
Abstract
Background:
The preoperative diagnosis of malignancy in nodules suspicious for a follicular neoplasm remains challenging. A number of clinical and cytological parameters have been previously studied; however, none have significantly impacted clinical practice. The aim of this study was to determine predictive characteristics of follicular neoplasms useful for clinical application.
Methods:
Four clinical (age, sex, nodule size, solitary nodule) and 17 cytological variables were retrospectively reviewed for 144 patients with a nodule suspicious for follicular neoplasm, diagnosed preoperatively by fine-needle aspiration (FNA), from a single institution over a 2-year period (January 2006 to December 2007). The FNAs were examined by a single, blinded pathologist and compared with final surgical pathology. Significance of clinical and cytological variables was determined by univariate analysis and backward stepwise logistic regression. Odds ratios (ORs) for malignancy, a receiver operating characteristic curve, and predicted probabilities of combined features were determined.
Results:
There was an 11% incidence of malignancy (16/144). On univariate analysis, nodule size ≥4.0 cm nears significance (p = 0.054) and 9 of 17 cytological features examined were significantly associated with malignancy. Three variables stay in the final model after performing backward stepwise selection in logistic regression: nodule size (OR = 0.25, p = 0.05), presence of a transgressing vessel (OR = 23, p < 0.0001), and nuclear grooves (OR = 4.3, p = 0.03). The predicted probability of malignancy was 88.4% with the presence of all three variables on preoperative FNA. When the two papillary carcinomas were excluded from the analysis, the presence of nuclear grooves was no longer significant, and anisokaryosis (OR = 12.74, p = 0.005) and presence of nucleolus (OR = 0.11, p = 0.04) were significantly associated with malignancy. Excluding the two papillary thyroid carcinomas, a nodule size ≥4 cm, with a transgressing vessel and anisokaryosis and lacking a nucleolus, has a predicted probability of malignancy of 96.5%.
Conclusions:
A combination of larger nodule size, transgressing vessels, and specific nuclear features are predictive of malignancy in patients with follicular neoplasms. These findings enhance our current limited predictive armamentarium and can be used to guide surgical decision making. Further study may result in the inclusion of these variables to the systematic evaluation of follicular neoplasms.
Introduction
Fine-needle aspiration (FNA) remains the gold standard for screening nodules for malignancy (6,7). Despite its accuracy in diagnosing papillary thyroid carcinoma (PTC) and benign, macrofollicular thyroid nodules, FNA is unable to distinguish a follicular carcinoma and follicular variant of PTC from a benign follicular adenoma. Aspirates of each of these entities may reveal a paucity of colloid, hypercellularity, and presence of varying percentage of microfollicles. Currently, the diagnosis of a follicular carcinoma is based on histologic evaluation of the nodule for cellular transcapsular or vascular invasion, which requires surgical excision. Because of the risk of malignancy, most patients are referred for surgical resection, despite the fact that the majority will have a benign follicular adenoma on final pathology. Based on results from a number of studies, ∼10–30% of nodules diagnosed by FNA as suspicious for a follicular neoplasm are malignant (8,9). This results in a significant number of unnecessary thyroidectomies each year, costing healthcare resources and subjecting patients to the risks of surgery and anesthesia. Further complicating matters is the fact that frozen section is unreliable for detecting carcinoma in microfollicular lesions. As such, patients who undergo unilateral thyroid lobectomy are generally subjected to a second surgical procedure if the final pathology reveals malignancy (10 –12).
The ability to better predict the risk of malignancy in a follicular neoplasm would clearly be of benefit with respect to which patients should be referred for surgery, and in those undergoing resection, planning the extent of surgery. Numerous studies have attempted to identify factors predictive of malignancy; however, results have been contradictory. In this study, we aimed to identify clinical and cytological variables that would improve diagnostic accuracy in patients with follicular neoplasms.
