
Abstract
Background:
Ultrasound is a useful imaging tool in the assessment of thyroid glands, and Doppler ultrasound helps in the evaluation of thyroid vascularity. This study was undertaken to evaluate the difference in the thyroid vascularity demonstrated on the state-of-the-art high-sensitivity power Doppler sonography (HSPDS) and the conventional power Doppler sonography (PDS), and to investigate the feasibility of using a customized algorithm with image-processing software for semi-quantitative assessment of thyroid vascularity.
Methods:
A total of 25 healthy volunteers were included in the study, and each subject had two thyroid ultrasound examinations with HSPDS and PDS, respectively. High sensitivity and conventional power Doppler sonograms of the thyroid glands were taken and recorded. To evaluate the vascularity of thyroid lobes quantitatively, a customized algorithm using the software Matlab® was developed and used to analyze the ultrasound images. The vascularity of thyroid lobe (i.e., region of interest, ROI) was expressed as the vascular index (VI), which is the ratio of the number of color pixels to the total number of pixels within the ROI.
Results:
Results showed that thyroid vascularity was detected in all thyroid lobes on both HSPDS and PDS. The mean VI of the thyroid lobes on HSPDS (right lobe, 0.31 ± 0.08; left lobe, 0.32 ± 0.07) was significantly higher than on PDS (right lobe, 0.18 ± 0.09; left lobe, 0.16 ± 0.08) (p < 0.05). There was no significant difference in the VI between the right and left thyroid lobes (p >0.05). On HSPDS, 96% of the thyroid lobes showed a VI <0.5, while 96% of thyroid lobes had a VI <0.3 on PDS.
Conclusions:
HSPDS is more sensitive than PDS in the detection of thyroid vascularity. The developed algorithm can quantify the color pixels on power Doppler sonograms, which is useful for objective assessment of thyroid vascularity.
Introduction
Ultrasound is useful in the assessment of thyroid glands. Gray-scale ultrasound can assess the morphology of the thyroid, whereas the vasculature of thyroid gland can be evaluated with Doppler sonography. Previous studies have suggested that the assessment of the vascularity of thyroid gland is useful in the diagnosis of thyroid diseases (1 –5). Thyroid diseases, such as Graves' disease (also known as diffuse toxic goiter), thyrotoxicosis, and acute thyroiditis, cause an increased thyroid vascularity on ultrasound (2 –7). Doppler ultrasound also helps to distinguish autoimmune form of toxic multinodular goiter from nonautoimmune form of the disease in which the former shows markedly increased extranodular parenchymal vascularity, whereas the latter demonstrates normal extranodular parenchymal vascularity (1). Moreover, the assessment of thyroid vascularity is helpful in monitoring treatment responses because patients with thyroid diseases may have decreased thyroid vascularity during and after treatment (4,7). However, the variations of thyroid vascularity may be subtle in some patients, particular for those who are at the early stage of the disease or at the initial stage of the treatment. Therefore, Doppler ultrasound with higher sensitivity in detecting blood flow, which allows detection of smaller vessels, is essential for accurate assessment of thyroid vascularity changes.
With the advancement of technology, high-sensitivity power Doppler sonography (HSPDS) (also known as velopower Doppler sonography, as it also shows information of blood flow direction, similar to color Doppler sonography) is available, which has been suggested to be more sensitive than conventional power Doppler sonography (PDS) in the detection of blood flow (8). Stramare et al. (8) used HSPDS to assess the vascularity of normal superficial lymph nodes, and compared their findings with another study that used PDS in assessing intranodal vascularity. However, as different groups of subjects were used in these two studies, the difference in the sensitivity of detecting blood flow between HSPDS and PDS may not be accurately evaluated. To the best of our knowledge, the literature is devoid of information about the use of HSPDS in assessing thyroid vascularity. Therefore, this study was undertaken to compare the thyroid vascularity of the same group of subjects when using HSPDS and PDS.
In the assessment of thyroid vascularity, a subjective grading system was usually used (1,2,4,6,9). However, this method may not be accurate in the assessment and cannot evaluate subtle variations of thyroid vascularity. An objective and quantitative method is needed for more accurate assessment of thyroid vascularity. In the present study, a semi-quantitative approach was used to evaluate the thyroid vascularity.
