
Abstract

Acute suppurative thyroiditis is a rare disease of the thyroid. In adults it is usually associated with the immunocompromised state. This is not always true, however. Here we present a patient whose acute suppurative thyroiditis progressed to fatal necrotizing mediastinitis. She highlights the need for early and aggressive management in patients within whom the differential diagnosis includes acute suppurative thyroiditis, even if they are otherwise healthy.
A 37-year-old mother, previously fit and healthy, presented with a 3-day history of sore throat, fever, generalized malaise, and dysphagia. She had a right-sided tender and erythematous thyroid swelling. Laboratory analysis showed raised inflammatory markers with a C-reactive protein of 704 mg/L (normal range: <20 mg/L) and a white cell count of 11.8 × 109/L (90% neutrophils). The results of thyroid function tests were unremarkable with thyroid-stimulating hormone level 4.3 mU/L (normal range: 0.3–3.3 mU/L) and free T4 of 20 pmol/L (normal range: 10–25 pmol/L). Thyroid autoantibodies were negative. Granulicatella adiacens was isolated from blood cultures taken on admission. The patient was commenced on intravenous clindamycin as she was allergic to penicillin.
An ultrasonography scan of the neck (Fig. 1) demonstrated a gas-containing hypo echoic collection measuring 12 × 7 mm predominantly in the right lobe of thyroid gland in keeping with an abscess. No nodularity was noted in the background thyroid gland. The abscess was aspirated under ultrasound guidance. The aspirate grew mixed flora (alpha-hemolytic Streptococcus and Haemophilus influenzae). In the next 48 hours she developed systemic sepsis with pericarditis, bilateral pleural effusions, acidosis, and respiratory failure requiring transfer to intensive care unit. The antibiotic spectrum was broadened to vancomycin and gentamicin followed by ciprofloxacin and linezolid to cover the polymicrobial infection. Mechanical ventilation and inotropes were commenced. Computed tomography scan of the neck and chest revealed suppurative thyroiditis, mediastinal collections, bilateral pleural effusions, and lung consolidation. Mediastinotomy and drainage of suppurative collections were performed. Transoesophageal echocardiogram did not show any evidence of endocarditis. Subsequent chest and neck imaging demonstrated continued sepsis, and hence a repeat drainage of mediastinal abscesses was performed. Despite aggressive management, the patient died of severe sepsis and acute respiratory distress syndrome 20 days postadmission.
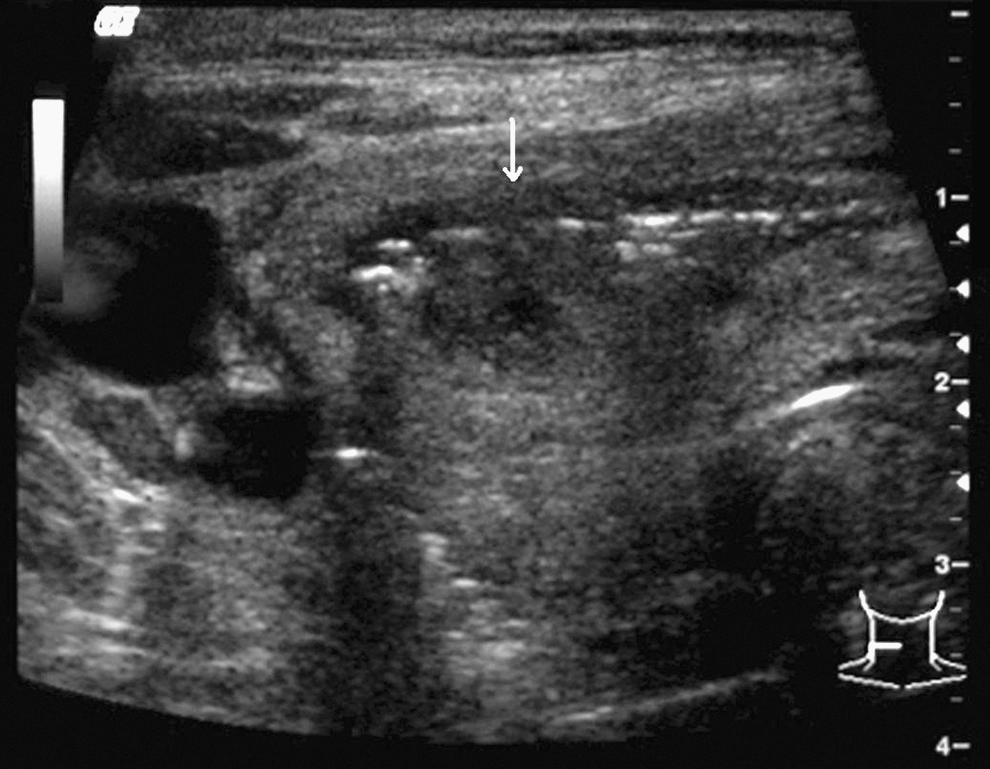
Ultrasonography image demonstrates gas-containing abscess (arrow) in the right lobe of the thyroid.
Acute suppurative thyroiditis is rare as the thyroid is high in iodine content, has a rich blood and lymphatic supply, and is protected by a capsule. The presentation varies from anterior neck swelling, sore throat, and fever to a more life-threatening fulminant infection. Causative agents are often gram-positive bacteria, such as Staphylococcus aureus. In adults, it is usually associated with immunocompromised state, trauma, or direct involvement by adjacent structures, whereas in the pediatric population it is usually secondary to a congenital abnormality of persistent pyriform sinus fistula or thyroglossal duct. The unusual features in our patient include fatal and rapidly progressive acute suppurative thyroiditis in a previously fit and healthy immunocompetent adult. The absence of any preexisting disease suggests hematogenous infection. G. adiacens infection is associated with high mortality with treatment failures and relapses being common. Granulicatella belong to a group of nutritionally variant streptococci that require pyridoxal for optimal growth. They are fastidious and their growth is enhanced by the presence of other organisms in the vicinity that provide essential nutritional support. However, the nutritional dependence does not hamper their virulence. On the contrary, they are highly pathogenic, and isolation from blood and other sterile specimens should alert clinicians about an ongoing suppurative process requiring prompt attention. Granulicatella produce a fibrillar adhesin that binds to the extracellular matrix proteins in tissues. They also have the ability to exist as L-forms. L-forms are devoid of cell wall. The ability to persist in a cell-wall-free state might make them tolerant to the cell wall active agents such as the β-lactam antibiotics. Comparatively, longer course of treatment is therefore advisable when treating infections due to Granulicatella. Synergy between penicillin and aminoglycoside has been documented, and vancomycin is also active (1). In this patient, polymicrobial infections with G. adiacens, alpha-hemolytic Streptococcus, and H. influenzae led to a highly pyogenic thyroiditis followed by unremitting widespread mediastinitis. This kind of mediastinal involvement, termed descending necrotizing mediastinitis, is a rare complication of thyroiditis (2). Although death from acute suppurative thyroiditis is rare, descending necrotizing mediastinitis, which can occur due to a number of other causes, has been associated with a high mortality (3).
In retrospect this patient teaches us that acute suppurative thyroiditis is a progressive and potentially fatal disease. Early diagnosis and appropriate antibiotic therapy is essential. Awareness of this condition and its potential complications is critical to aid prompt recognition of symptomatology and appropriate management. Early aggressive therapy should be considered to avoid fatal complications.