Materials and Methods
Patient selection and evaluation
All patients preoperatively diagnosed with a nodule suspicious for a follicular neoplasm by FNA (over a 2-year period at a single institution from January 2006 through December 2007) were assessed retrospectively for four clinical and 17 cytological variables (Table 1). Nodules suspicious for a follicular neoplasm were defined as predominantly nonmacrofollicular on cytology. Hürthle cell lesions were included, and nodules suspicious for PTC were excluded. Demographic information included the patient's age (≤45, 46–55, and ≥56) and sex. The nodule size and presence of other nodules within the thyroid were also noted. Nodule size cutoff was chosen for comparison to American Joint Committee on Cancer (AJCC) tumor node metastasis (TNM) staging (<4.0 cm vs. ≥4 cm) (13). This study was conducted in compliance with the Institutional Review Board of the Massachusetts General Hospital.
Significant variables are shown in bold.
Excluding the two patients with PTC, nodule size >4.0 cm was significantly associated with malignancy.
Transgressing blood vessels are defined as capillaries coursing through groups of cells detectable on intermediate magnification (14).
A single, blinded pathologist at our institution examined each of the FNAs for the presence of 17 cytological/cytoarchitectural variables: cellular crowding, chronic inflammation, transgressing blood vessels, stripped nuclei, nucleoli, colloid, overall cellularity, nuclear to cytoplasmic ratio, Hürthle cells, chromatin, general cytoarchitectural pattern, percentage of macrofollicular cells, percentage of single cells, general nuclear atypia, and specific forms of atypia including nuclear pleomorphism, anisokaryosis, and nuclear grooves. Transgressing blood vessels are defined as capillaries coursing through groups of cells detectable on intermediate magnification (14). FNAs were performed by ultrasound guidance. All cytologic materials, including 6–10 ethanol-fixed, Papanicolaou-stained smears and one thin-layer prep, were reviewed. These findings were compared with final surgical pathology.
Statistical analysis
Significance of clinical and cytological variables was determined by univariate analysis. Chi-square test or Fisher's exact test was used for categorical variables and t-test was used for continuous variables. A p-value of <0.05 was considered significant. A multivariate analysis of backward stepwise logistic regression was used to select the most significant variables with a p-value of 0.1 as the cutoff for staying in the model. Odds ratios (ORs) for malignancy, a receiver operating characteristic (ROC) curve, and predicted probabilities of malignancy for combined features were determined. All variables were included in both the univariate and multivariate analyses.
Results
One hundred forty-four patients met the inclusion criteria during the 2-year period. Overall, there was an 11% (16/144) incidence of malignancy in the index nodule, the majority of which were follicular thyroid carcinomas and none of which were follicular variant of PTC (Table 2). Of note, an additional five patients were found to have incidental papillary thyroid microcarcinomas separate from the index nodule. Women constituted 78% of the entire cohort and 75% of the malignancies. Overall, the mean age was 55 (range, 18–89; standard deviation [SD], ±14.4). Average age in the malignant group was 51 (SD, ±14.3) versus 55 (SD, ±14.4) in the benign group. In patients with malignancy, there was no significant difference in age between men and women (p = 0.35). On univariate analysis, there was no correlation between solitary nodules (p = 0.76), age (p = 0.17), or sex (p = 0.76) with malignancy. Binary groupings for age ≥/<45 (p = 0.36) and ≥/<55 (p = 0.14) were also not correlated with malignancy. There was a 21.4% incidence of malignancy in tumors ≥4 cm versus 8.6% in tumors <4 cm that neared significance (p = 0.09) on univariate analysis. When the two patients with PTC in the index nodule were excluded (n = 142), nodule size ≥4.0 cm was significantly associated with malignancy (p = 0.03).
Of the 17 cytological features examined, nine were significantly associated with malignancy: the presence of transgressing vessels; general nuclear atypia, specifically nuclear grooves, anisokaryosis, and nuclear pleomorphism; cellular crowding; high cellularity; high percentage of single cells; and low percentage of macrofollicles (Table 1; Fig. 1). As expected, there was an inverse relationship between percentage of macrofollicles and malignancy. Seven of the 16 cancers were less than pure microfollicular lesions.
