
Abstract
Background:
Perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS) are ubiquitous compounds that may act as endocrine disruptors, neurotoxic agents, and fetal development perturbing substances and may also be carcinogenic, as recently demonstrated in experimental animal models. There is little information on the potential for these compounds to affect the thyroid. Therefore, this study was performed to measure the intrathyroidal levels of PFOA and PFOS in surgical specimens of thyroid glands and to determine if there was a relationship between the concentrations of these substances and the clinical, biochemical, and histologic phenotype of the patients from whom the thyroids were obtained. We also sought to determine if there was a relationship between tissue and serum levels of both PFOA and PFOS.
Methods:
PFOA and PFOS were measured in 28 patients undergoing thyroid surgery for benign (15 multinodular goiters and 7 Graves' disease) and malignant (5 papillary and 1 follicular carcinoma) thyroid disorders.
Results:
PFOA and PFOS were detectable in all surgical specimens of thyroid tissue. Their median concentrations were 2.0 ng/g (range = 0.4–4.6 ng/g) and 5.3 ng/g (range = 2.1–44.7), respectively. Intrathyroidal concentrations of PFOA and PFOS were similar in the thyroids of patients with thyroid diseases as in thyroid glands obtained at autopsy. There was no relationship between the intrathyroidal concentrations of either PFOA or PFOS and the underlying thyroid disease. A significant correlation between the serum and the tissue levels of PFOS was found in all patients. The serum concentrations of PFOA and PFOS were significantly higher than those in the correspondent surgical specimens.
Conclusions:
These observations do not support the view that PFOA and PFOS are actively concentrated in the thyroid. PFOA and PFOS, however, are both found in surgical and autopsy thyroid specimens. Therefore, further studies to determine if they have disrupting effects in thyroid cells or tissue, and studies to compare populations with and without these compounds in their thyroid glands, are important.
Introduction
The recent demonstration that, in experimental animal models, PFOA and PFOS may act as endocrine disruptors, neurotoxic agents, and fetal development perturbing substances and may also have a carcinogenic effect has raised great concern as to their potential for harmful effects on human health (10 –19). For this reason, in 2006 the U.S. Environmental Protection Agency included PFOA and PFOS among dangerous compounds and reached a consent agreement with the industry to work voluntarily toward eliminating perfluorinated chemicals from emissions and product content by 2015. Epidemiological and toxicological data on PFAS were recently reviewed by Lau et al. (20). The role of PFOA and PFOS in human pathology is incompletely understood. The potential effects of PFAS as thyroid function disruptors were mainly investigated in the rat (12,21 –26). Several studies (12,21 –26) demonstrated a decrease in the serum levels of total thyroxine (T4) and triiodothyronine (T3) in PFOS-exposed rats, with no corresponding elevation of thyroid-stimulating hormone (TSH) through feedback stimulation of the hypothalamic-pituitary thyroid axis. Indeed, serum free T4 (FT4) levels in PFOS-treated rats were found to be comparable to those of controls (22). These findings are consistent with the hypothesis advanced by Gutshall et al. (24), suggesting that PFOS may act by displacing thyroid hormones from their binding proteins in the circulation. Similar changes in thyroid function parameters have not been reported in the few studies investigating humans exposed to PFOA (27,28) or PFOS (29).
In a previous investigation, we developed an assay method for the determination of PFOA and PFOS in human tissues obtained at autopsy (30). These tissues included endocrine glands, such as the thyroid, the pituitary, the gonads, and the pancreas. Significant concentrations of both compounds were found in all tissues that were tested. The demonstration that PFOA and PFOS could be detected in the thyroid gland prompted this study aimed at measuring the intrathyroidal levels of PFOA and PFOS in surgical specimens of thyroid glands. To this purpose, patients undergoing thyroid surgery for different thyroid diseases, both benign and malignant, were recruited. The intrathyroidal concentrations of PFOA and PFOS were related to the clinical, biochemical, and histologic phenotype of the patients to provide information on the possible role of PFOA and PFOS as endocrine disruptors.
