
Abstract
Background:
Hypothyroidism decreases energy expenditure and combustion of fuels, but the reported effects on lipid metabolism and insulin sensitivity are divergent and there is a lack of studies assessing rates of lipolysis and lipid oxidation. The present study was conducted to test the hypotheses that hypothyroidism decreases lipolysis, blood concentrations of free fatty acid, lipid oxidation, and insulin sensitivity.
Methods:
We studied 11 hypothyroid patients (thyroid-stimulating hormone: 150 mU/L) with autoimmune thyroiditis (i) before and (ii) after 2 months of triiodothyronine-euthyroidism upon levothyroxine treatment and (iii) compared the patients to 10 healthy volunteers. Subjects underwent a 3-hour study in the basal state followed by a 3-hour euglycemic clamp study, and we used a combination of lipid blood concentrations, palmitate tracer dilution, and indirect calorimetry to assess lipid metabolism.
Results:
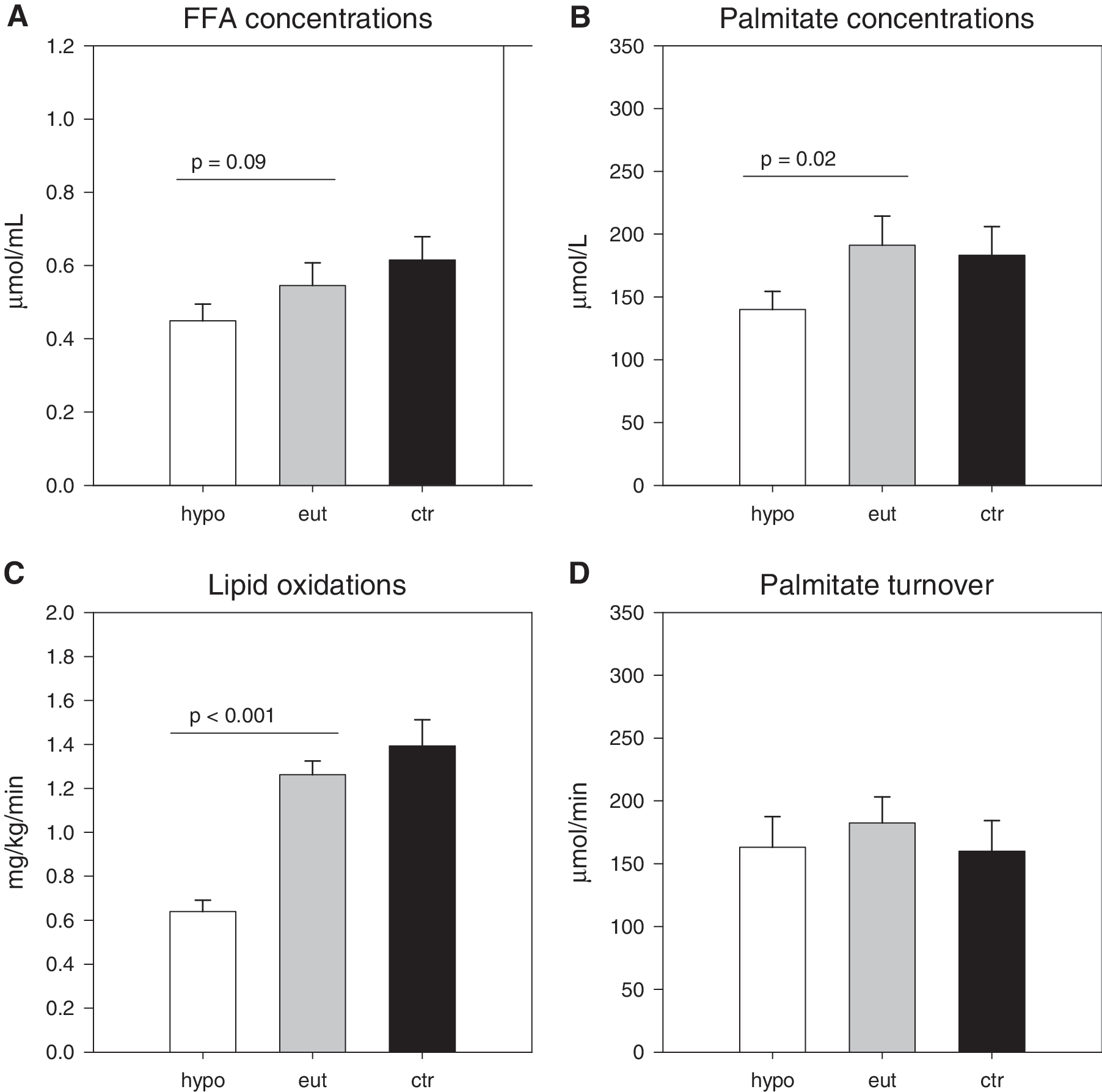
Compared to euthyroid control subjects and/or euthyroid posttreatment values hypothyroid patients were characterized by (i) 40%–50% decreased concentrations of plasma free fatty acids, palmitate, and 3-OH-butyrate (p < 0.05); (ii) >50% decreased lipid oxidation by indirect calorimetry (p < 0.001); (iii) unchanged whole-body lipolysis by palmitate dilution (all p's > 0.45); (iv) 50% increased triglyceride levels (p < 0.05); and (v) ∼30% decreased insulin sensitivity judged by glucose infusion rate values (p = 0.05).