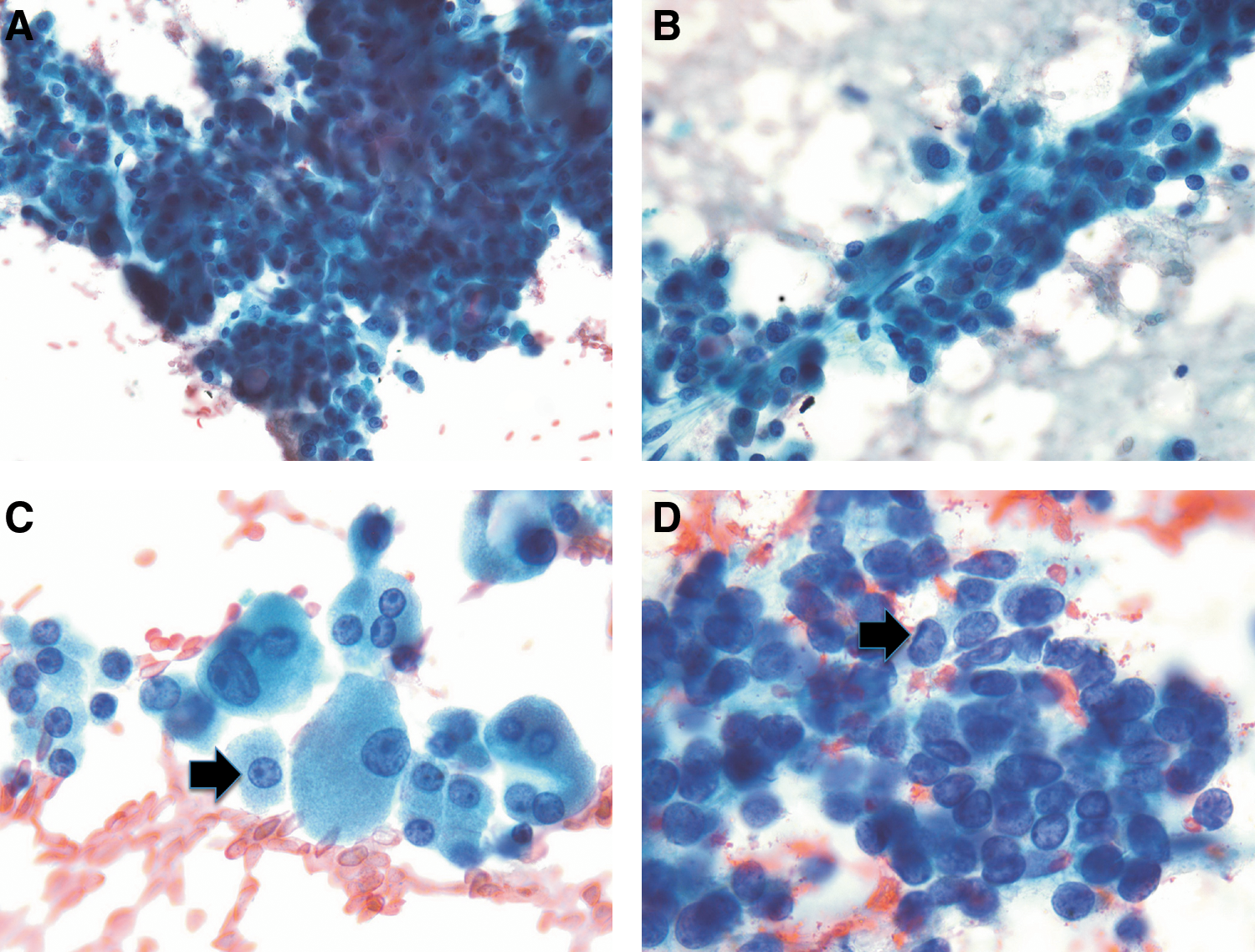
Significant cytological variables: cellular crowding (
Multivariate analysis was performed on two groups of patients: the entire cohort and the group excluding the two papillary cancers. With the entire cohort, three variables stayed in the final model after performing backward stepwise selection in logistic regression: nodule size <4.0 cm, presence of transgressing vessels, and nuclear grooves. Presence of transgressing vessels (OR = 23, p < 0.0001, confidence interval [CI] = 5.90–90.17) and nuclear grooves (OR = 4.3, p = 0.03, CI = 1.18–15.62) were significant, and nodule size neared significance (OR = 0.25, p = 0.05, CI = 0.06–1.03) (Table 3). Moreover, patients with nodule size <4 are less likely and patients with presence of transgressing vessels and/or nuclear grooves are more likely to have a malignant nodule. The presence of all three of these variables has a predicted probability of malignancy of 88.4% in our cohort (Table 4). Transgressing vessels, found in 10 of the 16 cancers, was the most significant variable with sensitivity of 62.5%, specificity of 92.2%, positive predictive value of 50%, and negative predictive value of 53%.
