
Abstract
Background:
Proper candidates to improve the effectiveness of molecular testing for thyroid nodules detected on ultrasonography (US) in a clinical setting are not well known. We aimed at evaluating the effective indication and method of BRAF V600E mutation analysis of aspiration specimens according to the US features of thyroid nodules in a BRAF V600E mutation-prevalent area.
Methods:
A total of 244 patients with 244 thyroid nodules were prospectively classified as malignant and nonmalignant based on US. Thyroid nodules with any malignant US features including spiculated margin, the presence of microcalcifications or macrocalcifications, marked hypoechogenicity, or a taller-than-wide shape were defined as US-positives and those without these features were defined as US-negatives. All patients underwent US-guided fine-needle aspiration (FNA). The presence of the BRAF V600E mutation in FNA specimens was determined by allele-specific polymerase chain reaction (AS-PCR) and direct DNA sequencing. The mutation results were correlated with cytology and either surgical pathology or follow-up.
Results:
Of 244 nodules, 66 were US-positive and 178 were US-negative. The malignancy rate was 92% (61/66) for US-positives and 14% (25/178) for US-negatives. The BRAF V600E mutation was identified in 67% (44/66) of US-positives and in 10% (17/178) of US-negatives. The BRAF V600E mutation for nodules with indeterminate or nondiagnostic cytology was present in 45% (5/11) of US-positives and in 8% (2/26) of US-negatives (p = 0.0168). A false negative cytology with the mutation was found in only one case of the US-negatives. All nodules with the mutation were surgically confirmed as papillary carcinomas. Adding the genetic analysis to the FNA as compared with the FNA alone improved the sensitivity and accuracy for US-positives, whereas there was no significant improvement for US-negatives. With regard to sensitivity and accuracy, the use of the AS-PCR was better than the use of the direct DNA sequencing for US-positives as compared with US-negatives.
Conclusion:
The application of BRAF V600E mutation analysis in FNA specimens is more effective for thyroid nodules with malignant US features as compared with nodules without malignant US features. The use of the AS-PCR is more valuable as compared with the direct DNA sequencing to refine the diagnosis in a clinical setting.
Introduction
Ultrasonography (US)-guided fine-needle aspiration (FNA) is the mainstay for the detection of thyroid cancers and, aside from the information provided by FNA, there are several ultrasonographic criteria that are predictive of thyroid malignancy (10,11). Unfortunately, 5–20% of FNA aspirates are insufficient or nondiagnostic (12 –15). Therefore, the addition of molecular testing can enhance the accuracy of FNA cytology (16). Although the BRAF V600E mutation can be reliably detected, its routine use for all FNA samples is unlikely to be cost-effective. Therefore, it would be important to have information regarding the following: In what thyroid nodules, would BRAF V600E mutation analysis be most useful?
Apart from a physical examination, the first information obtained when a thyroid nodule is first evaluated by US-guided FNA is the characteristics of the US. Therefore, we sought to determine whether US characteristics could predict in which nodules BRAF V600E mutation analysis of aspiration specimens would most likely to be positive. Our study was performed in a region of the world wherein there is a high prevalence of BRAF V600E mutations in PTC.
Materials and Methods
Patients
Our institutional review board approved the study, and informed consent was received from patients before their undergoing the US-guided FNA procedure and genetic analysis. From April 2008 to August 2008, 266 patients with 266 nodules underwent BRAF V600E mutation analysis at our institution. Of the 266 nodules, six nodules were excluded as extrathyroidal lesions such as parathyroid lesions and lymph nodes that were confirmed after FNA. An insufficient quality of nucleic acids was obtained for one nodule, which was excluded from the analysis. Fifteen patients who did not undergo follow-up or surgical excision were excluded. The study ultimately included 244 nodules in 244 patients. Final cytopathological diagnoses and mutation results of the thyroid nodules were analyzed.
