
Abstract
Background:
Thyroid tuberculosis is rarely encountered. Due to the absence of specific signs and symptoms, the diagnosis is difficult without histopathologic examination of surgical material. In this study, we aim to present histopathologic findings of our patients with thyroid tuberculosis.
Methods:
We retrospectively reviewed 800 thyroidectomy specimens from the pathology laboratories of two medical centers that were obtained over a 5-year period. We reviewed clinical and laboratory data, fine-needle aspiration cytology smears, and 4-μm formalin-fixed paraffin-embedded hematoxylin–eosin sections and Erlich Ziehl Nelsen–stained sections of granulomatous thyroiditis.
Results:
We found nine cases of granulomatous thyroiditis and detected five cases of thyroid tuberculosis. Thyroid ultrasound revealed hypoechoic nodules ranging between 1.3 and 2.5 cm in all patients with thyroid tuberculosis. Fine-needle aspiration cytology smears, which showed thyrocytes, macrophages, and lymphocytes with a colloid background, were nonspecific. Microscopic examination of all thyroids revealed granulomas of different sizes, which were composed of Langhans' giant cells, epithelioid histiocytes, and lymphocytes around caseation necrosis. In Erlich Ziehl Nelsen–stained sections of three cases, bacilli were seen. Bacilli were identified in the microbiology culture of the remaining two patients.
Conclusions:
Thyroid tuberculosis is diagnosed by histopathologic examinations and microbiologic cultures. When granulomatous thyroiditis is encountered, tuberculosis should be kept in mind and Erlich Ziehl Nelsen staining should be performed for prompt diagnosis.
Introduction
Materials and Methods
We retrospectively reviewed reports of 800 thyroidectomy specimens in the pathology laboratories of Dicle University Teaching Hospital and Diyarbakir State Hospital. Thyroidectomy specimens were obtained during a 5-year period from January 2004 to December 2008. We detected nine cases of granulomatous thyroiditis. Epidemiologic, clinical, and laboratory findings of the patients were retrospectively reviewed from hospital records. Five women (age range, 29‱64 years) had a diagnosis of thyroid TB. All patients had thyroid ultrasonography (US) as initial evaluation, and two patients had thyroid scintigraphy. We reviewed US and thyroid scintigraphy reports of the patients. All patients underwent FNAC examination. Material obtained by FNAC was not used for Erlich Ziehl Nelsen (EZN) staining and microbiology culture because thyroid TB was not clinically considered. FNAC smears were retrospectively reevaluated. The reports and 4-μm formalin-fixed paraffin-embedded hematoxylin and eosin–stained sections of thyroidectomy specimens were reviewed. All patients had sections stained with EZN.
Results
Nine out of 800 throidectomy specimens were reported as granulomatous thyroiditis. Microscopic examination of thyroids revealed caseation necrosis in five patients who had a diagnosis of TB with either EZN staining of pathologic specimen or microbiology culture, and this accounted for 0.6% of all thyroid material. Inflammation and foreign body giant cell-containing granulomas without caseation necrosis were present in the specimens of the remaining four patients. Bacilli were absent in EZN-stained sections of these cases, and the patients had the diagnosis of granulomatous (de Quervain) thyroiditis with clinical and laboratory findings.
All five patients with thyroid TB were women (age range, 29‱64), who presented to the outpatient clinics of general surgery and medicine with the common complaint of a mass in the neck. One patient had an occasional yellow drainage from the mass, and another had relapsing fever. Thyroid examination of all patients revealed masses ranging between 1 and 2 cm. Thyroid function tests were within normal limits in all cases. Erythrocyte sedimentation rates were between 32 and 54 mm/h. Leukocytosis was detected in two patients who had drainage and fever. Thyroid US revealed hypoechoic nodules ranging between 1.3 and 2.5 cm in all patients. Two patients had cold nodules on thyroid scintigraphy. Heterogeneous and enlarged thyroids were reported in two patients. All patients had FNAC, which were reported as benign cytological findings. Smears showed thyrocytes, macrophages, and lymphocytes with a colloid background. Although we reviewed the cytological examinations, we did not observe any epithelioid histiocytes or giants cells.