Materials and Methods
A total of 42 healthy volunteers with no history of thyroid diseases or thyroid surgery, without family history of thyroid diseases, and without signs and symptoms of thyroid diseases were recruited for the study. This study was approved by the Human Subject Ethics Subcommittee of the Department of Health Technology and Informatics, the Hong Kong Polytechnic University. Written consent was obtained from all subjects before the commencement of the study. Gray-scale ultrasound examination of the thyroid gland was initially performed in each subject to identify any thyroid nodules. Ultrasound scans were performed with a 12–5 MHz linear transducer (Philips HD11 XE, Bothell, WA). All ultrasound examinations were performed using the SonoCT® real-time compound imaging and XRES™ adaptive image-processing functions for higher image resolution (Philips Medical System, Bothell, WA). In the ultrasound examination, subjects laid supine on the examination table with the neck hyperextended, and the shoulders were supported with a pillow. The left and right thyroid lobes were assessed separately with the subject's head turned away from the side under examination. Transverse and longitudinal scans of each thyroid lobe were performed to examine for any thyroid nodules. Since the aim of the present study was to evaluate and compare the thyroid vascularity detected by PDS and HSPDS in the same group of subjects, thyroid function tests were not performed on the subjects. Nevertheless, the medical history of the subjects was taken in detail, and subjects with history of thyroid diseases or thyroid surgery, with family history of thyroid diseases, or with signs and symptoms of thyroid diseases were excluded from the study.
For the subjects without thyroid nodules, the vascularity of the left and right thyroid lobes was assessed with two Doppler sonographic methods: PDS and HSPDS, in the same ultrasound session. For PDS, a Philips HD11 XE ultrasound unit in conjunction with a 12–5 MHz linear transducer was used (Philips Medical System). For HSPDS, an Esaote Technos MPX ultrasound unit with a 13–4 MHz linear transducer was used (Esaote, Genoa, Italy). Settings of both Doppler sonographic methods were standardized for high sensitivity with a medium wall filter to allow detection of vessels with low blood flow and to have minimum color noise. Pulsed repetition frequency was 700–750 Hz, and medium persistence was used. The color gain was initially increased to a level that shows color noise, and then decreased until the noise disappears (10,11). For both PDS and HSPDS, multiple transverse scans of the left and right thyroid lobes were taken and recorded. For each subject, three PDS and three HSPDS images that show the most abundant vascularity of the left thyroid lobe were selected for the evaluation of thyroid vascularity. Similarly, three PDS and three HSPDS images of the right thyroid lobes were selected.
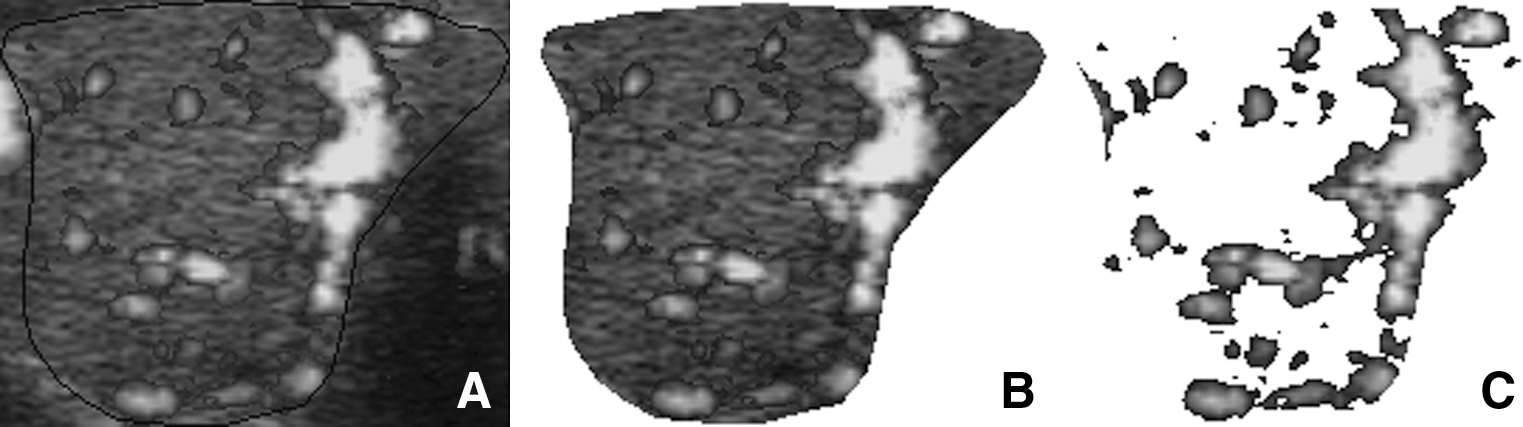
With the use of the software program Matlab® (version 7.3.0.267 R2006b; The MathWorks, Natick, MA), a customized algorithm was developed to evaluate the thyroid vascularity. In the evaluation of the thyroid vascularity, selected ultrasound images were retrieved from the ultrasound units, and converted into tagged image file format. Archived images were then transferred to a computer workstation with the Matlab and the Microsoft Paint (version 5.1; Microsoft Corporation, Redmond, WA) installed. Using the Microsoft Paint software, the boundaries of the thyroid lobe (i.e., ROI) were manually outlined on the ultrasound image (Figs. 1 and 2). Images with the ROI outlined were then analyzed with the Matlab. With the use of the customized algorithm, the ROI was initially extracted from the ultrasound image and the total number of pixels of the ROI was then counted by the algorithm (Figs. 3A, B and 4A, B). Subsequently, the color pixels coded by HSPDS or PDS were extracted from the ROI and the number of color pixels was counted (Figs. 3C and 4C). The vascular index (VI) of the thyroid lobe was calculated by the following equation:
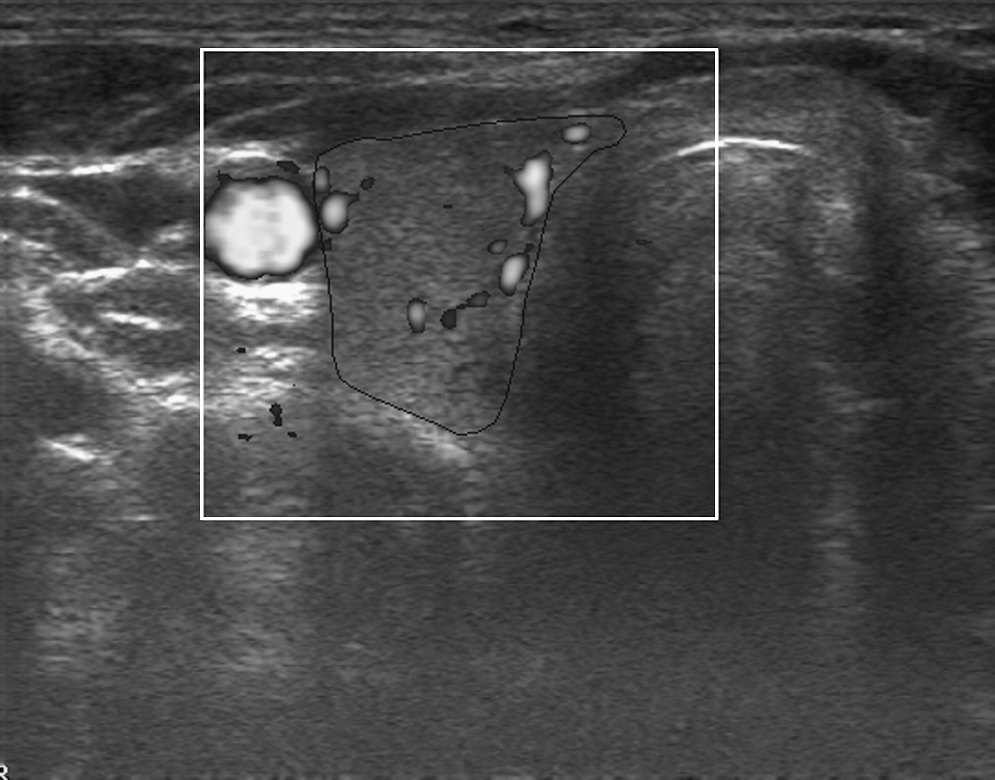
Conventional power Doppler sonogram showing a transverse scan of the right thyroid lobe of a subject. Note the boundaries of the thyroid lobe were outlined (black line).