Conclusions:
Our data show that hypothyroidism leads to decreased concentrations and oxidation rates of lipid intermediates and increased triglyceride concentrations in the presence of unaltered rates of lipolysis. The combination of normal lipolysis, low lipid oxidation rates, and high triglyceride concentrations is compatible with increased triglyceride synthesis.
Introduction
The metabolic effects of hypothyroidism are not well characterized. The condition is characterized by increased fasting plasma levels of both cholesterol and triglyceride (6 –8) conferring an elevated risk of atherosclerosis and ischemic heart disease (9,10). Studies on triglyceride kinetics in hypothyroidism have indicated a lowered fractional clearance of triglycerides, and these findings have been supported by studies showing decreased activity of hepatic lipase in severe hypothyroidism by 85% (8). Studies on fatty acid metabolism in hypothyroid patients are sparse. In the early 1970s Tulloch et al. (11) reported decreased palmitate turnover in hypothyroidism, whereas a classic study by Saunders et al. (12) compared hypothyroid patients before and after treatment and found unaltered free fatty acid (FFA), ketone body, and glycerol concentrations together with unchanged lipolysis and lipid oxidation rates, assessed by nonsteady state palmitate dilution (12). This was supported by a study reporting that hypothyroidism does not impact on lipid metabolism as judged by normal basal lipolysis in gluteal fat cells from hypothyroid patients (13). By contrast, more recent studies exploiting the microdialysis technique have indicated decreased lipolysis in subcutaneous abdominal adipose tissue in hypothyroidism (4,14). Others, however, failed to reproduce these findings (15). Reports on lipid oxidation assessed by indirect calorimetry and on steady state FFA turnover rates are lacking.
As regard insulin sensitivity some studies have reported normal responses to insulin (16), but the majority of data support that hypothyroid subjects are resistant to insulin (17,18).
Given these inconsistencies we designed a study comparing hypothyroid patients before and after treatment to healthy euthyroid subjects to test the hypotheses that—as opposed to hyperthyroidism—hypothyroidism is characterized by decreased lipolysis, decreased levels of FFA, decreased lipid oxidation, and decreased insulin sensitivity. For this purpose we used a combination of measurements of blood concentrations, palmitate tracer dilution, indirect calorimetry, and hyperinsulinemic euglycemic clamp techniques.
Materials and Methods
Eleven hypothyroid patients (seven women) were consecutively recruited from our outpatient clinic; the inclusion criterion was untreated hypothyroidism with serum thyroid-stimulating hormone (TSH) values above 20 mU/L. The etiology in all cases was chronic autoimmune thyroiditis, with increased thyroid peroxidase antibody levels. Ten healthy volunteers served as the control group, matched for sex, age, and body mass index of the patients in the euthyroid state. Ghrelin levels in these subjects have previously been published (19).
All participants gave their written informed consent after receiving oral and written information. The study was performed in accordance with the Declaration of Helsinki, and the Aarhus County Scientific Ethics Committee approved the protocol.