Patients and Methods
The study group included patients who underwent thyroid surgery at the Department of General and Minimally Invasive Surgery, Fondazione Salvatore Maugeri I.R.C.C.S., Pavia, Italy. Twenty-eight patients (8 males and 20 females) were enrolled. Their median age (and range) was 50 years (33–78 years) (mean ± standard deviation = 51.9 ± 11.3 years). Near total or total thyroidectomy was performed in 5 patients for a toxic multinodular goiter, in 10 patients for a nontoxic multinodular goiter, in 6 patients for a differentiated thyroid cancer, and in 7 patients for Graves' disease. At histology, malignant thyroid nodules were diagnosed as papillary cancer in five cases and follicular cancer in one patient. Three patients with papillary cancer had a well-differentiated classic type carcinoma with poor mitotic activity, and two patients had a moderately differentiated papillary carcinoma with poor mitotic activity. Among the 10 patients with nontoxic multinodular goiter, 3 had circulating antithyroglobulin antibodies (TG-Ab) and antithyroperoxidase antibodies (TPO-Ab) and, at histologic examination, concomitant chronic autoimmune thyroiditis was observed.
Before surgery, all patients with toxic multinodular goiter and Graves' disease were treated with methimazole to achieve euthyroidism. Four patients with nontoxic nodular goiter were treated with levothyroxine at a TSH suppressive dose. All patients were Caucasian and the majority of cases lived in Pavia or in the nearby northern part of Italy. One patient was from Sicily. Sixteen patients lived in a rural and 12 in an urban area. Seven patients were housewives, 7 were manual workers, 12 were employees, and 2 were executives. Before surgery, all patients underwent a complete thyroid work-up at the Outpatient Clinic of the Unit of Internal Medicine and Endocrinology of the Fondazione Salvatore Maugeri. This included (1) clinical examination, including history regarding working activity, (2) the measurement of serum FT4, free T3 (FT3), and TSH, (3) the search for circulating thyroid antibodies; anti-TG-Ab, anti-TPO-Ab, and anti-TSH receptors antibodies, (4) an ultrasound (US) scan of the thyroid gland, with estimation of thyroid volume, thyroid parenchyma echogenicity, thyroid blood flow, size, and US characteristics of any nodule, and (5) fine-needle aspiration of nodules greater than 1 cm in diameter.
The control group consisted of thyroid tissue samples collected at postmortem examination from seven subjects (five men and two women). Their mean age was 32.5 ± 23.4 years (median: 25 years; range: 12–83 years), and all of them came from northern Italy. A negative history for thyroid disease was recorded in all cases and there was no evidence of thyroid disease at autopsy.
Serum samples for the measurement of PFOA and PFOS were drawn from 21 patients immediately before surgery. The control group consisted of serum samples from 10 subjects with no clinical, laboratory, or instrumental evidence of thyroid disease.
Informed consent, concerning the future use of clinical and pathological data for research purposes, was obtained from all patients included in this study. This was in accordance with the Institution Ethics Committee on human experimentation.
Hormone and autoantibody measurement
Serum concentrations of FT4 (normal range: 8.0–19.0 pg/mL), FT3 (normal range: 1.8–4.2 pg/mL), and TSH (third-generation TSH assay; normal range: 0.4–4.0 mIU/L) were measured using immunochemoluminescent assays by an automated analyzer (Immulite 2000; DPC Cirrus, Los Angeles, CA), employing commercial kits (Diagnostic Products Corporation, Los Angeles, CA). Serum concentrations of TG-Ab (normal range: <60 U/mL) and TPO-Ab (normal range: <60 U/mL) were measured using immunochemoluminescent assays employing commercial kits (Brahms, Hennigsdorf, Germany). TSH receptor antibodies were measured with a second-generation human TSH receptor assay (LIA TRAK human; Brahms) with a sensitivity of 1.0 U/L.
Measurement of PFOA and PFOS in tissue samples and sera
Serum samples were obtained from patients undergoing thyroid surgery and from control subjects. Samples of thyroid tissue were kept frozen at −80°C until the assay. The concentrations of PFOA and PFOS were measured as previously described (30). Briefly, thyroid tissues were homogenized using an Ultra Turrax TP 18/10 (250 mg tissue in 2 mL water); serum samples were then diluted with water (250 μL serum in 2 mL water).
Calibration curves were constructed using pools of tissue or serum samples. The five calibration standards were prepared by spiking tissues (2 mL homogenate) with PFOA and PFOS to final added concentrations of 0, 4.0, 16.0, 80.0, and 400.0 ng/g of tissue. Twenty microliters of internal standard (perfluoro nonanoic acid [PFNA], 2 mg/L in water, final concentration = 160 ng/g of tissue) were added to all samples. One aliquot of tissue homogenate was also processed without addition of PFNA (“tissue blank”), to check whether this compound was present in the tissues at measurable levels. PFNA can be detected in the blood of the general population (31); however, its concentrations are lower than 2 ng/mL, which could introduce a negligible (<1.25%) overestimation of the PFNA peak. Confirming these assumptions, no chromatographic peak occurred at the retention time of PFNA in tissue blanks.