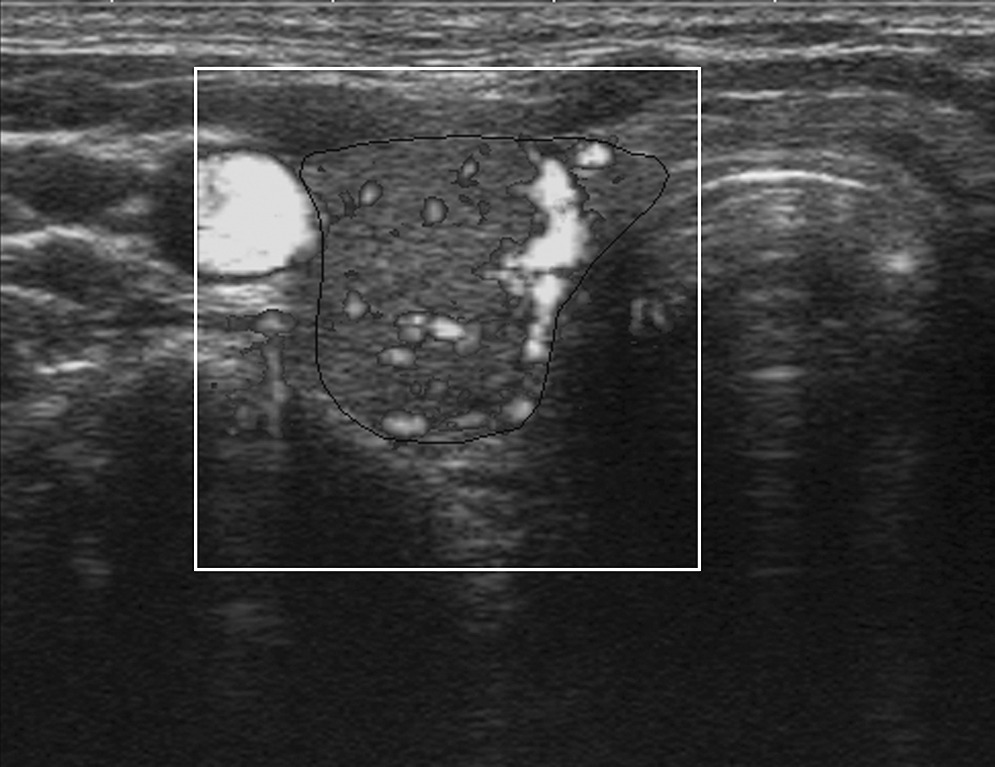
High-sensitivity power Doppler sonography (HSPDS) showing a transverse of the right thyroid lobe of the same subject as in Figure 1. Note the boundaries of the thyroid lobe that were outlined (black line).

The sequence of image analysis of the power Doppler sonogram as in Figure 1 by using the customized algorithm with the Matlab. (
The sequence of image analysis of the high-sensitivity power Doppler sonogram as in Figure 2 by using the customized algorithm with the Matlab. (
VI of the thyroid lobe = Number of color pixels within the ROI/Total number of pixels within the ROI.
For both PDS and HSPDS, a mean VI was calculated for each thyroid lobe by averaging the VI of the three ultrasound images. The mean VI of the thyroid lobes on PDS will be compared with that on HSPDS, and the level of significance of the difference was calculated by paired t-test. The difference in the VI between the left and right thyroid lobes was also evaluated by paired t-test. The level of significance of the difference in the number of thyroid lobes with different VI between PDS and HSPDS was calculated by chi-square test.
Results
Of the 42 subjects recruited, 17 subjects showed at least one nodule in their thyroid and were excluded from the study. Thyroid nodules were not detected in the remaining 25 subjects and these subjects were included in the study. There were 7 men and 18 women (age range, 19–64 years; mean age, 46.8 years). For the 25 subjects included in the study, the vascularity of their thyroid lobes (25 left lobes and 25 right lobes) was evaluated with PDS and HSPDS. Of the 50 thyroid lobes evaluated, a total of 150 conventional power Doppler sonograms and 150 high-sensitivity power Doppler sonograms were selected and analyzed for the VI of the thyroid lobes using the customized algorithm with the Matlab.
Of the 50 thyroid lobes assessed, results showed that thyroid vascularity was detected in all thyroid lobes when using PDS or HSPDS. In all the thyroid lobes, HSPDS (range of VI, 0.19–0.51) demonstrated a higher VI than PDS (range of VI, 0.03–0.38). The mean VI of the thyroid lobes on HSPDS (right lobe, 0.31 ± 0.08; left lobe, 0.32 ± 0.07) was significantly higher than that on PDS (right lobe, 0.18 ± 0.09; left lobe, 0.16 ± 0.08) (p < 0.05, Fig. 5). On both PDS and HSPDS, there was no significant difference in the VI between the right and left thyroid lobes (p > 0.05, Fig. 5). Table 1 shows the number of thyroid lobes with different VI when PDS or HSPDS was used. On HSPDS, 96% of the thyroid lobes showed a VI ≥0.2 but <0.5. However, 96% of thyroid lobes demonstrated a VI <0.3 when PDS was used. The difference in the number of thyroid lobes with different VI on PDS and HSPDS was statistically significant (p < 0.05).