Values significantly correlated with malignancy are shown in bold.
Effect of presence or absence of these variables on predicting malignancy and prevalence of these combined characteristics in the malignant nodules and the entire cohort are reported.
When the two PTC patients were excluded, nuclear grooves were not significant and four variables stayed in the final model: nodule size <4.0 cm (OR = 0.19, p = 0.04, CI = 0.04–0.94), presence of transgressing vessels (OR = 27.5, p = 0.0002, CI = 4.69–161.31), anisokaryosis (OR =12.74, p = 0.005, CI = 2.17–74.77), and presence of nucleolus (OR = 0.11, p = 0.04, CI = 0.01–0.90) (Table 5). Excluding the two PTCs, a nodule sized ≥4 cm, with a transgressing vessel and anisokaryosis and lacking a nucleolus, has a predicted probability of malignancy of 96.5%.
Values significantly correlated with malignancy are shown in bold.
ROC curves provide a comprehensive illustration of the accuracy of variables in predicting a certain outcome, in this instance, in predicting malignancy. The best possible prediction method would yield a point in the upper left corner of the ROC space, representing 100% sensitivity and specificity, whereas a random guess would give a point along a diagonal line from the left bottom to the top right corners. The area under the curve (AUC) represents the predicted probability of malignancy. In this case, the AUC is 0.882, meaning nodules >4 cm with FNA cytology showing transgressing vessels and nuclear grooves have an 88% chance of being malignant (Supplemental Fig. S1, available online at
Discussion
Given the 10–30% incidence of malignancy in follicular neoplasms, current treatment paradigms recommend surgical excision (8,9). The criterion for determination of lesions suspicious for follicular neoplasm varies with institution. At our institution, we assign this distinction to nodules with >50% microfollicles. As illustrated above, there was a direct relationship between percentage of microfollicles and malignancy. Our rate of malignancy (11%) likely reflects the inclusion of less than pure microfollicular lesions. Historically, only nodules with pure microfollicles are recommended for surgery. Our data indicate that malignancies exist with >50% microfollicular cells. To our knowledge this has not been reported previously and may change the indication criteria for surgery.
The decision for performing a hemithyroidectomy versus a total thyroidectomy is based on several factors: the presence of contralateral nodules, specific nodule and patient characteristics, and surgeon and patient preference (15). The American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons Clinical Practice Guidelines of 2001 recommend lobectomy for follicular lesions with completion thyroidectomy considered for invasive follicular thyroid cancers. The 2009 American Thyroid Association guidelines further recommend lobectomy for solid lesions suspicious for follicular or Hürthle cell neoplasms without concordant risk factors and total thyroidectomy for tumors >4 cm or with signs of atypia (16). Presence of specific cytological variables, namely transgressing vessels, may steer a surgeon to perform a total thyroidectomy at the initial surgery avoiding the risks of a second operation.
