
Abstract
Background:
The accuracy of cancer detection in thyroid nodules by fine-needle aspiration (FNA) cytology and prognostication of thyroid cancer needs further improvement and can benefit from testing for molecular alterations known to occur in thyroid tumors.
Summary:
Recent studies have demonstrated the feasibility of mutation detection in clinical FNA samples from thyroid nodules and their contribution to improving the diagnostic accuracy of FNA cytology. It appears that molecular testing is most beneficial for thyroid FNA samples with indeterminate cytology, where it can resolve the diagnosis in a significant number of cases. In addition to BRAF mutation, which has been studied most extensively, detection of RAS, RET/PTC, and PAX8/PPARγ mutations also contribute substantially to cancer diagnosis. Some of these molecular markers, particularly BRAF, can also be used for tumor prognostication. In clinical setting, molecular testing of thyroid FNA samples and surgically removed tumors should utilize a restricted number of techniques that provide high accuracy and specificity of mutation detection.
Conclusion:
Testing for cancer-specific mutations in thyroid FNA samples and surgically removed tumor tissues increases diagnostic accuracy of FNA cytology and offers better prognostication of thyroid cancer.
Introduction
Most thyroid cancers originate from thyroid follicular cells. They encompass the most common well-differentiated papillary carcinoma (∼80% of all thyroid cancers) and follicular carcinoma (∼15%), as well as poorly differentiated carcinoma (<1%) and anaplastic carcinoma (<2%) (1,2). Follicular carcinomas are further subdivided into conventional and oncocytic (Hürthle cell) types. Poorly differentiated and anaplastic thyroid carcinomas can arise de novo or from preexisting well-differentiated papillary or follicular carcinoma. Follicular adenomas, either conventional or oncocytic type, are benign thyroid tumors that often enter the differential diagnosis of cancer in thyroid nodules. Medullary carcinoma originates from thyroid C cells and accounts for about 3% of all thyroid cancers.
A number of genetic mutations are known to occur in thyroid cancer (Table 1). Papillary carcinomas may carry point mutations of the BRAF and RAS genes and RET/PTC and TRK rearrangements, all of which are able to activate the mitogen-activated protein kinase (MAPK) pathway. These mutually exclusive mutations are found in more than 70% of papillary thyroid carcinomas (3 –6). Follicular carcinomas are known to harbor either RAS mutations or PAX8/PPARγ rearrangement. These mutations are also mutually exclusive and identified in approximately 80% of follicular carcinomas (7). Genetic alterations involving the PI3K/AKT signaling pathway also occur in thyroid tumors, but they are rare in well-differentiated thyroid cancer and have higher prevalence in less-differentiated thyroid carcinomas (8 –10). Additional mutations known to occur in poorly differentiated and anaplastic carcinomas involve the TP53 and CTNNB1 genes (11). Medullary thyroid carcinomas (both familiar and sporadic) frequently harbor point mutations in the RET gene (12).
In clinical practice, the most common and challenging problems involve the diagnosis and prognostication of well-differentiated thyroid cancers; therefore, most of the new developments in molecular diagnostics are centered on these tumor types. As a result, this review is restricted to the discussion of genetic abnormalities found in papillary and follicular carcinomas and their diagnostic and prognostic use.
Molecular Genetics of Thyroid Cancer
Four mutation types constitute the majority of known mutations occurring in papillary and follicular cancers and carry the highest impact on tumor diagnosis and prognostication. They are BRAF and RAS point mutations and RET/PTC and PAX8/PPARγ rearrangements. Among other types of genetic alteration, microRNA (miRNA) markers appear to be the most promising for the diagnostic use at this time.
BRAF
Activating mutations of the BRAF gene is the most common genetic alteration in papillary carcinoma and found in ∼45% of these tumors (4,13,14). About 95% of all mutations involve nucleotide 1799 and result in a substitution of valine to glutamate at residue 600 (V600E). This point mutation leads to constitutive activation of BRAF kinase and chronic stimulation of the MAPK pathway, and is tumorigenic for thyroid cells (15,16). Other and rare mechanisms of BRAF activation in thyroid papillary cancer include K601E point mutation, small in-frame insertions or deletions surrounding codon 600 [reviewed in Chiosea et al. (17)], and AKAP9/BRAF rearrangement, which is more common in papillary carcinomas associated with radiation exposure (18).
