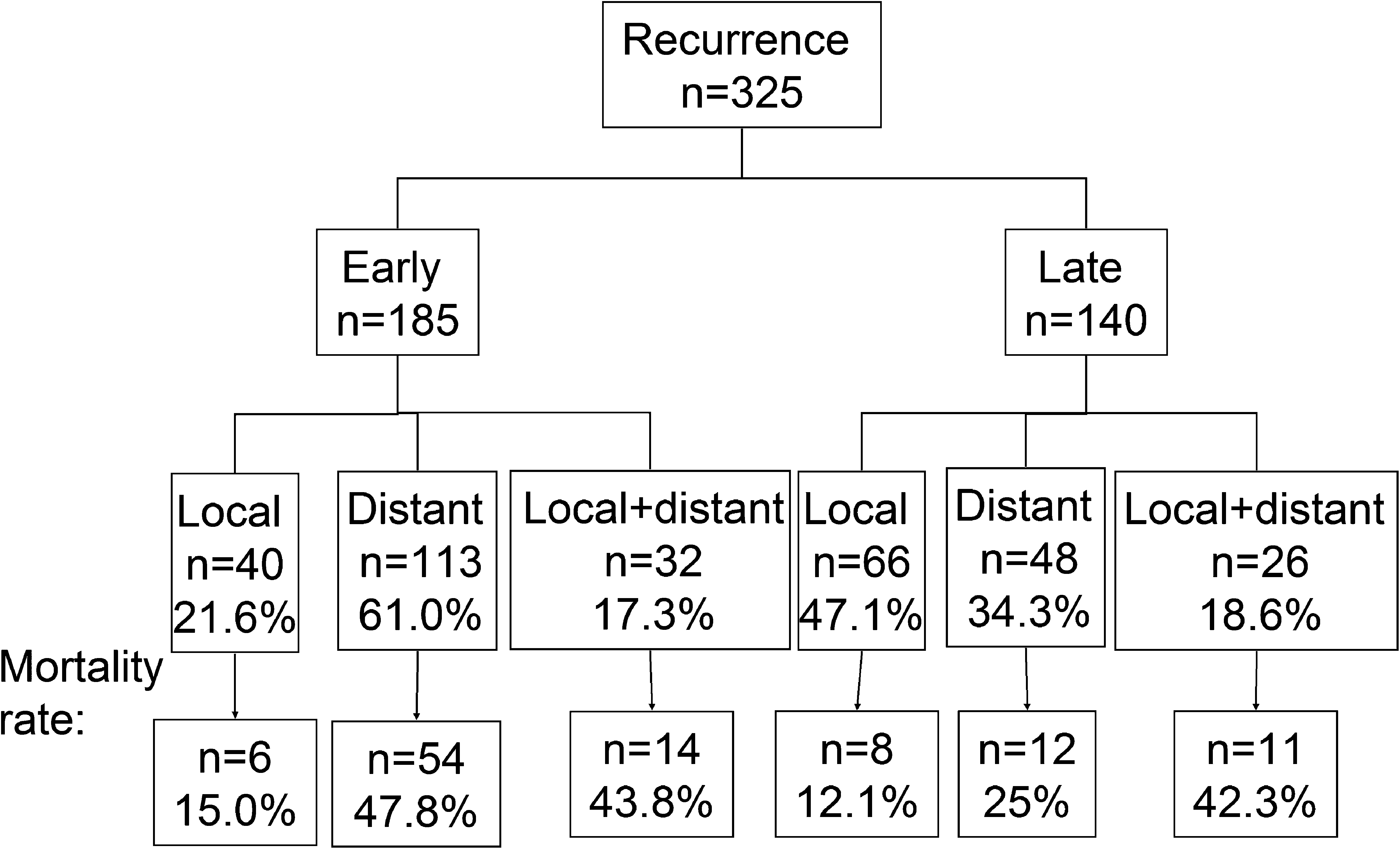
Subcategorization of early and late recurrent cases of thyroid cancer according to the region of recurrence and the mortality rates associated with each subcategory.