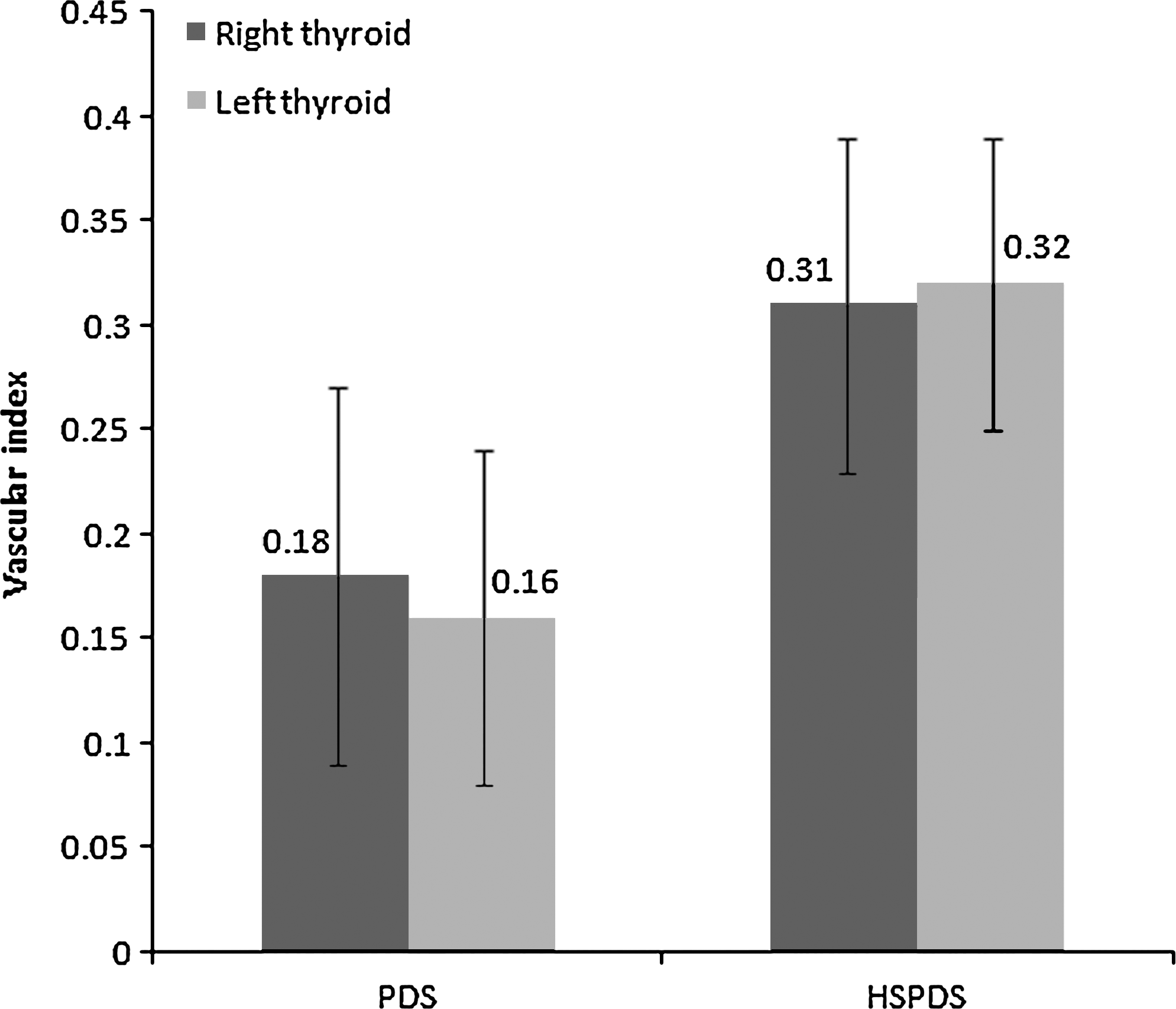
A bar chart showing the mean vascular index of the right and the left thyroid lobes on conventional power Doppler sonography (PDS) and HSPDS. The error bars indicate one standard deviation of the data.
VI, vascular index; PDS, conventional power Doppler sonography; HSPDS, high-sensitivity power Doppler sonography.