Two milliliters of the homogenate was liquid–liquid extracted with acetonitrile and then purified using Sep-Pak tC18 (Waters, Milford, MA; 1 g/6 mL) and strong anionic exchange (Isolute, Argonaut Technologies, Redwood City, CA; 25 mg/1 mL) solid phase extraction cartridges. The resulting sample (25 μL) was injected into a high-performance liquid chromatography (HPLC)–mass spectrometry (MS). A calibration curve was constructed in the range of 0–400 ng/g of tissue. The analytical procedure was carried out using an Alliance 2695 HPLC system (Waters) coupled to a single quadruple Waters ZQ 2000 mass spectrometer. For quantitative analysis the MS detector was used with an electrospray ionization interface in negative ion mode, with acquisition in single-ion monitoring. The m/z ratios of 413.0 for PFOA, 499.0 for PFOS, and 463.6 for PFNA were recorded simultaneously. HPLC separation was performed on a mixed bed Waters XTerra® MS C18 column (4.6 [inner diameter] × 150 mm, 3.5 μm, kept at 28°C) by gradient elution with a mixture containing variable proportions of 3 mM ammonium acetate and methanol. The detection limits (signal-to-noise ratio = 3) were 0.1 ng/g for both PFOA and PFOS.
Statistical analysis
Statistical analysis was performed using SPSS software (SPSS, Evanston, IL). Between groups, comparisons were performed by Student's t-test for unpaired data and by Mann–Whitney U-test, according to a normal or a nonparametric distribution of the variable tested. Correlation between two variables was ascertained by Pearson and Spearman's correlation tests, as appropriate. Frequencies among groups were compared by χ 2 test with Fisher's correction, when appropriate. To test the effects of different variables independently of a covariate, binary linear regression analysis was used and partial correlation coefficients were computed. A p-value of < 0.05 was considered statistically significant.
Results
PFOA and PFOS were detectable in all surgical specimens of thyroid tissue, their median concentrations being 2.0 ng/g (range = 0.4–4.6 ng/g) and 5.3 ng/g (range = 2.1–44.7) for PFOA and PFOS, respectively. The concentrations of PFOA and PFOS in surgical samples from diseased thyroids were similar to those found in healthy glands obtained at autopsy. In the latter group the median concentrations of PFOA and PFOS were 1.5 ng/g (range = 1–6 ng/g) and 4.5 ng/g (range = 2.2–8 ng/g), respectively. The intrathyroidal concentrations of PFOA and PFOS were significantly related with each other (p < 0.001).
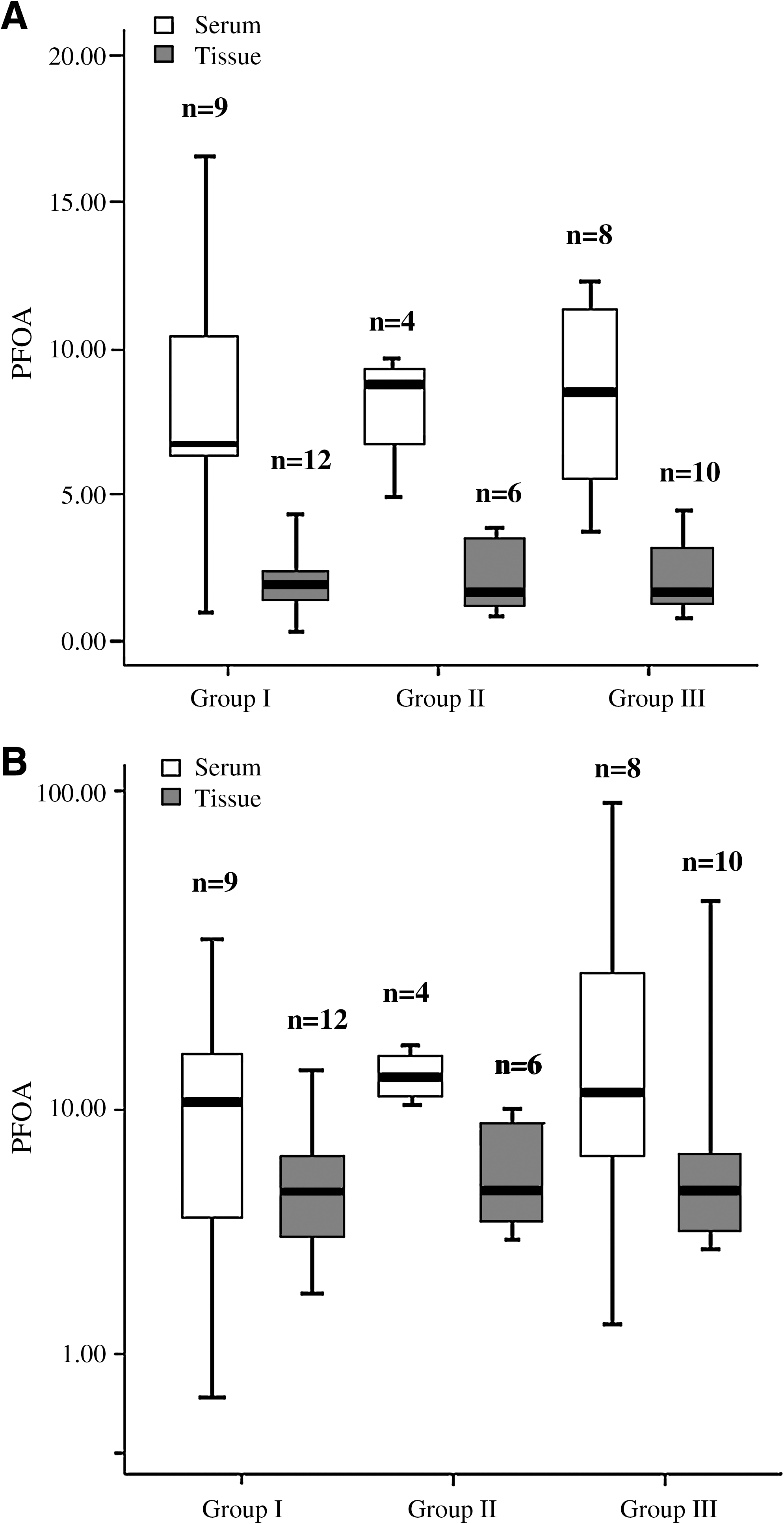