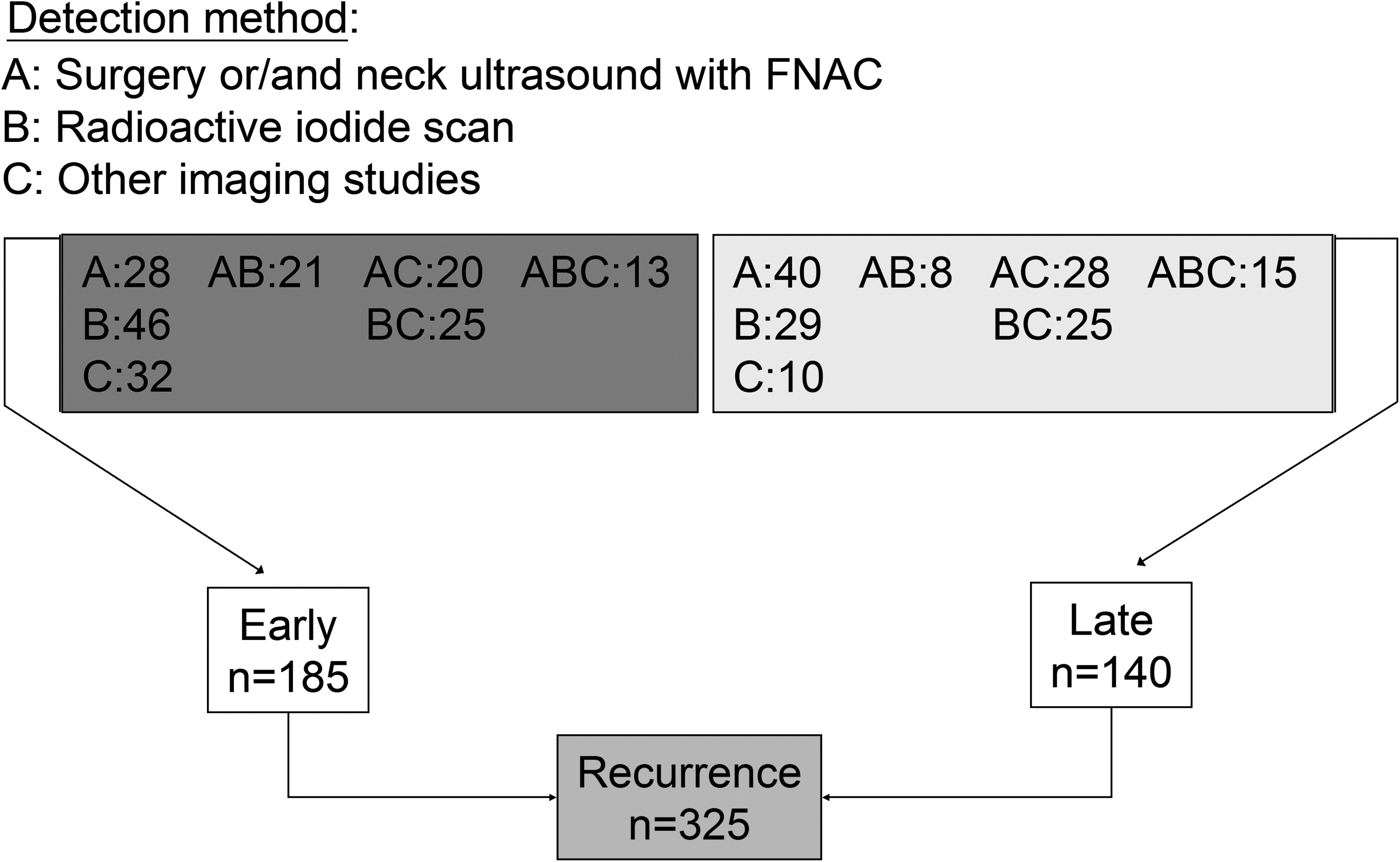
Categorization of patients with early and late recurrent thyroid cancer into subgroups according to the method of diagnosis.