Study design
The patients were studied before (pre) and after (post) levothyroxine (L-thyroxine) replacement, when thyroid hormones had been normalized for at least 2 months, that is, triiodothyronine between 1.1 and 2.5 nmol/L and thyroxine levels ranging from 60 to 140 nmol/L. The healthy subjects (ctr) were studied once. Each study day started at 08:00 hours after a 12-hour overnight fast. Indirect calorimetry, palmitate tracer dilution and blood sampling for 3 hours in the basal state were performed on all subjects; only eight patients and seven volunteers underwent an additional 3-hour hyperinsulinemic euglycemic clamp (20). Hyperinsulinemia was achieved by a continuous intravenous infusion of regular human insulin (Novo Nordisk). We aimed to obtain the same levels of insulin during the glucose clamp in both hypothyroid and euthyroid subjects. We have previously observed decreased insulin clearance in hypothyroidism, and accordingly insulin was infused at a rate of 0.6 mU/(kg · min) in the hypothyroid patients, and 0.7 mU/(kg · min) in the patients in the euthyroid state and in the healthy controls. Euglycemia (∼5 mmol/L) was maintained by a variable intravenous infusion of 20% glucose (SAD). Every 10 minute, plasma glucose was sampled and immediately measured in duplicate on a glucose analyzer (Beckman Instruments). Insulin sensitivity was calculated as glucose infusion rate (GIR or M value) during the second hour of the clamp.
Palmitate tracer
[9,10-3H]-palmitate (Danish Medicines Agency) was infused continuously at 0.3 μCi/min from 180 to 240 minute and from 360 to 420 minute, and blood was drawn for analysis of palmitate concentration and specific activity (SA). Steady state of SA was verified (t = 210–240 minute and 390–420 minute) for each individual. Plasma palmitate concentration and SA were determined by high-performance liquid chromatography using [2H31]-palmitate as internal standard. Systemic palmitate flux (rate of appearance, μmol/min) was calculated using the [9,10-3H]-palmitate infusion rate (dpm/min) divided by the steady state palmitate SA (dpm/μmol) (21,22).
Indirect calorimetry
Indirect calorimetry (Deltatrac; Datex Instrumentarium) was performed to assess resting energy expenditure, the respiratory quotient, and fuel oxidation rates (3).
Blood samples and analyses
Thyroid hormones (total triiodothyronine and thyroxine) and TSH were measured by immunoassays (Bayer ADVIA Centaur; Bayer Healthcare).
Plasma glucose was analyzed in duplicate using the glucose oxidase method (Beckman Instruments). Plasma triglyceride concentration was analyzed using a COBAS Fara II. Serum growth hormone was analyzed with a double monoclonal immunoflourometric assay (Delfia; Wallac Oy). Serum insulin and C-peptide were measured with an immunoassay (Dako). Plasma glucagon was measured in one run by an in-house radioimmuno assay modified from (23). Serum leptin was measured in one run by a commercial ELISA kit (Linco Research). Serum FFA levels were determined using a commercial kit (Wako Chemicals).
Glycerol, lactate, alanine, and 3-hydroxybutyrate (3-OHB) were measured using a COBAS biocentrifugal analyzer with fluorometric attachment (Roche Diagnostics) (24).
Statistical methods
All data were tested for normal distribution by P-P-plots, Q-Q-plots, histograms, and the Kolmogorov–Smirnov test using SPSS for Windows version 10.0 (SPSS). Depending on this, Student's paired t-test, Student's unpaired t-test, Wilcoxon signed ranks test for related samples, or Mann–Whitney U-test for unrelated samples were employed for comparisons. Results are expressed as mean ± standard error of the mean. p-Values under 5% were considered statistically significant.
Results
Anthropometric indices
The patients and healthy controls were comparable regarding age, sex, and body mass index (Table 1). Hypothyroid subjects had slightly decreased fat mass and, compared to euthyroidism, had increased lean body mass.
Values are means ± SE.
ns, nonsignificant; BMI, body mass index; DEXA, dual energy X-ray absortiometry; LBM, lean body mass; T3, triiodothyronine; T4, thyroxine; TSH, thyroid-stimulating hormone; TPO, thyroidperoxidase; RQ, respiratory quotient; EE, energy expenditure; SE, standard error of the mean.
Circulating hormones
Biochemically the patients were clearly hypothyroid at study entry: pretreatment thyroxine levels were 86% lower than posttreatment (nmol/L) (14.9 ± 3.7 [pre] vs. 108.1 ± 4.4 [post], p < 0.001), and 83% lower as compared to the healthy subjects (p < 0.001). Replacement with L-thyroxine resulted in a normalization of thyroid hormones (Table 1).
During the basal period there was no significant difference between insulin levels in the three groups (pre, post, and ctr), nor were there significant differences between c-peptide and glucagon between the three groups. Growth hormone and leptin levels were also similar in all groups (Table 2). Insulin-like growth factor-I levels were decreased and catecholamine levels increased in hypothyroidism.
