
Abstract
Background:
Ectopic thyroid tissue can be found anywhere between the foramen cecum and the normal position of the thyroid gland, most commonly located in the anterior cervical area, the region of the thyroglossal duct. Although thyroid cancer has been described frequently in thyroglossal duct remnants, thyroid dysfunction related to this tissue is rare. We report a patient with recurrent Graves' disease arising in a thyroglossal duct remnant.
Summary:
A 40-year-old woman with a history of total thyroidectomy for Graves' disease, presented with a slowly enlarging midline neck mass in association with clinical signs of hyperthyroidism. Serum-free triiodothyronine (6.6 pg/mL) and serum-free thyroxine (2.2 ng/dL) were elevated (normal range, 2.3–4.2 pg/mL and 0.9–1.8 ng/dL, respectively), and thyroid-stimulating hormone was suppressed (<0.01 mIU/mL; normal range, 0.35–5.50 mIU/mL). Neck ultrasonography showed a solid mass, localized at the infrahyoid area; radionuclide scanning confirmed an increased uptake at the same level. A 4 cm solid mass was removed by the Sistrunk technique. Microscopic examination revealed marked follicular hyperplasia, with tall cells, small follicles, scant, and scalloped colloid, in association with patchy lymphocytic infiltrate consistent with Graves' disease.
Conclusions:
There appears to be no reason why thyroid cells within thyroglossal duct remnants should not be influenced by the thyroid-stimulating immunoglobulins of Graves' disease. Thyrotoxicosis resulting from this must be very rare, however, as were unable to find reports of patients with thyrotoxicosis due to Graves' disease in thyroglossal duct remnants. Although some thyroid tissue can be found within the thyroglossal duct in 1.6% to 40% of normal adults, the risk of thyroid dysfunction from this is far too low to justify new therapeutic approaches.
Introduction
Patient
A 40-year-old woman presented with general weakness, palpitations, and a slowly enlarging painless mass in the midline of 3-month duration. She did not complain of dysphagia, odynophagia (i.e., painful swallowing), or inflammatory signs. She had undergone total thyroidectomy, 4 years previously, for Graves' disease with a huge diffuse toxic goiter extending down into the superior mediastinum associated with airway compression. Her past laboratory values were as follows: free triiodothyronine (FT3): 6.5 pg/mL (reference range [RR], 2.3–4.2 pg/mL); free T4 (FT4): 2.8 ng/mL (RR, 0.9–1.8 ng/mL); and TSH: <0.01 mIU/mL (RR, 0.35–5.50 mIU/mL). High levels of anti-thyroglobulin antibody (1807 IU/mL; RR, <40 IU/mL), along with anti-thyroid peroxidase antibody (575 IU/mL; RR, <35 IU/mL), were also present. Her thyrotropin receptor antibody (TRAb) was slightly elevated (10.8 IU/mL; RR, 0–10 IU/mL). 99m-TC thyroid scintigraphy showed an enlarged thyroid with homogeneous uptake throughout the gland in conjunction with 65.4% uptake at 24 hours, without any activity outside the thyroid bed. After surgery she was immediately treated with substitution T4 therapy (0.1 mg/day). The follow-up schedule consisted of neck examination and determination of serum TSH values every 6 months for the initial 2 years and then annually. Her physical examination at the time she presented now revealed a 4 cm fibroelastic nontender midline neck mass that moved upward with the protrusion of the tongue and during swallowing. There was no cervical lymphadenopathy. Thyroid function tests revealed elevated serum levels of FT3 (6.6 pg/mL) and FT4 (2.2 ng/mL) with a low TSH level (<0.01 mIU/mL), confirming a clinical picture of thyrotoxicosis. TRAb was within the normal range (9.12 IU/L), anti-thyroglobulin autoantibody was 1807 IU/mL, and anti-thyroid peroxidase was 456 IU/mL. The patient shortly discontinued substitution T4 therapy. After a month, thyroid blood tests demonstrated the persistence of hyperthyroidism (FT3, 6.3 pg/mL; FT4, 2.3 ng/mL; TSH, <0.01 mIU/mL). Neck ultrasonography showed a hypoechoic solid mass, 4.5 × 3 × 1.5 cm in dimension, localized at the infrahyoid area without evidence of any residual thyroid parenchyma (Fig. 1). Power-Doppler examination highlighted diffuse hypervascularity as reported in Graves' disease. 99m-TC radionuclide scanning confirmed an increased uptake at the same level, evidence for autonomy. No activity was demonstrated to correspond with the thyroid bed (Fig. 2). The patient was rendered euthyroid preoperatively with anti-thyroid medication (i.e., methimazole for 2 weeks). At operation a thick mass connected by a stalk to the hyoid bone was observed; the patient was submitted to the Sistrunk procedure that involved an en bloc resection of the mass, body of hyoid, and the suprahyoid tract to the foramen cecum (Fig. 3). Microscopic examination of the specimen revealed marked follicular hyperplasia, with tall cells, small follicles, scant, and scalloped colloid, in association with patchy lymphocytic infiltrate (Fig. 4). A diagnosis of Graves' disease recurrence was made. The postoperative course was uneventful, and the patient was discharged at the second postoperative day.