Ultrasonographic evaluation for thyroid nodules and follow-up
HDI 5000 or IU22 (Philips Medical Systems, Bothell, WA) ultrasound scanners equipped with a commercially available 7- to 12-MHz linear-array transducer were utilized. Four radiologists who specialized in thyroid
Patients with US-positive nodules (n = 66) were treated with thyroid surgery or had FNA more than twice. The final diagnosis in these patients was based on either (a) the histopathological diagnosis after thyroid surgery (n = 61) or (b) the results of FNA more than twice (n = 5) with the diagnosis being based on the last FNA. Patients with US-negative nodules (n = 178) underwent surgery, a repeat FNA, follow-up
Cytopathological examinations
All patients underwent a US-guided FNA. If a patient had multiple thyroid nodules, FNA was targeted for the most suspicious nodule. The aspiration was also performed in the largest one when the multiple nodules showed similar characteristics on US. Although a patient underwent multiple FNAs for multiple lesions, the sample for gene analysis was obtained only for the most suspicious one in view of cost. FNAs were performed using 22- or 23-gauge needles attached to a 2-mL syringe with or without local anesthesia. The aspirates were expressed onto frosted-end glass slides and were then immediately fixed in 95% alcohol for both Papanicolaou staining and May–Grunwald–Giemsa staining. Cytopathologists were not on site during the FNA procedures. One of four experienced cytopathologists evaluated the slides. The criterion for an adequate smear was the presence of six groups of cells with more than 10 cells per group. The cytological findings of FNAs were classified into four categories: benign, malignant, indeterminate (or suspicious for malignancy), and nondiagnostic. The reference standard for making the final diagnosis of benign or malignant was the last FNA or surgery.
DNA Isolation and Detection of the BRAF V600E mutation
Gene analysis was performed with DNA extracted from FNA specimens. Both direct DNA sequencing and allele-specific polymerase chain reaction (AS-PCR) method were used to detect the BRAF V600E mutation. Scoring for a mutation was considered positive even if only one of the two methods identified the presence of a mutation.
All samples were kept refrigerated until use. Genomic DNA was extracted from aspirated thyroid cells using the QIAamp DNA Mini kit (Qiagen, Chatsworth, CA) according to the manufacturer's instructions. PCR amplification for the analysis of mutations in exon 15 of the BRAF gene was carried out using specific oligonucleotide primer pairs: 5′-TTCATGAAGACCTCACAGTAAAAA-3′ (forward) and 5′-CCACAAAATGGATCCAGACA-3′ (reverse). A 6-μL sample of the DNA template was amplified by PCR in a 20-μL reaction containing 4 μL 5 × BRAF PM and 10 μL 2 × multiplex master mix (Seegene, Seoul, Korea). PCR was carried out on a GeneAmp PCR System 9700 (Applied Biosystems, Foster City, CA) with an initial denaturation step at 94°C for 15 minutes; then 35 cycles at 94°C for 30 seconds, 62°C for 30 seconds, 72°C for 60 seconds, and a final extension cycle at 72°C for 10 minutes. Reaction products were visualized on a 2.0% agarose gel with ethidium bromide. Samples were also analyzed in parallel by direct DNA sequencing with an ABI PRISM 3100 sequencer using the BigDye Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems). DNA sequences were compared with those of the normal BRAF gene exon 15 in the GenBank database using sequence assembly software (Sequencher 4.8; Gene Codes Corporation, Ann Arbor, MI).
Statistical analyses
The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy of the first FNA for the diagnosis of malignancy, AS-PCR, and direct DNA sequencing for the presence of the BRAF V600E mutation were calculated.
The performance of the first FNA alone and the combination of FNA and molecular analysis for the diagnosis of thyroid nodules was compared between US-positive nodules and US-negative nodules using the Mcnemar test and Bennett's method. A p-value of <0.05 was considered to indicate a statistically significant difference.
Results
Clinical and cytopathological findings of the thyroid nodules
The clinical, imaging, and cytopathological findings of 244 patients are shown in Table 1. Of 244 nodules, 66 (27%) were US-positive nodules and 178 (73%) were US-negative nodules (Figs. 1 and 2). The malignancy rate was 92% (61/66) for US-positive nodules and 14% (25/178) for US-negative nodules.