Many endocrinologists and endocrine surgeons operate under the assumption that larger follicular and Hürthle cell neoplasms are more likely to be malignant. Clinical prognostic parameters of follicular neoplasms have been evaluated with contradictory results. Tyler et al. found that in 81 patients who underwent surgery for indeterminate FNAs, age >50 was the only factor predictive of malignancy (17). Schlinkert et al. found an incidence of malignancy of 12% in their cohort of 219 patients, 9% when PTCs were excluded. Multivariate analysis of this group revealed that nodules >4 cm and fixed nodules were predictive of follicular carcinoma (18). In a cohort of Hürthle cell neoplasms, Bronner et al. found that 80% of Hürthle cell tumors >4 cm were malignant (19). In another series of 122 follicular neoplasms, designated by “monotonous cell population” of >70% by FNA, Baloch and associates noted a 30% incidence of malignancy, 2/3 of which were follicular variant of PTC and 1/3 follicular thyroid carcinoma (FTC)/Hürthle cell carcinoma (HCC). Nodule size >3 cm, age >40, and male sex were all significantly associated with malignancy (20). When excluding suspicious for papillary and including Hürthle cell neoplasm, as in our study, Tuttle et al. found size >4 cm and solitary nodules to be significantly associated with malignancy on multivariate analysis. Of the 22 patients with malignancy in this study, 15 had PTC and only 7 had FTC (21). In the report by Raber et al., solitary nodule was associated with malignancy; however, neither atypia nor clinical parameters including age and sex were associated with malignancy (22). In summary, the data on clinical predictors of malignancy are somewhat confusing and inconsistent. However, our data, and that of others, support a correlation of larger nodule size with carcinoma on final pathology.
Cytological variables have been investigated to distinguish HCC from adenoma. Renshaw et al. found cytoarchitectural patterns including cellular crowding and dyshesion, analogous to single-cell populations, as well as scant colloid and cellular dyplasia, which help in distinguishing HCC from adenoma (23). The correlation of nuclear atypia with malignancy in a group of 98 indeterminate nodules was assessed by Kelman et al., who found that lesions with nuclear atypia had a 44% incidence of malignancy versus 6% of those without atypia (24). Carpi's group similarly found a risk of 21% versus 7% for follicular neoplasms with atypia. Our study also found atypia to be significant. Others have failed to find prognostic cytologic features (25,26).
In this report we identified nine statistically significant cytological variables by univariate analysis: the presence of transgressing vessels, cellular crowding, high cellularity, high percentage of single cells, low percentage of macrofollicles, general nuclear atypia, and specifically, nuclear grooves, anisokaryosis, and nuclear pleomorphism. After performing backward stepwise selection in logistic regression, nodule size, presence of transgressing vessels, and nuclear grooves stayed in the final model. The predictive probability of nuclear grooves in this cohort may reflect the inclusion of the two PTC patients. Of note, although nuclear grooves are extensive in PTCs, they are frequently present in follicular carcinomas as well. In fact, when these two patients are excluded in the analysis, nuclear anisokaryosis replaces nuclear grooves as a significant cytological variable. The presence of transgressing blood vessels maintains an OR for malignancy of >23, with and without the inclusion of the PTC patients. This has previously been found to be a significant cytological variable in distinguishing HCC from adenoma (14).
The designation of follicular neoplasms remains a challenge. Aside from nodule size, clinical features were not found to be helpful in our study. These data are supported by the inconsistent significance of clinical parameters in the literature. Beyond generalized atypia, specific cytological predictive variables have not been studied. In this article, we add specific cytological variables, namely the presence of transgressing vessels on cytology, to the cadre of available diagnostic tools. These data, in addition to ultrasound characteristics and potential molecular markers of malignancy, will provide a more complete armamentarium in distinguishing benign from malignant neoplasms.
Footnotes
Acknowledgment
This study was supported by the Claflin Award of the Massachusetts General Hospital.
Disclosure Statement
There are no conflicts of interests between this report and any of the authors.