
Abstract

Papillary thyroid cancer (PTC) is the most common type of thyroid cancer. It occurs more frequently in women. The age range of presentation is 30–40 years old, but older patients usually have worse outcomes in the literature. It is also the predominant cancer type in children and in patients with a history of irradiation to the head and neck. Papillary microcarcinoma (mPTC) is a subset of PTC defined as measuring less than or equal to 1 cm. The highest incidence in a retrospective surgical series was reported by Pakdaman et al. and was 49.9% out of 860 cases (1). Management strategies for incidental mPTC range from total thyroidectomy and lymph node excision with radioactive iodine ablation to observation alone. Arora et al. stated that mPTC > 7 mm can have aggressive tumor features and disease recurrence similar to conventional PTC. The authors argued that these aggressive tumors should be managed like any other papillary thyroid malignancy (2). We would like to highlight and comment on an exceptional case of fulminant occult mPTC.
A 37-year-old man presented with a 7 × 3.5 cm right painless neck lump in July 2008. The patient had a history of neck trauma two months before. He had no history of familial thyroid disease or malignancy, no history of radiation exposure, and no immune compromise. On physical examination, his neck mass was fixed and his thyroid was normal. Postcontrast CT scans displayed egg-shell calcifications with heterogeneous vascularization within a level II-III-IV nodal mass. The latter showed a mixed echostructure and extracapsular spread (Fig. 1) on US scan. A 2 mm benign-appearing micronodule was noted on the left lower thyroid lobe. Fine-needle aspiration biopsy of the 7 × 3.5 cm lump showed poorly differentiated cells with positive thyroglobulin concentrations (37.6 