Multiple regression analysis was performed to identify independent factors in cases of postoperative recurrence (Table 2). Survival, tumor size (2 cm), TNM stage, multifocality, and postoperative 131I cumulative dose were significant independent factors. In contrast, age, gender, postoperative Tg value, operative method, and histological type were not found to be significant factors with respect to postoperative cancer recurrence.
Serum thyroglobulin without thyroxine treatment.
Of the 325 cases of recurrent thyroid carcinoma, 140 were late recurrence and 185 were early recurrence. Table 3 presents the clinical features of patients in these two groups. The mean period between first thyroid surgery and detection of recurrence for late recurrent cases was 5.5 ± 0.4 years, with the longest period being 30 years. When compared with the late recurrent group, the early recurrent group was characterized by older age, male gender, higher postoperative Tg value, higher TNM stage including more lymph-node or soft tissue invasion, and higher cancer mortality. Cancer-specific mortality was 40% in the early recurrent group after mean follow-up of 5.5 years.
Case number.
Postthyroidectomy serum thyroglobulin without thyroxine treatment.
Of the 325 recurrent cases, 125 have survived and have a nonrelapsed status. After mean follow-up of 8.7 ± 0.1 years, 105 of the recurrent cases succumbed to thyroid cancer. Figure 3 presents Kaplan–Meier cancer-specific survival curves for all subjects with papillary or follicular thyroid carcinomas examined in this study. Survival curves for all subjects, those with papillary thyroid carcinomas, and those with follicular thyroid carcinomas are presented in Figure 3a, whereas curves for subjects with recurrent carcinomas, early recurrent carcinomas, or late recurrent carcinomas are presented in Figure 3b. Significant better survival was noted for papillary thyroid carcinoma than follicular thyroid carcinoma. The 5-, 10-, and 20-year survival rates were 66.0%, 52.5%, and 34.5%, respectively, for the early recurrent group, and 94.1%, 85.1%, and 60.2%, respectively, for the late recurrent group. The differences in survival rates were statistically significant. Survival curves for subjects with recurrent papillary, early recurrent papillary, and late recurrent papillary thyroid carcinomas are presented in Figure 3c, whereas curves for subjects with recurrent follicular, early recurrent follicular, and late recurrent follicular thyroid carcinomas are presented in Figure 3d. For patients with either recurrent papillary or recurrent follicular carcinomas, survival was greater in the late recurrent groups when compared with the early recurrent group.