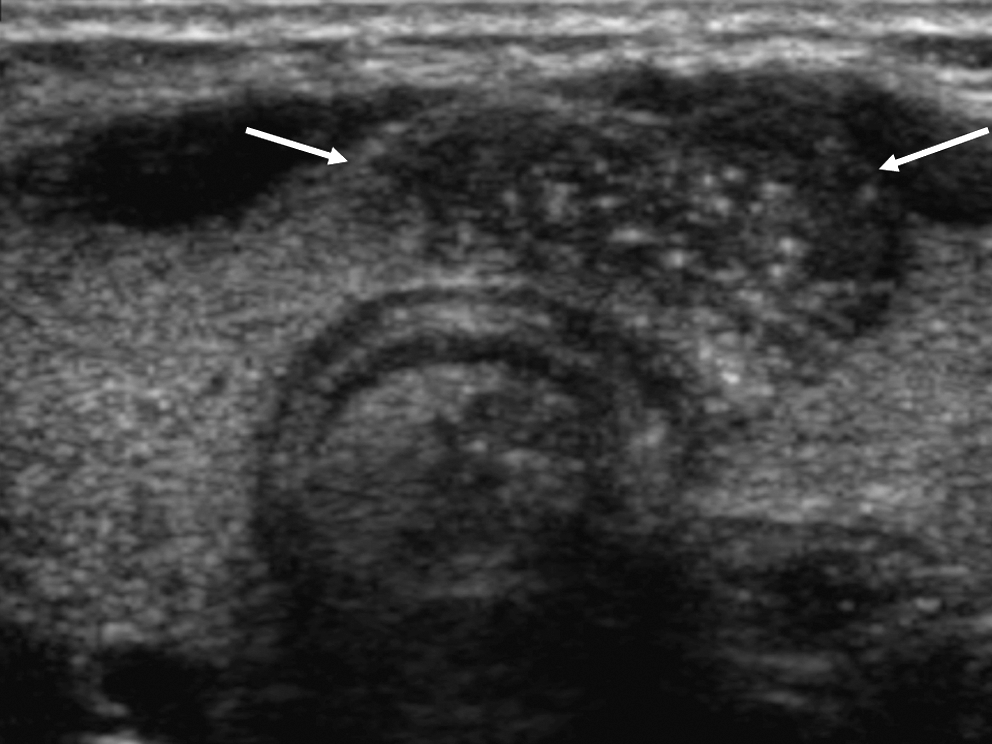
Papillary thyroid carcinoma in a 35-year-old woman. The ultrasonographic image shows a 1.9 cm ill-defined hypoechoic nodule (arrows) with microcalcifications in the paraisthmic portion of the left thyroid gland that was classified as malignancy on ultrasonography (

Transverse ultrasonographic image of papillary thyroid carcinoma in a 53-year-old woman shows a 1.7 cm spiculated, taller-than-wide shaped, and hypoechoic nodule (arrows) with a microcalcification in the right thyroid gland. This nodule was diagnosed as a malignancy based on
FNA, fine-needle aspiration; US, ultrasonography.
Thirty-seven (15%) of the thyroid nodules were diagnosed as indeterminate or nondiagnostic based on the FNA cytology. Indeterminate or nondiagnostic cytology was found for 17% (11/66) of US-positive nodules and for 15% (26/178) of US-negative nodules. All 37 patients with indeterminate or nondiagnostic cytology underwent surgery (n = 20) or a repeat FNA (n = 17). Seventeen (46%) of the 37 nodules were confirmed after surgery as malignancies including 16 PTCs and one follicular thyroid carcinoma (FTC).
Among the 244 thyroid nodules, the reference diagnosis relating to malignancy was based on surgery in 93 (38%) nodules and was based on FNA in 151 (62%) nodules. Among the remaining 151 nodules, 38 (25%) were evaluated by a repeat FNA, and 31 (20%) were only evaluated by a follow-up with US. All 31 nodules with follow-up US that had a benign diagnosis on their initial cytology and US were not changed. The remaining 82 nodules were classified negative for malignancy based on FNA. These were not followed up with imaging, because they were benign on both imaging and cytology. The possibility of some FNA results being false negative cannot be excluded, but we assume that the percentage would be low.
According to the pathological findings in the 93 nodules for which thyroid surgery was performed, there were 85 papillary carcinomas, five cases of nodular hyperplasia, one FTC, one follicular adenoma, and one hyalinizing trabecular tumor. Two of the five patients with nodular hyperplasia underwent surgery for a contralateral papillary carcinoma. Indeterminate cytology, which found it difficult to differentiate nodular hyperplasia from a follicular neoplasm, was present in two cases, and a cosmetic problem was present in one case.
Detection of the BRAF V600E mutation in the FNA specimens
The prevalence of the BRAF V600E mutation in FNA obtained material in the present study was 25% (61) of all 244 nodules and 71% of the 85 PTCs.