The concentrations of PFOA and PFOS were also evaluated in relation to the type of thyroid disease. To this purpose, patients were divided into three groups: group I (patients with toxic and nontoxic multinodular goiter), group II (patients with differentiated thyroid cancer), and group III (patients with serological and histological evidence of thyroid autoimmune disease, either Hashimoto thyroiditis [HT] or Graves' disease [GD]). The median (range) concentrations of PFOA and PFOS observed in thyroids from patients with different types of thyroid disease are reported in Table 1.
No significant difference was found within different groups of patients and between patients and controls. Group I, patients with toxic and nontoxic multinodular goiter; group II, patients with differentiated thyroid cancer; group III, patients with serological and histological evidence of thyroid autoimmune disease, either Hashimoto's thyroiditis or Graves' disease. Results are reported as median (range) and 25th and 75th percentiles.
PFOA, perfluorooctanoic acid; PFOS, perfluorooctane sulfonate.
The patients undergoing thyroidectomy for different thyroid conditions had similar intrathyroidal levels of both PFOA and PFOS, regardless of the benign/malignant or autoimmune/nonautoimmune nature of their thyroid disease. A linear regression model was constructed by entering the intrathyroidal levels of both compounds, as dependent variable, with age, sex, rural or urban living, working activity, malignant/nonmalignant disease, TPO-Ab, TG-Ab, or TSH receptor antibody positivity, FT3, FT4, and TSH concentrations, thyroid volume, and hypoechogenity at US were entered together as covariates. None of these parameters was significantly related to the intrathyroidal or serum levels of either PFOA or PFOS. Interestingly, the highest level of PFOS (44.7 ng/g), nearly 10 times above the median levels, was in a female patient who had thyroidectomy for a multinodular goiter associated with Hashimoto's thyroiditis. High concentrations of PFOS were also found in her serum (92.9 ng/mL). There were no apparent demographic or other features which distinguished this patient from the other patients.
PFOA and PFOS were also detected in patients' sera, and their median concentrations were 8.6 ng/mL (range = 1.2–16.6 ng/mL) and 11.4 ng/mL (range = 0.5–92.9 ng/mL), respectively. These concentrations were higher than those detected in the corresponding thyroid samples. Similar median concentrations of PFOA and PFOS were found in control sera: 7.45 ng/mL (range = 4–13.7 ng/mL) and 9.3 ng/mL (range = 2.9–23.5 ng/mL) for PFOA and PFOS, respectively. The median (range) concentrations of PFOA and PFOS observed in sera from patients with different types of thyroid disease are reported in Table 1. Interestingly, there was a significant correlation between the serum and the tissue concentrations of PFOS (p < 0.0001) but not between the serum and the tissue levels of PFOA.