Values are means ± SE.
GIR, glucose infusion rate; GH, growth hormone; IGF-I, insulin-like growth factor-I; stim, stimulated (during hyperinsulinemic euglycemic clamp).
Circulating metabolites
Fasting glucose concentrations were significantly lower in hypothyroid patients compared to after treatment (mmol/L) (5.01 ± 1.16 [pre] vs. 5.34 ± 0.19 [post], p = 0.001). After treatment glucose values were normalized and comparable to healthy controls. Triglyceride levels were significantly increased in patients in the hypothyroid state as compared to the euthyroid state (mmol/L) (1.66 ± 0.21 [pre] vs. 1.24 ± 0.15 [post], p = 0.038).
FFA levels were decreased during hypothyroidism and were significantly lower in the hypothyroid state compared to healthy controls (μmol/L) (449.5 ± 46.3 [pre] vs. 614.8 ± 64.3 [ctr], p = 0.05) (Table 3). 3-OHB concentrations were significantly decreased in the hypothyroid state and normalized during L-thyroxine treatment (μmol/L) (62.7 ± 14.5 [pre] vs. 145.0 ± 36.8 [post], p = 0.04).
Values are means ± SE.
During hyperinsulinemic euglycemic clamp.
TG, triglyceride; FFA, free fatty acids; BOH, beta-hydroxybutyrate.
Indirect calorimetry
Resting energy expenditure was significantly reduced in the hypothyroid state and increased following L-thyroxine replacement to a level comparable to that of the control group (Table 1). The respiratory quotient was elevated in the hypothyroid state and became normalized after L-thyroxine substitution (Table 1). Lipid oxidation was significantly decreased (mg/[kg · min]) (0.64 ± 0.05 [pre] vs. 1.26 ± 0.06 [post], p < 0.001) and normalized with treatment.
Palmitate
Palmitate concentrations were 29% lower in the hypothyroid state compared to the euthyroid state. Levels normalized during L-thyroxine treatment and became comparable to healthy controls. (135.7 ± 16.0 [pre] vs. 191.1 ± 23.3 [post], p = 0.02).
There was no significant change in palmitate flux (163.0 ± 24.4 [pre] vs. 182.5 ± 20.6 [post], p = 0.46) (Fig. 1).
(
As expected there was a positive correlation between palmitate concentration and palmitate flux both in the euthyroid state and in healthy controls (Fig. 2). No such correlation was observed in the hypothyroid state (p = 0.20).

Correlation between palmitate turnover and palmitate concentration in (
Glucose clamp
Insulin sensitivity was significantly decreased in hypothyroid patients compared to after treatment (GIR values in mg/[kg · min]: 4.99 ± 0.64 [pre] vs. 6.61 ± 1.12 [post], p = 0.05). During the glucose clamp we attempted to obtain similar insulin levels in all groups, administering 0.6 mU/(kg · min) insulin to patients in the hypothyroid state and 0.7 mU/(kg · min) insulin to patients in the euthyroid state and to healthy controls. Insulin levels were similar in patients in the hypothyroid state compared to euthyroid, but significantly higher than in healthy controls (pmol/L) (365.5 ± 26.9 [pre] vs. 276.0 ± 24.4 [ctr], p = 0.005) (Table 2).
Discussion
Our results show that hypothyroidism is characterized by complex and unexpected changes in lipid metabolism. Despite normal rates of lipolysis, circulating concentrations of FFA, palmitate, and 3-OHB and lipid oxidation rates are decreased. This suggests that an increased fraction of the circulating FFA pool is diverted elsewhere, for example, to increased triglyceride synthesis, as supported by the elevated triglyceride concentrations in blood. To our knowledge this is the first study to measure lipid oxidation and FFA turnover under steady-state conditions in hypothyroid humans.
Saunders et al. (12) reported normal turnover rates of FFA and normal palmitate oxidation rates estimated after a bolus injection of 14C-labelled palmitate in 12 hypothyroid patients. It should be noted that these patients were not as profoundly hypothyroid as our patients in terms of thyroid hormone concentrations and energy expenditure, which may explain the finding of unaltered FFA, ketone body, and glycerol concentrations in that study. In addition, the isotopic measurements performed involved nonsteady state algorithms. Nonsteady state tracer techniques may lead to systematic errors due to differences in volumes of distributions and equilibration rates between various compartments of the body. Still, the concept of normal basal lipolysis in hypothyroidism is supported by an in vitro study showing normal base line lipolysis in isolated gluteal adipocytes from hypothyroid women, with an impaired response to catecholamines (16).