BRAF V600E mutation is typically found in papillary carcinomas with classical histology and in the tall cell variant, and is less common in the follicular variant of papillary carcinoma (3,13). This mutation can also be seen in anaplastic and poorly differentiated thyroid carcinomas arising from papillary carcinoma (19 –21). However, BRAF V600E is not found in follicular carcinomas and benign thyroid nodules; therefore, among primary thyroid lesions, it represents a specific marker of papillary carcinoma and related tumor types.
RET/PTC
RET/PTC rearrangement is another genetic alteration found in papillary carcinomas (22). It is formed by the fusion between the 3′ portion of the RET receptor tyrosine kinase gene and the 5′ portion of various unrelated genes. Two most common rearrangement types, RET/PTC1 and RET/PTC3, are paracentric inversions since both RET and its respective fusion partner, H4 or NCOA4 (ELE1, RFG), reside on the long arm of chromosome 10 (23 –25). RET/PTC2 and nine more recently identified types of RET/PTC are all interchromosomal translocations [reviewed in Ciampi et al. (26)]. All fusions contain the intact tyrosine kinase domain of the RET receptor and enable the RET/PTC chimeric protein to activate the RAS-RAF-MAPK cascade and initiate tumorigenesis (27 –29).
RET/PTC is found in approximately 20% of adult sporadic papillary carcinomas, but its prevalence is highly variable between various observations, largely due to the difference in sensitivity of the detection methods and also due to some geographic variability (30,31). RET/PTC occur with higher incidence in patients with the history of radiation exposure (50–80%) and in papillary carcinomas from children and young adults (40–70%) (32 –35). The distribution of RET/PTC rearrangement within the tumor may be quite heterogeneous, varying from involving almost all neoplastic cells (clonal RET/PTC) to being detected only in a small fraction of tumor cells (nonclonal RET/PTC) (36,37). Although RET/PTC has been found in several studies in adenomas and other benign thyroid lesions, it can be assumed that clonal RET/PTC (i.e., rearrangement that is found in most cells within the tumor) is reasonably specific for papillary thyroid carcinoma (30,36). Proper techniques that should be used for the clinically relevant detection of RET/PTC are discussed later in the review.
Among the different types of rearrangement, RET/PTC1 is typically the most common and comprises up to 60–70% of positive cases, whereas RET/PTC3 accounts for 20–30% and RET/PTC2 and other novel rearrangement types for less than 5% (38,39). The exception is a cohort of papillary carcinomas that developed in children within 10 years of exposure to radiation after the Chernobyl accident, where RET/PTC3 was the most prevalent rearrangement type (32). RET/PTC-positive papillary carcinomas typically present at younger age, reveal classic papillary architecture, and have a high rate of lymph node metastases (3).
RAS
Point mutations of the RAS genes are not restricted to a particular type of thyroid tumor and are found in follicular carcinomas, papillary carcinomas, and follicular adenomas. The RAS genes (HRAS, KRAS, and NRAS) encode highly related G-proteins that propagate signals arising from cell membrane receptors. In its inactive state, RAS protein is bound to guanosine diphosphate. Upon activation, it releases guanosine diphosphate and binds guanosine triphosphate (GTP), activating the MAPK and other signaling pathways, such as PI3K/AKT. Normally, the activated RAS-GTP protein becomes quickly inactive due to its intrinsic guanosine triphosphatase (GTPase) activity and the action of cytoplasmic GTPase-activating proteins. Point mutations in the specific domains of the RAS gene either increase its affinity for GTP (mutations in codons 12 and 13) or inactivate its autocatalytic GTPase function (mutation in codon 61). As a result, the mutant protein becomes permanently switched in the active position and chronically stimulates its downstream targets.
In thyroid tumors, mutations involving NRAS codon 61 and HRAS codon 61 are by far the most common, although mutations have been found in different hotspots of all three genes. In papillary carcinomas, RAS mutations occur in 10–20% of tumors (40 –45). Papillary carcinomas harboring RAS mutation almost always have the follicular variant histology; this mutation also correlates with more frequent encapsulation and low rate of lymph node metastases (3,46).
RAS mutations are also found in 40–50% of conventional-type follicular carcinomas (43,47 –51) and 20–40% of conventional-type follicular adenomas (40,47 –50). A lower incidence has been seen in oncocytic tumors (52,53). RAS mutations have also been reported in some adenomatous nodules and goiter nodules, although it is likely that these lesions are true neoplasms and therefore could be better designated as follicular adenomas, despite their frequent macrofollicular and colloid-rich histology.