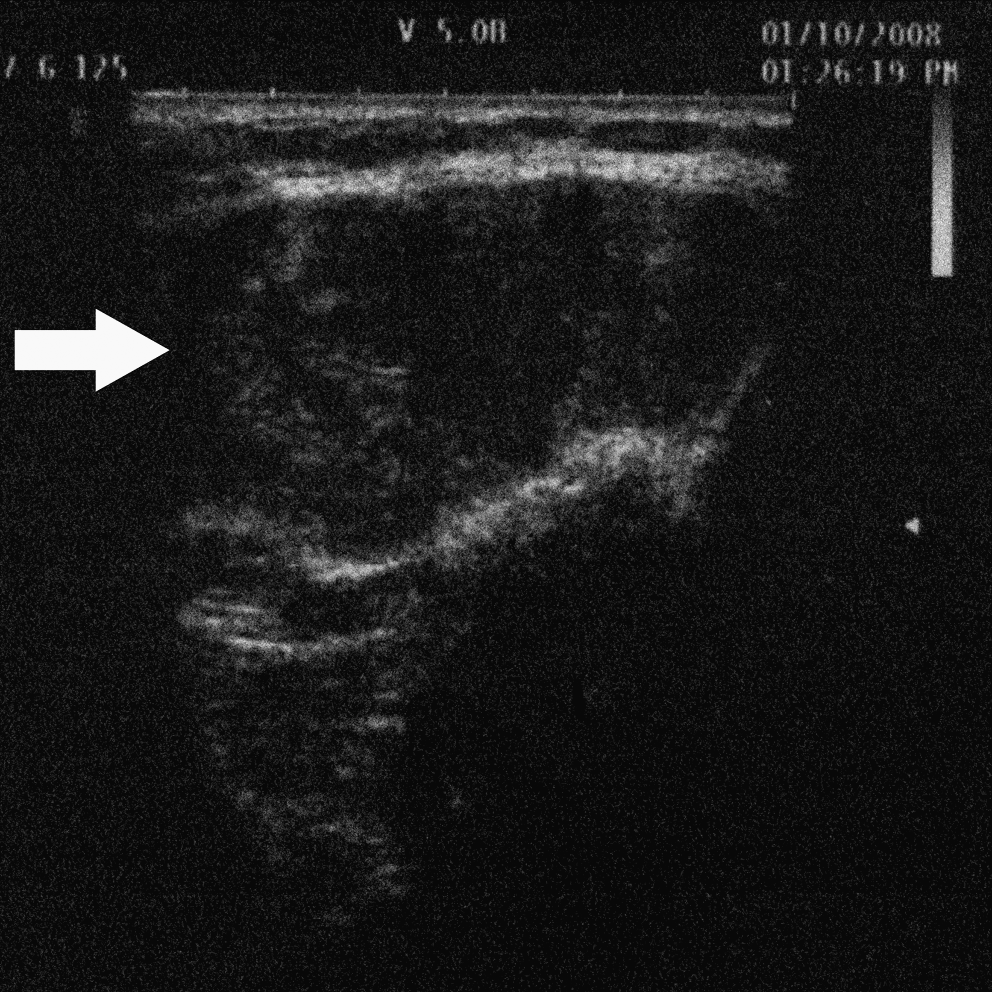
High-resolution ultrasonography shows a 4.5 × 3.0 × 1.5 cm hypoechoic mass at the infrahyoid area (arrow).