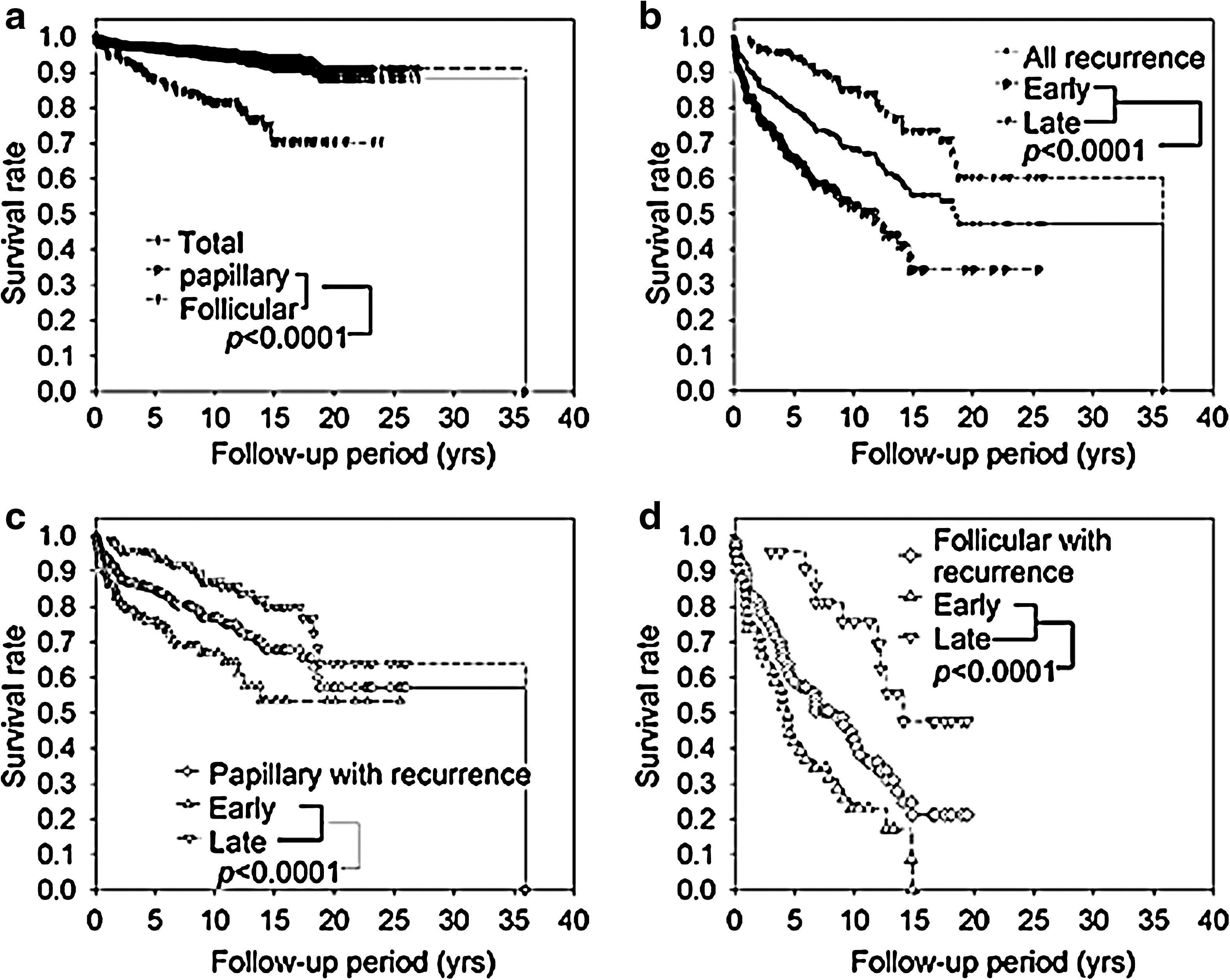
Thyroid cancer-specific survival rates as a function of thyroid cancer type, early recurrence, and late recurrence. (
Subjects with recurrent thyroid carcinomas were subdivided into “survival” and “mortality” groups, and the characteristics of these two groups are presented in Table 4. When compared with the survival group, the mortality group was characterized by older age, male gender, larger tumor size, less aggressive surgery, and more treatment with external radiotherapy. Cumulative 131I dosage was not significantly different between the two groups.
Case number.
Serum thyroglobulin without thyroxine treatment.
op, operation-thyroidectomy; RT, external radiotherapy.
Discussion
Diagnostic and therapeutic strategies for recurrent papillary and follicular thyroid carcinomas differ significantly from strategies for the initial management of primary thyroid tumors. During initial thyroid surgery for primary tumors, it is essential to identity patients at high risk for cancer recurrence. Most high-risk papillary and follicular thyroid carcinoma patients receive 131I ablation therapy (13). Micrometastases are detectable during the first postsurgical year through whole body therapeutic or diagnostic scanning. The detection of cancer recurrence depends on tumor cancer burden and methods selected for detection.
The size of papillary thyroid carcinoma nodules is the first and most important piece of information used by clinicians in planning for treatment of these cancers (14). The findings of our investigation confirm those of Rosário et al. (15), in which the patients with small papillary thyroid carcinomas (2 cm or less) who do not exhibit extrathyroidal invasion or lymph-node metastases, who have no history of radiation to the head and neck, and who show an absence of a family history of thyroid cancer are at very low risk. In multiple regression analysis using a tumor size of 2 cm as the criterion for classification of patients, application of the TNM staging system revealed that tumor size is an independent factor for tumor recurrence (8). A multifocal histological pattern is another important independent factor for cancer recurrence. Although mutifocal papillary thyroid carcinoma and other histological variants were not categorized in the TNM stage system, recent reports are consistent with an association between multifocal papillary thyroid carcinoma and cancer recurrence (16). Aggressive therapeutic strategy is indicated for these cases.