PAX8/PPARγ
PAX8/PPARγ rearrangement is a result of the translocation t(2;3)(q13;p25), leading to the fusion between the PAX8 gene coding for the thyroid-specific paired domain transcription factor, and the peroxisome proliferator–activated receptor (PPARγ) gene (54). PAX8/PPARγ rearrangement leads to strong overexpression of the PPARγ protein, but the mechanisms of cell transformation induced by this genetic event are yet to be fully understood.
PAX8/PPARγ is found in 30–40% of conventional-type follicular carcinomas, and with lower prevalence in oncocytic carcinomas (7,55,56). Tumors harboring PAX8/PPARγ tend to present at a younger age and be smaller in size, have a solid/nested growth pattern, and more frequently reveal vascular invasion (7,55). This rearrangement can also be found in a small fraction (2–10%) of follicular adenomas and occasionally in the follicular variant of papillary carcinoma (7,56 –58). Follicular adenomas positive for PAX8/PPARγ typically have a thick capsule and show the immunohistochemical profile characteristic of thyroid cancer, suggesting that they may represent preinvasive (in situ) follicular carcinomas or malignant tumors where invasion was overlooked during histological examination (7).
miRNA markers
miRNAs are endogenous noncoding RNAs that negatively regulate the expression of protein-coding genes. miRNAs are dysregulated in different types of cancer, including thyroid cancer, suggesting that aberrations in miRNA expression may be important in tumorigenesis (59). Many miRNAs are expressed in cell type–specific manner and significantly overexpressed or downregulated in tumors as compared to normal tissues, providing a rationale for their potential diagnostic use.
Several miRNAs, including miR-146b, miR-221, miR-222, miR-181b, miR-155, and miR-224, are significantly upregulated in papillary carcinomas, as confirmed by several observations (60 –65). Interestingly, levels of upregulation of some of these miRNAs correlate with the mutational status of papillary carcinomas (60). For example, miR-187 was expressed at higher levels in tumors harboring RET/PTC rearrangements, miR-221 and miR-222 were at the highest levels in BRAF- and RAS- positive tumors and papillary carcinomas with no known mutations, and the highest expression levels of miR-146b were seen in tumors carrying RAS mutations (60). Several upregulated miRNAs were found in thyroid follicular carcinomas (60,66).
Molecular Diagnostics of Thyroid Cancer
Modern molecular techniques allow the detection of these genetic alterations in fine-needle aspiration (FNA) samples from thyroid nodules and in surgically removed tumor tissues, offering additional useful information for the diagnosis and management of patients with thyroid nodules.
Molecular testing of FNA samples
Palpable thyroid nodules are common in the adult population, but only a small proportion of those are malignant. The most reliable diagnostic test for thyroid nodules is FNA cytology, which establishes the definitive diagnosis of a benign or malignant lesion in the majority of cases, whereas 10–40% of all FNA samples are diagnosed as indeterminate for malignancy (67 –70). The general category of indeterminate cytology encompasses several subcategories, that is, follicular lesion of indeterminate significance, follicular neoplasm/Hürthle cell neoplasm, and suspicious for malignancy, which correlate with the estimated risk of malignancy of 5–10%, 20–30%, and 50–75%, respectively (71). Due to the lack of definitive diagnosis, most patients with indeterminate cytology undergo surgery, but only 8–17% of surgically removed thyroid nodules are malignant (72,73). Patients with indeterminate FNA cytology and malignant tumors are not adequately treated as well, since most of them initially undergo thyroid lobectomy and later have another surgery to complete thyroidectomy.
A number of studies have shown that molecular testing of FNA samples significantly improves the accuracy of cytologic diagnosis of thyroid nodules. Most studies have explored the diagnostic role of BRAF mutation. To date, the results of BRAF testing in 2766 samples have been reported, including 9 prospective FNA studies (74 –82), 7 retrospective FNA studies (83 –89) [study of Xing et al. (87) was also partially prospective], and 2 studies of research FNA performed on surgically removed thyroid glands (90,91) (Table 2). All 450 BRAF-positive clinical FNA samples studied prospectively and retrospectively were papillary carcinomas, and only one reported BRAF-positive sample, obtained by research aspiration of the nodule in a surgically removed thyroid gland, appeared to be benign (91). This reportedly benign nodule, pathologically diagnosed as atypical nodular hyperplasia, has not be worked up using modern immunohistochemical techniques helpful in the diagnosis of thyroid malignancy in difficult cases (92), and the nature of atypical changes has not been described or illustrated in the study published (91). Even if this case is accepted as false-positive, it appears that 580 out of the 581 BRAF-positive nodules tested in various types of FNA samples are papillary carcinomas, with a false-positive rate of 0.2%. Importantly, a significant proportion (15–39%) of BRAF-positive FNA samples in many of these studies were indeterminate or nondiagnostic by cytology, demonstrating that testing for BRAF is helpful in establishing the definitive diagnosis of cancer in nodules with indeterminate cytology (74,78,81,84,85,89). In addition, several FNA samples with benign cytology were also tested positive for BRAF, and they were found to be papillary carcinomas after surgery (74,82).