The BRAF V600E mutation was identified in 67% (44/66) of US-positive nodules and in 10% (17/178) of US-negative nodules based on AS-PCR analysis (Table 2). The BRAF V600E mutation for nodules with indeterminate or nondiagnostic cytology was present in 45% (5/11) of US-positive nodules and in 8% (2/26) of US-negative nodules (p = 0.0168). One nodule with an initial benign cytology but positive for the BRAF V600E mutation was identified as a malignancy after a repeat FNA and surgery. This was a US-negative nodule.
For FNA performance, the specificity and PPV for malignancy were 100.0% and 100.0%, respectively because there were no false positive cytologies. The sensitivity, NPV, and accuracy of FNA were 79.1%, 89.8%, and 92.6%, respectively. The combination of FNA and testing for the BRAF V600E mutation as compared with FNA alone provided a significant improvement in the sensitivity, NPV, and accuracy (Table 3). The sensitivity and accuracy of the diagnosis of a malignancy in the combination of FNA and testing for the BRAF V600E mutation as compared with FNA alone provided a significant improvement in the case of US-positive nodules but not in the case of US-negative nodules (Table 4).
A p-value of <0.05 was considered to indicate a statistically significant difference. FNA, fine-needle aspiration, which indicates the first FNA; PPV, positive predictive value; NPV, negative predictive value.
A p-value of <0.05 was considered to indicate a statistically significant difference. FNA, fine-needle aspiration, which indicates the first FNA.
Based on direct DNA sequencing analysis, the BRAF V600E mutation was present in 45 (18%) of all 244 nodules. For 16 (26%) of 61 cases wherein the BRAF V600E mutation was detected by AS-PCR, no mutation was found based on direct DNA sequencing. For all 244 nodules, the sensitivity, NPV, and accuracy of AS-PCR were significantly better than in the case of direct DNA sequencing. However, the sensitivity and accuracy of the use of AS-PCR for US-positive nodules were better than those of the use of direct DNA sequencing (p = 0.0018 and p = 0.0018, respectively) (Table 5), although the NPV was not significantly different. There were no significant differences in the sensitivity, NPV, and accuracy between the use of the two methods for detecting the BRAF V600E mutation for US-negative nodules. The specificity and PPV were 100.0% and 100.0%, respectively; no false positives for the mutation in the study population were identified.
A p-value of <0.05 was considered to indicate a statistically significant difference. FNA, fine-needle aspiration, which indicates the first FNA; AS-PCR, allele-specific polymerase chain reaction.
Sixty (75%) of 80 conventional PTCs and one tall cell variant of PTC were positive for the BRAF V600E mutation, but all four follicular variants of PTC were negative for the BRAF V600E mutation. The BRAF V600E mutation was not present in the one FTC.
Discussion
PTC is the most common malignancy of the thyroid gland. Therefore, US criteria for thyroid malignancy are often related to PTC (11,17 –20) and, as such, are also more likely to be associated with the BRAF V600E mutation. Not surprisingly, thyroid nodules with US features that had been associated with malignancy in other studies were also associated with malignancy in our series, and there was a higher prevalence of the BRAF V600E mutation in the US-positive than in the US-negative nodules.
US-guided FNA is the most reliable nonsurgical test for the evaluation of thyroid nodules. Sometimes, however, the cytology is not conclusive either due to insufficient material or due to indeterminate (overlapping) morphological criteria (12 –15,21,22), and molecular analysis of the cytology material is helpful in determining which of these nodules is malignant. In our study, 17% of 244 thyroid nodules were either indeterminate or nondiagnostic. The prevalence of cancer of these 37 nodules was 46%. The BRAF V600E mutation for nodules with indeterminate or nondiagnostic cytology was identified in 45% (5/11) of US-positive nodules and in 8% (2/26) of US-negative nodules, indicating that the utility of testing for the BRAF V600E mutation is relatively low in US-negative nodules with indeterminate or nondiagnostic cytology. On the other hand, if the US is positive and the cytology indeterminate or benign, it may be a good idea to perform molecular analysis.
In our series, only 1 (0.6%) of the 178 US-negative nodules was benign on cytology but was positive for the BRAF V600E mutation. This lesion was later confirmed as malignant. This result suggests that the genetic analysis for US-negative, cytologically benign nodules should be restricted when a very low yield and cost-effectiveness are considered.