Age, method of detection, extent of recurrence, and curability are important factors in predicting the outcomes of patients with recurrent papillary or follicular thyroid carcinomas (17). In our study, more aggressive surgical procedures predicted considerably lower mortalities in recurrent cases but did not influence recurrence rates. Therapeutic results may differ according to histological findings and TNM staging. The findings of our study indicate that early recurrent cases have a worse prognosis than late recurrent cases, and that cases of recurrent follicular thyroid carcinoma have a worse prognosis than cases of recurrent papillary thyroid carcinoma.
Histopathological diagnosis for all forms of recurrent thyroid cancer is difficult in clinical practice. The priorities for diagnosis of recurrent papillary and follicular thyroid cancer, in decreasing order, are histology, cytology, 131I uptake, and other imaging diagnostic tools. Our investigation retrospectively evaluated patients with papillary and follicular thyroid cancers over a period of ∼30 years. Therefore, the diagnostic methods applied to these patients were found to vary as new techniques were introduced. Scanning methods such as 201Tl, bone scans, and computed tomography were used more frequently in the earlier years of this study (18); FDG-PET, in contrast, was utilized in the more recent years. Neck ultrasonography with FNAC and diagnostic or therapeutic 131I scans were also employed during the study period. The diagnostic procedures used to determine tumor recurrence included ultrasonography, FNAC, 131I scans, FDG-PET, and other imaging methods (4,19,20). Ultrasonography with FNAC is considered the most sensitive method for detecting local recurrences and regional lymph node metastases. Otherwise, for recurrent cases with lymph nodes smaller than 1 cm or with deep-seated lymph nodes, other localization image studies are needed. FDG-PET is valuable in cases involving negative 131I scanning results and elevated serum Tg values (19). When lymph node metastases are identified during the initial thyroid surgery, high rates of recurrent lymph node metastasis are expected (21). In our study, the early recurrent group exhibited a higher incidence of distant metastases than the late recurrent group. When recurrence of papillary or follicular thyroid carcinomas was suspected at 1 year after the initial thyroid surgery, recurrence in the local-regional area was found to have occurred in 65.7% of cases.
Diagnostic and therapeutic 131I scans and methods for measurement of serum Tg concentrations are important follow-up surveillance tools for determining the recurrence of papillary thyroid carcinomas. The patients treated initially for papillary thyroid carcinomas are considered to be disease-free if 131I scans are negative, serum Tg is undetectable, and Tg antibodies are absent (13,22). In this regard, however, controversy currently exists regarding the adequacy of one-time negative 131I results and the sensitive of currently available Tg assay kits (23). Additionally, the complications or side effects that may occur after use of 131I in excess of 1000 mCi represent current concerns. In our study, most cases with a nonrelapsed status did not meet the criteria for disease-free survival; in particular, serum Tg values were detectable in the majority of these cases.
Surgical treatment for local-regional early or late recurrent thyroid cancers and 131I therapy for distant thyroid cancer metastases are currently considered the optimal therapies (24 –26). For treatment of concurrent local-regional and distant metastases, various surgical procedures, the appropriate therapeutic dose of 131I, external radiotherapy, and other therapeutic strategies represent controversial issues. Neck dissection for concurrent local-regional and distant metastases may temporarily reduce Tg values; however, long-term follow-up is essential to ensure patient survival (27). In cases of repeated neck surgery with involvement of the aerodigestive tract, disease-free survival without complications is difficult to achieve.
In conclusion, recurrent papillary and follicular thyroid carcinomas are associated with high mortality rates and are difficult to eradicate. Cases of early recurrent carcinomas detected during the first postoperative year have a worse prognosis than cases of late recurrent carcinomas. Tumor size and multifocality are important indicators of recurrence.
Footnotes
Acknowledgment
This work was supported by grants from the National Science Council in Taiwan (NSC 97-2314-B-182A-038-MY3 to J.-D.L.).
Disclosure Statement
The authors declare that no competing financial interests exist.