HN reported as atypical nodular hyperplasia (91).
FNA, fine-needle aspiration; HN, hyperplastic nodule; PTC, papillary thyroid carcinoma.
Several studies have explored the possibility of the detection of RET/PTC, TRK, or RAS mutations in thyroid FNA samples (85,93,94). However, the biggest diagnostic impact can be achieved by testing FNA samples for a panel of mutations rather than for a single mutation. A recent study explored the diagnostic utility of molecular testing for a panel of mutations consisting of BRAF, RAS, RET/PTC, and PAX8-PPARγ (74). The study employed 470 consecutive FNA samples from thyroid nodules that were prospectively tested and yielded 32 mutations (18 BRAF, 8 RAS, 5 RET/PTC, and 1 PAX8/PPARγ). The presence of any mutation was a strong predictor of cancer, as 31 (97%) of mutation-positive nodules had a malignant diagnosis after surgery and one case (3%) was a follicular adenoma. This study showed that testing for a panel of mutations is particularly useful in nodules with indeterminate cytology. Among those, the probability of malignancy was 40% based on cytologic evaluation, whereas the addition of molecular testing separated this category into mutation-positive samples with 100% probability of malignancy, and mutation-negative samples with a 14% probability of malignant outcome (Table 3). The molecular testing was especially helpful in the lowest risk subgroup of indeterminate cytology, that is, follicular lesion of indeterminate significance. In this subgroup, the positive mutational status had a 100% accuracy in predicting the risk of a malignancy, whereas mutation-negative nodules were all benign. In addition, this study showed that molecular testing decreased the false-negative rate of cytology from 2.1% to 0.9% (74). However, routine testing of all samples with benign cytology is unlikely to be cost effective. Therefore, further studies are needed to identify a set of clinical and possibly imaging criteria that would determine which nodules with benign cytology should be re-screened using molecular testing.
Based on the data reported by Nikiforov et al. (74).
Regarding specific mutations that constituted the panel, BRAF, RET/PTC, and PAX8/PPARγ mutations had all a 100% positive predictive value for cancer (74). Patients with these mutations would be candidates for total thyroidectomy irrespective of the cytologic diagnosis. This would eliminate the need for intraoperative pathology consultation and subsequent second surgery to complete thyroidectomy, reducing costs and additional morbidity. Detection of RAS mutation, which was the second most common mutation after BRAF, also appeared to be of high diagnostic value in FNA samples, as it conferred a 87.5% probability of malignancy. Importantly, RAS mutations were identified in tumors that are difficult to diagnose by cytology alone, that is, follicular variant of papillary carcinoma and follicular carcinoma. One RAS-positive nodule was diagnosed as a benign follicular adenoma, corresponding to a false-positive rate of 12.5% (74). However, it is conceivable that RAS-positive follicular adenomas serve as precursor lesions for RAS-positive follicular carcinomas (7). Therefore, surgical removal of follicular adenomas that carry this oncogenic mutation by lobectomy may be considered as justifiable to prevent this putative progression.
The accumulation of knowledge on diagnostic use of molecular markers has been reflected in the Revised Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer, recently released by the American Thyroid Association (95). The guidelines indicate that the use of molecular markers, such as BRAF, RAS, RET/PTC, and PAX8/PPARγ, may be considered for patients with indeterminate FNA cytology to help guide management.
The sensitivity of cancer detection by testing for the mutational panel is likely to be further improved by adding other molecular markers such as miRNA known to be upregulated in thyroid cancer. In one study of thyroid FNA samples, three miRNAs (miR-221, miR-222, and miR-181b) were found upregulated in 7/8 (88%) of cytological samples obtained from papillary carcinomas (62). In another study, a set of seven miRNAs (miR-187, miR-221, miR-222, miR-146b, miR-224, miR-155, and miR-197) was able to detect malignancy in thyroid FNA samples with high sensitivity, including tumors tested negative for genetic mutations (60). However, the diagnostic usefulness of miRNA markers has not been validated as extensively as that of the mutational markers, and their clinical diagnostic use awaits additional studies.