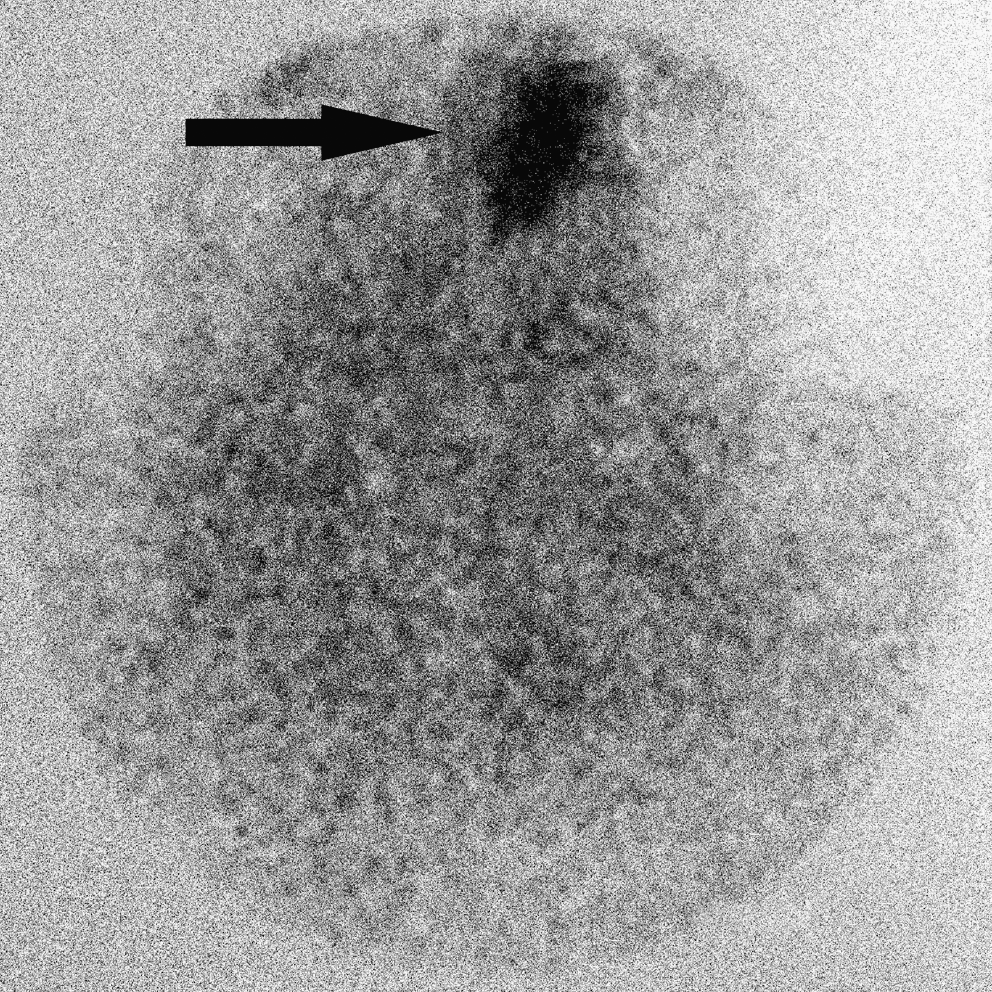
Pertechnetate scintigraphy highlights an increased uptake at the infrahyoid area (arrow) without any activity in correspondence of thyroid bed.

Surgical specimen: en bloc resection of the mass; parenchyma is diffusely swollen and hyperemic.