ng/mL) in the wash out liquid. Serum calcitonin level was normal (<5 pg/mL). Total thyroidectomy with bilateral central and cervical neck dissection was performed, including radical modified neck dissection removing right levels Ib, II, III, IV, Va, the IJV, and the sternocleido-mastoid muscle. The pathology specimen showed a 4-mm well-differentiated thyroid mPTC with focal extracapsular spread of the upper lobe (mPTC R+) and a benign hyperplastic micronodule of the left lower lobe (Fig. 2a). On neck dissection, there was one 7-mm well-differentiated papillary lymphadenopathy (N+) over nine nodes in the central compartments (Fig. 2b). The right lateral compartment dissection showed 5N+/28 lymph nodes, including three with extracapsular spread, one 7 × 3.5 cm node (neck lump) with necrotic ill-differentiated oncocytic features and extensive angiolymphatic invasion, and four with typical well-differentiated papillary carcinoma. Radioiodine therapy was given to the patient because of extensive nodal involvement of his pT1pN1b (R+) Mx mPTC (2010 version of the American Joint Committee on Cancer). The patient had headaches and ear pain during radiotherapy. He was diagnosed with multiple hypervascular metastases of the brain and histology-proven metastases of the external auditory canal and lungs of thyroid origin (Fig. 3). The patient died 28 days later of his brain metastases.
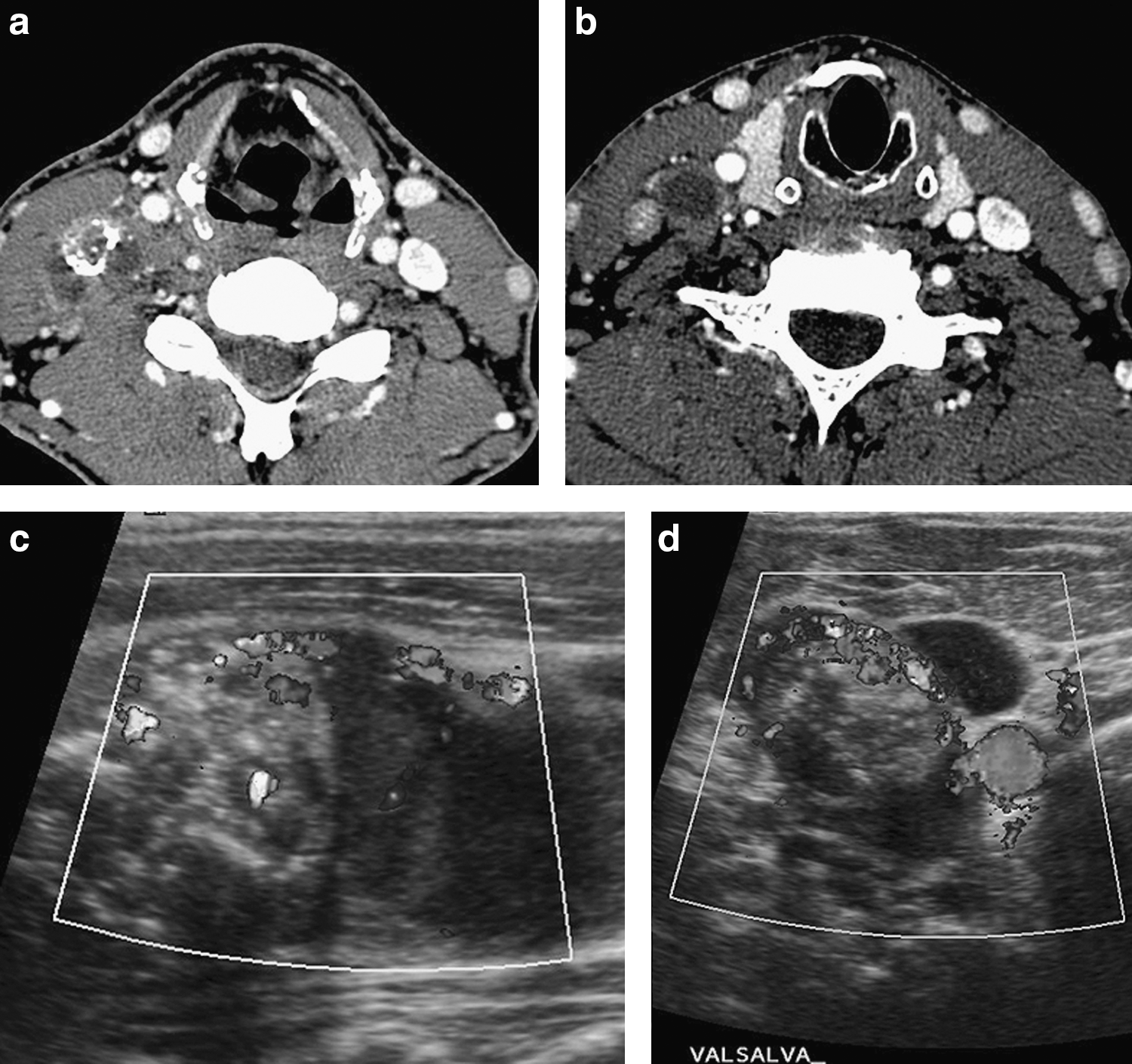
The neck lump CT (
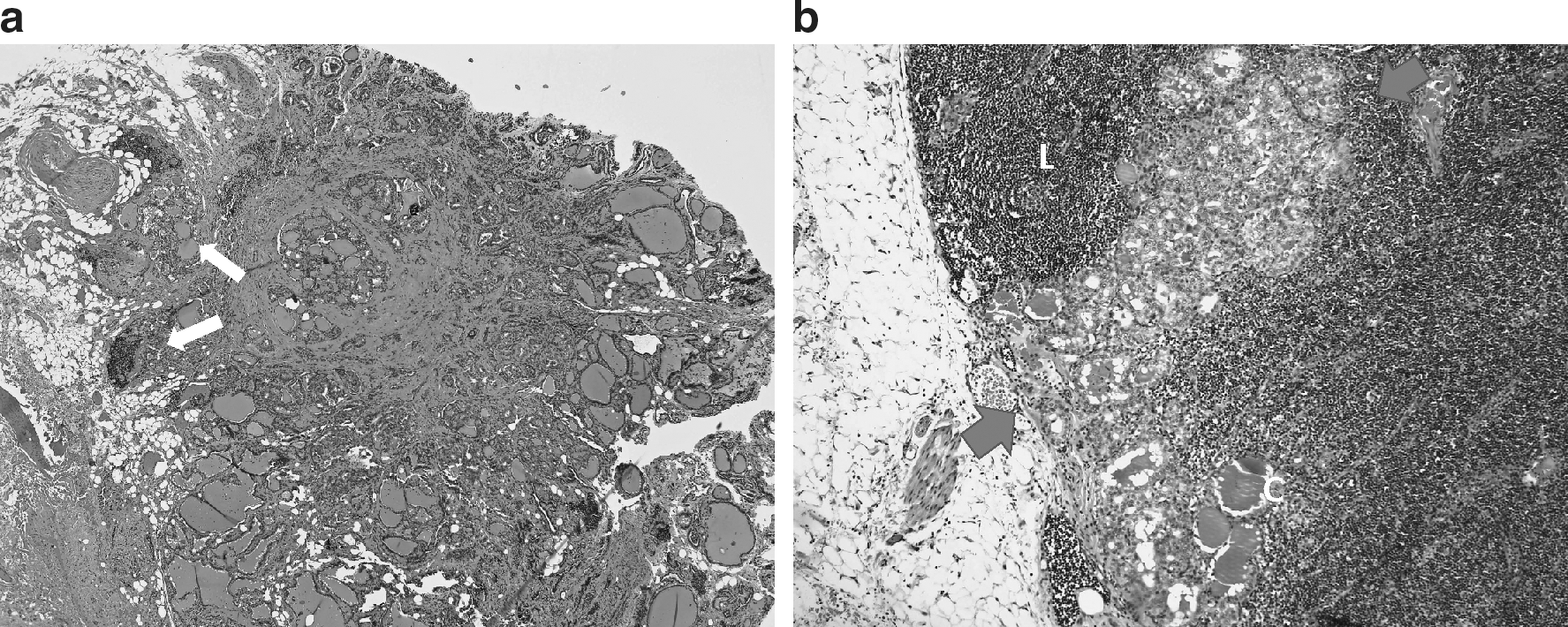
Typical well-differentiated mPTC R+ N+. (
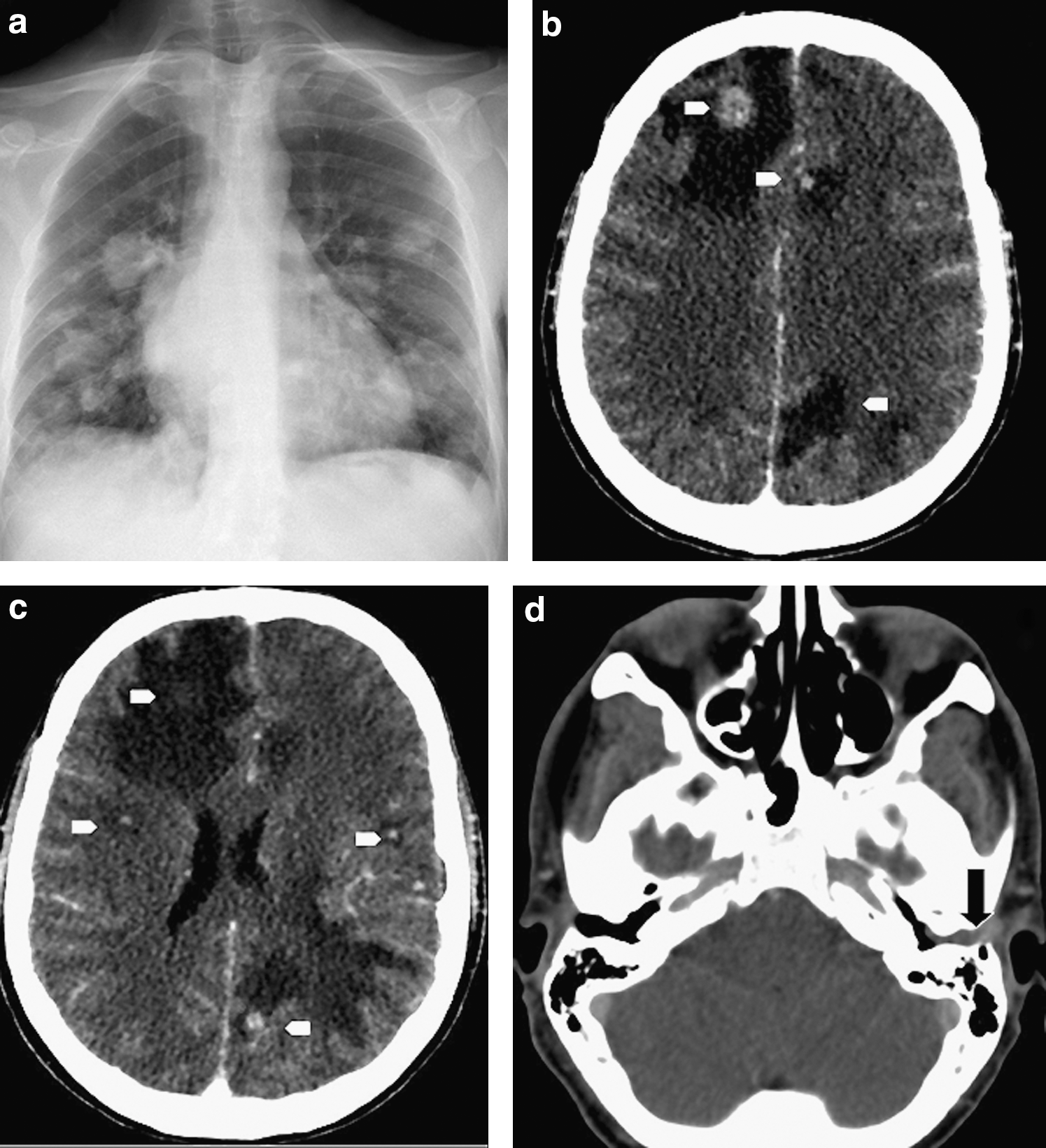
Multiple metastases are shown on chest X-ray (