Molecular testing of surgically removed tumors
Molecular testing of surgically removed thyroid samples has lower impact on tumor diagnosis compared with the testing of thyroid FNA samples. When the histopathologic diagnosis of papillary carcinoma is suspected, testing of tumor tissue for BRAF and clonal RET/PTC can be of diagnostic value as their presence is a strong indicator of papillary carcinoma. However, many tumors carrying these mutations are classic papillary carcinomas or tall cell variants, and in those cases the histologic diagnosis is typically straightforward. The follicular variant of papillary carcinoma, which more often imposes diagnostic difficulty on surgical pathology examination, most frequently has RAS mutations. However, RAS mutation cannot be used to define malignancy since it can be found in follicular adenomas.
When a surgically removed thyroid nodule is suspected to be a follicular carcinoma, the detection of PAX8/PPARγ rearrangement may be of diagnostic value. As discussed earlier, this mutation can also be seen in a small fraction of follicular adenomas, although the finding of PAX8/PPARγ should prompt the pathologist to perform an exhaustive search for vascular or capsular invasion. The invasion may not be seen at first, but is detected in many PAX8/PPARγ-positive follicular tumors after examination of the entire tumor capsule in multiple histological levels (7,55,96).
Despite the limited diagnostic use, molecular testing of surgically removed thyroid tumors may play an important role in tumor prognostication, as discussed in the next section.
Molecular Predictors of Aggressiveness in Thyroid Cancer
Most well-differentiated thyroid cancers, particularly localized, small-size tumors, have indolent behavior and can be treated more conservatively. Some of these tumors, however, have a potential for more aggressive disease course and therefore require more extensive treatment. It appears that molecular markers can contribute significantly to tumor prognostication.
BRAF
BRAF V600E mutation is generally accepted as a reliable prognostic marker for papillary carcinoma. Its association with more aggressive tumor behavior has been documented in most studies involving sufficiently large cohorts of patients, but some observations have not found such an association [reviewed in Xing (97)]. In many reports, BRAF mutations correlate with aggressive tumor characteristics such as extrathyroidal extension, advanced tumor stage at presentation, and lymph node or distant metastases [reviewed in Xing (97)]. More importantly, BRAF V600E has been found to be an independent predictor of treatment failure and tumor recurrence, even in patients with low stage disease (98 –100). A recent study of 102 papillary carcinomas with a median follow-up of 15 years demonstrated that BRAF V600E mutation was an independent risk factor for tumor-related death (101). Importantly, the association between BRAF V600E and poorer outcome remains significant when mutation detection was performed in thyroid FNA samples (87). This provides a basis for preoperative risk stratification of thyroid cancer.
BRAF activation via BRAF V600E mutation in thyroid cells appears to lead to the alteration of function of sodium iodide symporter and other genes metabolizing iodide, which is likely to be responsible for the decreased ability of tumors with BRAF mutation to trap radioiodine and treatment failure of the recurrent disease (10,102,103). BRAF mutation also predisposes to tumor dedifferentiation and progression to poorly differentiated and anaplastic carcinoma, which is likely to contribute to less favorable prognosis for these patients.
The prognostic implications of BRAF mutation should be of particular importance in papillary microcarcinomas, which are incidentally discovered tumors of 1 cm or less in size. These tumors are commonly found in thyroid samples removed for larger benign nodules. Most of microcarcinomas are indolent tumors cured by surgical resection, but some demonstrate metastatic behavior, recur, and may lead to patient death, and they require more aggressive treatment (104). The role of BRAF mutation in defining a subset of aggressive papillary microcarcinomas remains to be fully defined. However, several recent studies have demonstrated that BRAF mutation in thyroid microcarcinomas correlates with either high rate of extrathyroidal tumor extension or lymph node metastasis or both of these features (105 –107).
Based on a large body of evidence discussed above as well as in recent reviews on this topic (97), BRAF V600E mutation does represent a good marker of aggressiveness that can be applied to papillary thyroid carcinoma as a whole and possibly to specific tumor subtypes such as papillary microcarcinoma. However, it is important to keep in mind that not all BRAF mutation–positive papillary carcinomas are aggressive and not all aggressive papillary carcinomas carry this mutation. Therefore, additional studies are needed to identify the highest risk patients within the BRAF mutation–positive group.