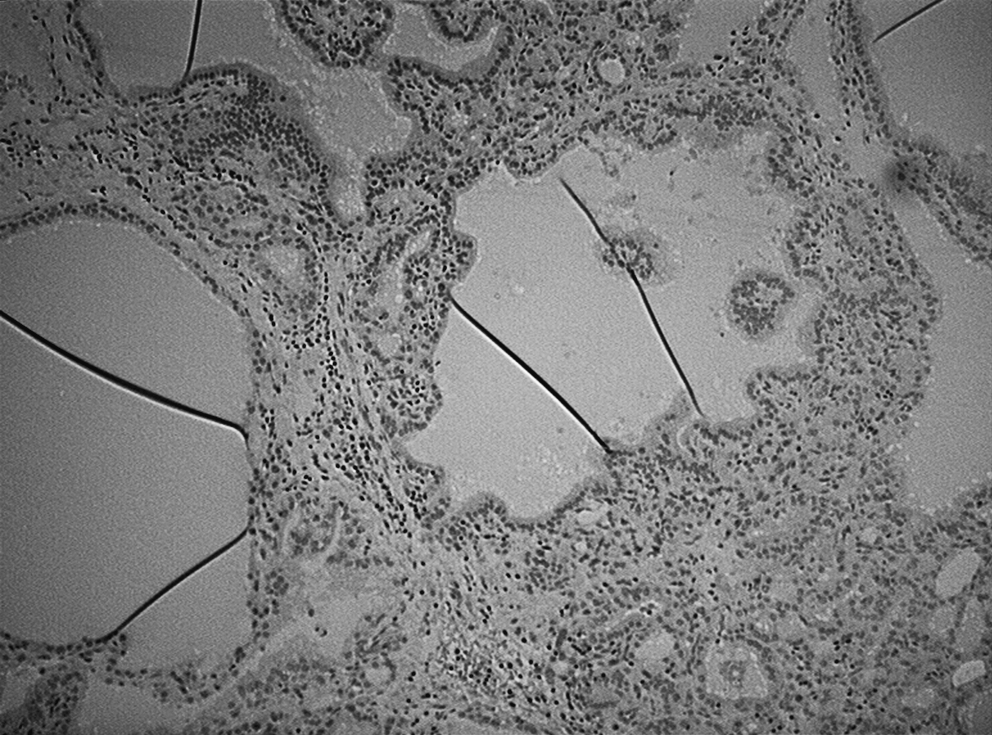
Pathologic examination showing diffuse thyroid hyperplasia with tall cells, small follicles, scant, and scalloped colloid in association with patchy lymphocytic infiltrate (hematoxylin & eosin; magnification, × 10).
Discussion
The thyroglossal duct is an embryological anatomical structure that forms the connection between the initial area of development of the thyroid gland and its final position. During normal embryonic development, the median thyroid migrates caudal from the area of the foramen cecum, through the second branchial arch to its permanent location in the neck. This migration sets the stage for development of a thyroglossal duct cyst and tumors. Normally, the stalk between the embryonic pharynx and the thyroid ruptures and obliterates during the migration process. However, in an unknown number of cases, a solid cord of cells persists. If a tumor or a cyst occurs, it is usually a midline mass that moves with swallowing and protrusion of the tongue. These tumors are of the epithelial remnant of the thyroglossal tract and present characteristically as a midline cervical mass at the level of the thyrohyoid membrane. The mass usually arises below but may be at the level of, or above, the hyoid bone. The differential diagnosis includes dermoid cyst, epidermoid cyst, branchial left cyst, lymph nodes, and soft tissue tumors generally. The diagnosis may be established by asking the patient to protrude his or her tongue; when the tongue is protruded, thyroglossal duct tumors move upward. Recurrent hyperthyroidism after surgery for Graves' disease is due to persistence of the underlying pathophysiologic mechanism, which can act on thyroid remnants if these are sufficiently large (8). A search of the MEDLINE databases from 1970 to 2008 was performed. The following key words were used: Graves' disease recurrence, thyroglossal duct remnants, thyroglossal duct cyst, and thyrotoxicosis. This review revealed only rare cases of thyrotoxicosis and Graves' disease in thyroglossal duct remnants in patients with thyroid gland in situ. None of the studies showed a relapse after total thyroidectomy. The possible presence of small accumulation of thyroid tissue in thyroglossal duct remnants could justify a risk of relapse, as these cells behave the same way as remnants after subtotal thyroidectomy. Since the size of the thyroid remnant is the most powerful factor associated with postoperative relapse, surgeons have gradually changed thyroid remnant size to reduce the relapse rate (9). The TSH receptor antibody has been noted as an immunologic marker or an essential cause of Graves' disease and has been reported to be useful for diagnosing and monitoring the clinical course of the disease. Some authors have shown that the TSH receptor antibody level and the antimicrosomal antibody titer are related to postoperative recurrent hyperthyroidism. However, concerning the TSH receptor antibody level, some reports have noted that the preoperative TSH receptor antibody level could not predict the long-term outcome of surgically treated patients with Graves' disease (10). In the patient reported here, TRAb were within the normal values. Although it is a single clinical observation, however, as it is possible that the biological potential of Graves' disease in thyroglossal duct remnants is very similar to that of relapsing after subtotal thyroidectomy, we may remember this rare occurrence during patient management by considering a risk of recurrence regardless of the surgery performed.
Footnotes
Disclosure Statement
The authors have nothing to disclose and no competing financial interests exist.