Discussion
This study demonstrates for the first time the presence of perfluorinated alkylated compounds, namely PFOA and PFOS, in the thyroid gland of patients submitted to thyroidectomy for different thyroid diseases. The main results of this study were that (i) similar intrathyroidal levels of PFOA and PFOS were detected in patients with thyroid diseases when compared with normal thyroid glands obtained at autopsy, (ii) no relationship was found between the intrathyroidal concentrations of either PFOA or PFOS and the underlying thyroid disease, (iii) the serum concentrations of PFOA and PFOS were significantly higher than those in corresponding thyroid surgical specimens, and (iv) a significant correlation between the serum and the tissue level of PFOS was found in all patients. As PFOA and PFOS are ubiquitous pollutants in the environment, it is not surprising that thyroids from controls for whom no exposure data were available also contained these compounds. The observation that the concentrations of PFOA and PFOS were higher in the serum than in the correspondent thyroid tissue (Fig. 1A, B) does not support the view that PFOA and PFOS are actively concentrated in the thyroid.
Concentrations of PFOA (
Biomonitoring of the human populations in different countries indicates that the serum levels of PFOA and PFOS are strictly influenced by environmental and dietary habits of the population. High serum concentrations of PFOA and PFOS were frequently reported in the United States, Japan, Poland, Sweden, and Denmark. Lower levels were found in India, Columbia, Spain, and Italy. The PFOA to PFOS ratio also varies widely in different countries, being 1:8 in Sweden, 1:5 in the United States, 1:2 in Germany, and 1:1 in Columbia. In this study, the serum ratio of PFOA to PFOS was 1:1.6 (1,20,32).
Toxicological studies in experimental animals aimed at establishing the thyroidal repercussions of PFOS exposure demonstrated that after acute exposure to this compound the concentration of circulating total thyroid hormones decreases, with no compensatory rise in serum TSH (25). This effect is likely due to the ability of PFOS to compete with thyroxine for its binding to plasma proteins (25,26). As a consequence, the serum concentration of FT4 remains unchanged. PFOA and PFOS are also known to be agonists of the peroxisome proliferator-activated receptor (PPAR)-α receptor, and through this pathway they have been shown to have a thyromimetic effect in rat liver. This is believed to result from the transcriptional activation of thyroid hormone-dependent genes (25).
In experimental animal models, PFOS was found to be hepatotoxic and carcinogenic, inducing tumors of the liver. A significantly increased incidence of thyroid follicular cell adenomas was also observed in rats exposed to the highest concentration of this compound (10 –15). However, the Scientific Panel on Contaminants in the Food Chain concluded that the evidence for the induction of thyroid carcinogenic effect was limited. Two carcinogenicity studies of dietary PFOA have shown that this compound may induce hepatocellular adenomas, Leydig cell adenomas, and pancreatic acinar cell hyperplasia in male rats.
The role of PFOA and PFOS in human cancer was investigated in a limited number of studies, mainly in workers occupationally exposed to these compounds. These investigations did not produce convincing evidence for an increased cancer risk. Workers exposed to PFOS-containing materials had a 13 times increased risk for fatal bladder cancer (16), but in a further study this association was found to be not statistically significant (17,18).
In this study, PFOA and PFOS were detectable in all surgical specimens of thyroid tissue. No correlation was found between the intrathyroidal concentrations of these perfluorinated alkylated compounds and any demographic clinical or biochemical feature of the investigated patients. The fact that these compounds were detected at similar levels in both benign and malignant, and autoimmune and nonautoimmune thyroid diseases, together with the lack of any correlation between PFOA and PFOS and the circulating levels of thyroid hormones, TSH, and thyroid autoantibodies, should be taken with caution in view of the limited number of patients enrolled in this study. Indeed, as for several other chemical compounds, later reported to act as endocrine disruptors, the demonstration of the intrathyroidal presence of PFOA and PFOS constitutes the first step for planning future studies aimed at evaluating their potential thyroid-disrupting effects. Experiences drawn from studies on endocrine disruptor agents indicate that in vitro studies are generally more likely to unveil subtle interferences with thyroid cells, in terms of proliferation, iodine uptake, and hormone synthesis. In this view, it seems particularly relevant to remember that this study design does not provide any information as to the time of exposure to PFOA and PFOS, a limit which could be hard to overcome by any in vivo experience.
Footnotes
Acknowledgment
This study was supported in part by funds from the Progetto di Ricerca Finalizzata ex art.12, del D.Lgs.502/92–2007.
Disclosure Statement
The authors have no conflicts of interest that could be perceived as prejudicing the impartiality of the research reported. In particular, this study did not receive any support from the industry that makes or markets the studied compounds.