All patients underwent bilateral subtotal thyroidectomies. On gross examination, the thyroidectomy specimens weighed between 65 and 110 g. Their cut surfaces had a colloid-rich appearance with small multiple grey areas; three cases also had necrotic areas. Microscopic examination revealed granulomas of different sizes, which were composed of Langhans' giant cells, epithelioid histiocytes, and lymphocytes around caseation necrosis (Fig. 1). In three cases bacilli were seen in sections stained with EZN (Fig. 2). In the remaining two cases, Mycobacterium tuberculosis was cultured in the microbiology laboratory. None of the patients had cultures from thyroid specimens. A positive bronchial aspirate culture was obtained in one patient, and the other had positive culture from aspiration material of a cervical lymphadenopathy. None of the patients had disseminated TB. In three patients TB of the thyroid gland was primary. Thyroid TB occurred in association with pulmonary TB and TB lymphadenitis in the remaining two patients.

(
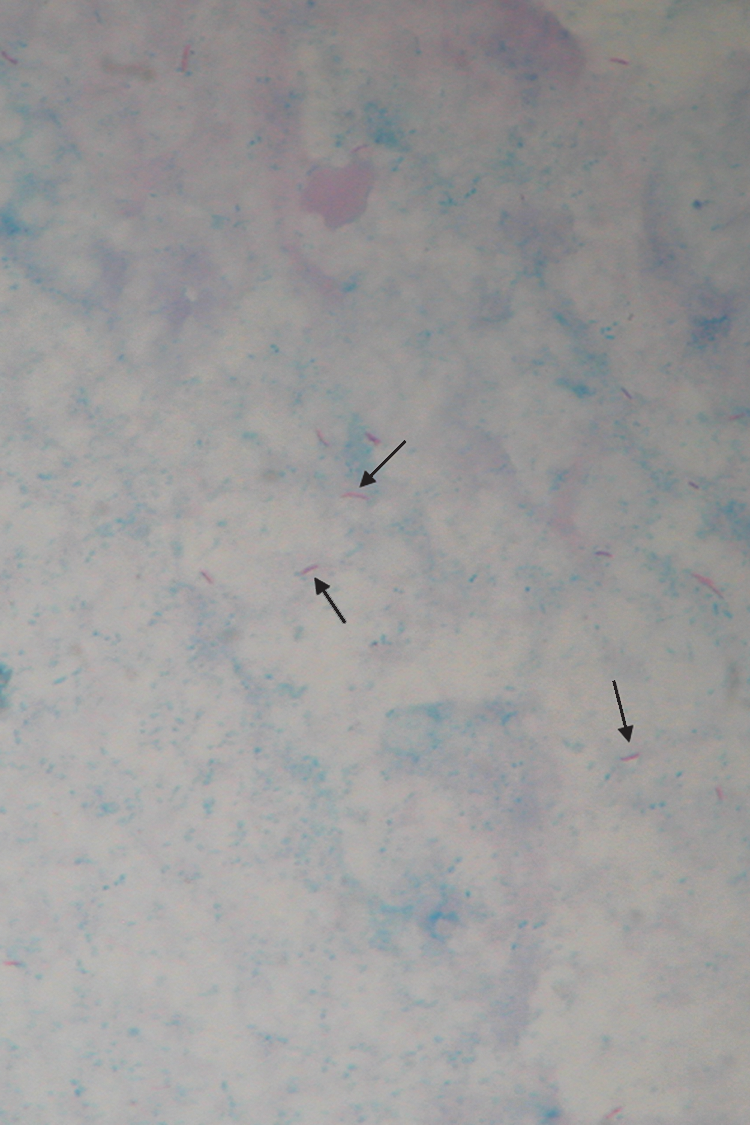
Bacilli are shown with arrows (Erlich Ziehl Nelsen stain, × 1000). Color images available online at
All patients were treated with a combination antituberculosis drug therapy consisting of isoniazid, rifampicin, and ethambutol with the addition of vitamin B6. On a 6-month clinical follow-up the patients were asypmptomatic and euthyroid.
Discussion
TB involves multiple organs. Even in countries with a high prevalence, however, thyroid involvement is rare (5 –7). The incidence of TB is reported to be 43–46 per 100,000 in the general Turkish population, and is higher in eastern and southeastern Anatolia (8). In this study the rate of TB thyroiditis was 0.6%. In the English literature its incidence is reported as 1% on average (9), comparable to our findings. In autopsy studies it is reported in the range of 0.1 to 0.003% (9).