To our knowledge, this is the first published report of a patient with lethal case fulminant mPTC. This case questions the widely perceived belief that small PTCs are clinically insignificant and do not require active treatment. PTCs have a good prognosis as a group, whereas follicular or anaplastic carcinomas more readily metastasize or infiltrate locally. The subgroup of PTCs with distant metastases, however, has a very poor prognosis. Dinneen et al. identified tumor-related factors associated with improved survival, namely complete resection of the primary tumor, histological grade 1, diploid nuclear DNA, and lung as the first site of distant metastasis (3). In the present case at presentation, the patient had a unique well-differentiated occult 4-mm mPTC with extracapsular spread (Fig. 2a), and two different histological subgroups of ipsilateral metastatic lymphadenopathies (papillary well-differentiated and undifferentiated oncocytic histological types) (Figs. 2b and 4). Despite complete adequate surgical resection (total thyroidectomy with central and lateral compartment dissection and safe margins) followed by radioiodine therapy and external beam radiation therapy, the patient developed brain, undifferentiated biopsy-proven lung, and subcutaneous metastases (external auditory canal) within 2 months. Nevertheless, we cannot definitively rule out the hypothesis of mPTC multifocality. Malignant mPTC may have been composed of a well-differentiated nidus and another poorly differentiated highly invasive nidus with extensive lymphatic spread propensity.

Presence of a mixed malignant population in the neck node mass. (
Lung or bone metastases are usually the first metastatic sites through hematogenous spread (4), whereas brain metastases of thyroid origin are very rare (0.4–1.3%). Well-differentiated carcinomas account for two thirds of brain metastases from thyroid carcinomas, whereas anaplastic and medullary cancers represent 23% and 9%, respectively. Disease-specific survival of metastatic well-differentiated