We found a significant association between the BRAF V600E mutation and some US features in the present study population. A taller-than-wide shape was more frequent in PTCs with the BRAF V600E mutation than in PTCs without the BRAF V600E mutation (67% vs. 36%; p = 0.0415), and the mean tumor size was smaller for PTCs with the BRAF V600E mutation than for PTCs without the BRAF V600E mutation (0.85 ± 0.609 cm vs. 1.19 ± 0.758 cm; p = 0.0161), although this association was lost on multivariate analysis adjusting for other US features including margin, echogenicity, and the presence or absence of calcifications. It is likely that a taller-than-wide shape seen on US is indicative of the aggressiveness of BRAF V600E mutation, because it means an antiparallel tumoral growth against the usual tissue plane.
The preoperative BRAF V600E mutation results predicted postsurgical clinicopathological characteristics of the PTCs, as recently reported (23). However, we could not observe a significant association between BRAF V600E mutation and poorer pathological findings of PTC, such as extrathyroidal extension (68% vs. 55%; p = 0.2472), lymph node metastasis (52% vs. 59%; p = 0.5503), and multifocality (37% vs. 55%; p = 0.1454). The recurrence rate for PTC could not be reliably predicted in our study due to the short postoperative follow-up period (mean = 8 months). There were no cases of distant metastasis. When US features were correlated, it was likely that PTCs with the BRAF V600E mutation had more aggressive clinicopathological features due to having poorer pathological findings and in this way, they were similar to PTCs without the mutation despite being of a significantly smaller size.
Although the combination of FNA and molecular testing as compared with FNA alone showed a significant improvement in the sensitivity, NPV, and accuracy of the FNA diagnosis, the diagnostic performance according to the US features was significantly different between nodules with malignant US features and nodules without malignant US features. The combination of FNA and BRAF V600E mutation testing was more useful for nodules with malignant US features.
To detect the BRAF V600E mutation in thyroid nodules, various molecular biological methods including PCR-single strand conformation polymorphism, PCR-RFLP, real-time PCR, direct DNA sequencing, and pyrosequencing have been utilized. Chung et al. (24) reported that the sensitivity and specificity of the PCR-RFLP to detect the BRAF V600E mutation were 78.6% and 80.0%, respectively; and the sensitivity and specificity of the direct DNA sequencing were 83.0% and 96.0%, respectively. Therefore, direct DNA sequencing was a more reliable method as compared with the PCR-RFLP to detect the BRAF V600E mutation. Kim et al. (25) have reported that pyrosequencing analysis was superior to direct DNA sequencing to detect the BRAF V600E mutation in thyroid nodules. In the present study, the sensitivity, specificity, and accuracy of the AS-PCR were 70.9%, 100%, and 89.8%, respectively, whereas the sensitivity, specificity, and accuracy of the direct DNA sequencing were 52.3%, 100%, and 83.2%, respectively. The sensitivity and accuracy of the use of the AS-PCR were significantly better than the sensitivity and accuracy of the use of the direct DNA sequencing for US-positive nodules. The AS-PCR seemed to be a more useful complementary tool in addition to FNA for enhancement of the diagnosis to detect a malignancy.
This study has several limitations. First, many cases were not pathologically proved. The study included mostly benign nodules (65%) without the necessity for further surgical resection. Considering false negative FNA (7.4%, 18/244) in the present study, 6 of the 82 nodules with no imaging follow-up can have the possibility of a malignancy. However, the true potential of a malignancy is a 0.5 (0.6% of 82) nodule, because all 82 nodules are US-negative. Therefore, it could not have influenced our conclusions. Second, the comparison of diagnostic performance between AS-PCR and direct DNA sequencing at our institution was not evaluated using both FNA specimens and surgical specimens. A further study is needed to determine the frequency of false-positive or false-negative results. Finally, interobserver variability for the diagnosis of thyroid nodules based on US in patients who were prospectively enrolled can be present, based on the experience of the radiologist.
In conclusion, the use of BRAFV600E mutation analysis of FNA specimens refines the cytological diagnosis in a clinical setting. However, the application of this analysis is more effective for thyroid nodules with malignant features on US as compared with nodules without malignant features. The use of AS-PCR was more valuable when compared with the direct DNA sequencing method to refine the diagnosis.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.