Discussion
It has been reported that the evaluation of intrathyroidal vascularity using color or power Doppler sonography is useful in the diagnosis of and monitoring treatment response of thyroid diseases such as Graves' disease, thyrotoxicosis, acute thyroiditis, and toxic multinodular goiter (1 –7,9). While power Doppler sonography is more sensitive than color Doppler sonography in the detection of blood flow, state-of-the-art power Doppler imaging technique is now available and allows an even more sensitive detection of blood flow than PDS. The results of the present study showed that HSPDS was more sensitive than PDS in detecting thyroid vascularity in which the VI of thyroid lobes evaluated with HSPDS was on average about 72% (right lobes) to 100% (left lobes) higher than that evaluated with PDS. Moreover, on HSPDS the majority of thyroid lobes (96%) had a VI of 0.2 to 0.5, whereas most of the thyroid lobes (96%) demonstrated a VI <0.3 on PDS. The results were consistent with those of a previous study (8), which found that HSPDS is more sensitive than PDS in detecting the blood flow of superficial lymph nodes. The higher VI of thyroid lobes in HSPDS was probably due to the higher sensitivity of HSDPS in detecting smaller blood vessels and vessels with lower blood flow within the thyroid gland.
In the present study, all the evaluated thyroid lobes demonstrated vascular signals on both PDS and HSPDS. The results were consistent with the findings of previous reports that normal thyroid glands demonstrate either minimal or absent intrathyroidal vascularity (1,4,7,9). Although HSPDS demonstrated more thyroid vascularity than PDS, none of the normal thyroid lobes showed abnormal hypervascularity on HSPDS.
The present study used a semi-quantitative VI to quantify the thyroid vascularity. A similar method in the assessment of thyroid vascularity has been reported (3). Hiromatsu et al. (3) found that the mean VI of the thyroid glands in healthy volunteers was 0.73%. However, in the present study, the mean VI of the thyroid glands was 0.31–0.32 (i.e., 31–32%) on HSPDS and 0.16–0.18 (i.e., 16–18%) on PDS. The discrepancy of the findings was probably due to the use of different Doppler ultrasound techniques in the assessment of thyroid vascularity. Hiromatsu et al. (3) used color Doppler ultrasound to assess the thyroid vascularity, whereas PDS and HSPDS were used in the present study. In addition, similar quantitative assessment of power Doppler sonograms was found to be useful in differentiating small benign and malignant thyroid nodules (12).
It has reported that in normal thyroids the right lobe is generally more vascular than the left lobe (13,14). However, previous reports did not mention the assessment method of thyroid vascularity or explain the asymmetry of thyroid vascularity. With the use of power Doppler ultrasound, the present study found that there was no significant difference in the mean VI of the right and left thyroid lobes. In fact, the mean VI of the right lobe was slightly, but not significantly, less than that of the left lobe on HSPDS.
The present study showed that the majority of thyroid lobes showed a VI <0.5 on HSPDS (96%), while most of them demonstrated a VI <0.3 on PDS (96%). The results suggested that when VI is used in the differential diagnosis of normal and abnormal thyroid glands, different cut-off values of VI may be needed for HSPDS and PDS. Further studies to investigate the cut-off values of VI in differentiating normal thyroid from different thyroid disorders are suggested.
Contrast-enhanced ultrasound is becoming common in the clinical practice, which improves the sensitivity of ultrasound in detecting vascular flow. However, as contrast-enhanced ultrasound involves the administration of microbubble contrast agent to the patient, it increases the cost of the examination and may be contraindicated to some patients such as pregnant women and patients with severe coronary artery disease.
One limitation of the present study is the lack of information of thyroid hormones of the subjects because of the difficulty in getting consent from the healthy volunteers for the blood test. Another limitation of the study is the lack of information about the working principle of HSPDS to explain its higher sensitivity than that of PDS.
The present study used a manual technique to outline the boundaries of the thyroid glands. In our experience, the image processing of manual outlining the gland and of quantifying the thyroid vascularity for one ultrasound image take about 2 minutes. Further studies to develop an automated system may be able to reduce the image processing time.
Conclusions
HSPDS is more sensitive than PDS in the detection of thyroid vascularity. Using customized algorithm with image-processing software for semi-quantitative assessment of vascular signals on Doppler sonograms is feasible, and it allows objective evaluation of thyroid vascularity.
Footnotes
Disclosure Statement
This study was supported by a grant from Esaote China Limited (H-ZK56), which is the company that markets the ultrasound unit with HSPDS. The authors declare that no other competing financial interests exist.