On the other hand, a study by Caraccio et al. (25) reported increased levels of FFA and ketone bodies in patients with subclinical hypothyroidism, implying that the influence and lack of thyroid hormones on lipid metabolism may be very complex. More recent studies employing microdialysis have yielded conflicting results when using local interstitial glycerol as a surrogate measure of regional lipolysis, reporting both decreased (17,18) and normal lipolytic rates. Atrial natriuretic peptide (ANP) is a powerful lipolytic peptide. It seems that thyroid hormones regulate ANP-induced lipolysis. ANP perfusion in hyper- and hypothyroid patients in a study by Polak et al. (15) induced a significant increase in extracellular glycerol concentration in both groups, determined by microdialysis. ANP-stimulated extracellular glycerol concentration AUC was higher in the hyperthyroid compared with hypothyroid group before the treatment. The induction of lipolysis by ANP perfusion in the hypothyroid group was, however, not modified by treatment, indicating that ANP-induced lipolysis is not diminished in hypothyroid patients.
Data from the literature on circulating concentrations of lipid intermediates, such as FFA, glycerol, and ketone bodies are amazingly sparse, and it should again be emphasized that our finding of decreased concentrations, aside from glycerol concentrations, which where normal, may relate to the fact that our patients were profoundly hypothyroid with TSH levels of around 150 mU/L.
Our finding of normal palmitate turnover rates expressed as μmol/min strongly supports that rates of lipolysis are normal in patients with hypothyroidism. Increased levels of catecholamines have been reported previously (26) and may contribute to maintenance of normal lipolytic rates.
Following treatment there was an increase in total fat mass and a decrease in lean body mass assessed by dual energy X-ray absortiometry, but body composition before treatment was very similar to that of the control subjects. Total fat mass in patients was under all circumstances below that of euthyroid patients and of healthy controls. In this context it is of interest that experimental studies in animals have shown an increased total body water content in hypothyroidism relating to compromised vasopressin secretion and decreased renal aquaporine 2 expression (27). Thus, fat mass and, in more particular, lean body mass in hypothyroid patients may be overestimated due to increased, inert body water mass.
If rates of lipolysis are normal and circulating FFA concentrations and lipid oxidation rates are decreased, how is the remaining FFA disposed of? Increased ketogenesis seems implausible since 3-OHB concentrations were normal and since increased ketogenesis ultimately would translate into increased lipid oxidation. The obvious candidate therefore is triglyceride synthesis. In our study we found that triglyceride levels were elevated around 50% in hypothyroid patients compared to euthyroid patients and healthy control subjects. This perturbation may contribute to the increased clinical risk of cardiovascular disease in hypothyroidism. Previous studies have reported that subclinical hypothyroidism is characterized by elevated triglyceride levels, which become normalized after treatment (28), and one study has shown that hypothyroidism doubled triglyceride synthesis and triglyceride synthesis enzyme activities in rat brown and white adipocytes (29). In addition, it has been shown that hypothyroidism increases intramuscular triglyceride storage of palmitate in rats (30).
In our study we found hypothyroid subjects to be insulin resistant, in accordance with most other reports (14,18). This occurred despite the fact that insulin concentrations tended to be elevated even though we infused less insulin in patients with hypothyroidism. Although the mechanisms remain uncertain, decreased levels of insulin-like growth factor-I have previously been reported in hypothyroidism and this may contribute to insulin resistance (31). It is also possible that increased catecholamine levels and/or sympathetic nerve activity plays a role. During the glucose clamp, rates of lipolysis were suppressed to normal levels, suggesting that lipolysis is not resistant to insulin.
In summary, we have found that hypothyroidism is characterized by some emblematic abnormalities of lipid metabolism, which include reduced blood concentrations of FFA and ketone bodies, reduced lipid oxidation, and increased triglyceride levels in the presence of entirely normal palmitate/FFA turnover. This suggests and merits future studies looking at the possibility that triglyceride synthesis rates are pathologically elevated in this relatively prevalent condition.
Footnotes
Acknowledgments
The excellent technical assistance of Iben Christensen, Hanne Petersen, and Lene Ring is highly appreciated. The study was supported by Novo Nordisk Fonden and by FOOD.
Disclosure Statement
The authors declare that no competing financial interests exist.