cancers is around 12 months versus less than 5 months in undifferentiated cancers. Surgical resection of brain metastases may be recommended to improve survival but was not performed in our case because of multiple metastases, patient's poor condition, and fulminant disease progression. Interestingly, retrospective pathological reanalysis showed no other primary thyroid tumor than the well-differentiated mPTC R+ (Fig. 2) but the presence of a malignant oncocytic population coexisting with a well-differentiated papillary cellular component of the metastatic neck nodes (Fig. 3). On the 7 × 3.5 cm fixed lateral neck mass, massive angiolymphatic invasion contrasted with the regular histological feature of the primary mPTC at presentation. According to Arora et al., angiolymphatic invasion of the primary tumor can be the only significant indicator of recurrence to distinguish PTC mPTC characteristics and outcome (2). In the present case, contrary to considerations of Arora et al., tumor aggressiveness was not related to size (less than 5 mm) or to angiolymphatic invasion of the primary but to the oncocytic changes of the metastatic tumor in the lateral compartment of the neck, the external auditory canal, the lungs, and in all probability, the brain.
In conclusion, this is the first patient with a lethal fulminant outcome due to an occult 4-mm mPTC. It occurred in a relative young person, a 37-year-old man with unremarkable medical history. This extraordinary aggressiveness may be explained by the oncocytic dedifferentiation of the lateral compartment mass from which other metastases developed into the ipsilateral external auditory canal, the lungs, and the brain. Biological tumor characteristics and weak host resistance are other possible explanations for the unusual aggressiveness of this patient's PTC.