The reason for its rare occurrence in the thyroid is unknown. Bactericidal activity of colloid, the rich blood supply of thyroid, deposition of iodine within the thyroid gland, and antitubercular activity of thyroid hormones (increased phagocyte activity is observed in hyperthyroidism) are possible explanations for the rarity of thyroid TB (2,4).
TB of the thyroid may be primary or spread from other organs (5 –7). The microorganism may invade the thyroid from a neighboring organ or be spread hematogenously (2). Five different clinicopathologic forms of tuberculous thyroiditis have been described. These are multiple lesions seen in miliary pulmonary TB, a goiter (enlarge thyroid) with a common presence of calcification necrosis, a cold abscess, chronic fibrosing TB, and acute abscess formation (2,4,6,7,10 –12). In this study we observed four cases with the goitrous form and a cold abscess with fistula formation.
Manifestations of infection, such as an isolated thyroid nodule, diffuse goiter, or multinodular goiter, can be the initial symptom; however, patients may be totally asymptomatic. There may also be dysphagia or dysphonia owing to local pressure. In the early period there may be hyperthyroidism as a result of parenchymal destruction and ensuing release of thyroid hormones into the circulation. In the late period hypothyroidism may follow because of total destruction of the gland. Thyroid TB may cause fever of unknown origin and lethargy, and it may mimic carcinoma or cysts of thyroid (13).
Since there are no specific signs and symptoms it is difficult to diagnose thyroid TB clinically (2,12). Although there is limited evidence in the literature, FNAC can be a useful method in the diagnosis of thyroid TB. FNAC is a simple, rapid, and easy technique. Obtained material may be used for EZN staining and microbiology culture, and if the findings are suggestive of TB, it can be easily repeated. However, most of the reported cases are diagnosed postoperatively or at postmortem examination (3,10,14).
A slight female dominance is reported in the literature, and the age of patients ranged between 14 and 83 (14). All our cases were female, and their ages ranged between 29 and 64. Laboratory findings are generally normal in tuberculosis thyroiditis. Abnormal thyroid function tests have been reported occasionally (13). US is the main imaging modality in thyroid disease, but the findings of thyroid TB are nonspecific. Thyroid TB can be seen as a well-defined, heterogeneous, hypoechoic mass on US (11). In case of abscess, ill-defined anechoic lesions with internal echoes are observed (15). TB may mimic a cystic nodule (16). Since the imaging findings are nonspecific, the diagnosis is established by histopathologic examination and microbiologic cultures. Microscopical diagnosis is usually made by observing granulomas composed of epithelioid histiocytes and Langhans giant cells with central caseation necrosis, all surrounded with lymphocytes peripherally. Mycobacteria are identified using EZN staining or by culturing the bacilli. In addition, auramine fluorescent staining and advanced techniques such as polymerase chain reaction can be used for identification of TB (17).
In this study, we found that FNAC smears were not diagnostic. Unfortunately, obtained material was not used for microbiology culture and EZN staining. EZN staining was positive in thyroidectomy sections of three cases. Auramine fluorescent staining was not performed.
If no bacilli can be shown by either histochemical or microbiological techniques, thyroid TB must be differentiated from other entities causing granulomatous thyroiditis, such as de Quervain thyroiditis, palpation thyroiditis, sarcoidosis, mycoses, and postoperative necrotizing granulomas. De Quervain thyroiditis is the most important consideration in the differential diagnosis. There are granulomas situated within the thyroid follicles in de Quervain thyroiditis, but there is no caseation necrosis. There may be patchy fibrotic areas (18).
With the increase in patients with immune suppression, there is an increasing incidence of TB all over the world and an increase in extrapulmonary involvement. Since the prognosis is better when thyroid TB is diagnosed and treated early, this must be kept in mind in the differential diagnosis of nodular thyroid lesions in areas with a high prevalence of TB, even in patients with no history and/or symptoms of TB. The diagnosis is confirmed by histopathologic examination and microbiologic cultures. EZN staining is useful in histopathologic diagnosis.
Footnotes
Disclosure Statement
No competing financial interests exist.