RAS
The role of RAS mutation in predicting more aggressive tumor behavior is not well defined. As this mutation is also found in benign follicular adenomas, the RAS status by itself cannot be used for tumor prognostication. Some evidence exists, however, that RAS mutations in invasive follicular and papillary carcinoma may correlate with more unfavorable prognosis, but this correlation is far from being conclusively established.
Several studies have found a significant correlation between RAS mutation and metastatic behavior of follicular carcinomas, especially with respect to bone metastases, which may be due to the role of RAS mutation in promoting tumor dedifferentiation and transformation to anaplastic carcinoma (41,43,108,109). The association between mutant RAS and more aggressive behavior of papillary carcinoma has been reported in a series of 91 tumors followed on average for 14 years, whereas RAS mutation was found to correlate with distant metastasis and significantly higher mortality rate (42). On the other hand, RAS mutations are frequently found in encapsulated follicular variant of papillary carcinoma, the tumor with an indolent behavior (46,110). Therefore, it is likely that RAS mutations mark a subset of widely invasive well-differentiated thyroid carcinomas that are prone to metastatic spread and dedifferentiation and therefore entail higher mortality, but this mutation cannot be used as a universal prognostic marker for all types of thyroid cancer.
RET/PTC
Correlation between RET/PTC rearrangement and prognosis in human papillary carcinomas remains unclear. Some evidence suggests that the RET/PTC1 rearrangement type is associated with more favorable behavior of papillary carcinomas [reviewed in Nikiforov (111)]. In contrast to papillary carcinomas carrying BRAF and RAS mutations, tumors harboring RET/PTC, particularly RET/PTC1, have a very low probability of progression to poorly differentiated and anaplastic carcinomas (35,39,112).
Practical Issues in Molecular Testing of Thyroid Samples
Although various scientific methods are used to study genetic alterations in thyroid cancer, the detection of mutations and other diagnostic markers for clinical use must be limited to those laboratory techniques that provide highly accurate, reproducible, and clinically relevant information. The choice of most appropriate technique(s) is determined by the mutation type and sample type available for the analysis.
Testing for point mutations, such as those of BRAF and RAS, is relatively straightforward and can be achieved by a variety of molecular techniques, including conventional polymerase chain reaction (PCR) and Sanger sequencing, pyrosequencing, real-time PCR amplification and post-PCR melting curve analysis, and allele-specific PCR (4,20,74,83,89,90,113,114). Some of these techniques are illustrated in Figure 1. These techniques typically provide a reliable and sensitive detection of BRAF mutations in various types of thyroid samples. One study that compared four different approaches, that is, probe-specific real-time PCR, real-time allele-specific PCR, direct sequencing, and colorimetric assay, found all the techniques showing similarly high sensitivity in the detection BRAF mutation in fixed FNA samples (83). However, caution has to be exercised in setting up the sensitivity of a diagnostic assay to avoid ultrasensitive detection of point mutations, which may increase probability of false-positive results and decrease diagnostic specificity.

Commonly used methods for detection of BRAF V600E mutation in all types of thyroid samples are illustrated. (
The choice of a method for the detection of chromosomal rearrangements, such as RET/PTC and PAX8/PPARγ, is dictated largely by the type of sample available. When freshly collected or snap-frozen FNA or tumor tissue samples are available, the testing can be reliably performed by reverse-transcriptase PCR in a conventional or real-time mode (Fig. 2). The sensitivity of detection should generally be not higher than 1% of tumor cells (i.e., should detect 1% or more tumors cells in the background of normal cells) to avoid detecting nonclonal rearrangements, which have no diagnostic implications. When only formalin-fixed and paraffin-embedded tissue is available for testing, fluorescence in situ hybridization is the assay of choice. The appropriate cut-off levels have to be established, which generally should be no less than 8–12% of cells with the rearrangement pattern of signals, as this assure the reliable detection and avoid detecting nonclonal rearrangements (115). Using reverse-transcriptase PCR for clinical detection of RET/PTC and PAX8/PPARγ rearrangements in formalin-fixed and paraffin-embedded tissues should be avoided due to severe RNA degradation, which cannot be compensated by choosing ultrasensitive conditions. The latter results in the loss of diagnostic specificity of the test due to increased detection of nonclonal rearrangement and higher risk of false-positive results. Fixed thyroid FNA samples are generally not suitable for testing for RET/PTC and PAX8/PPARγ rearrangements in clinical setting.
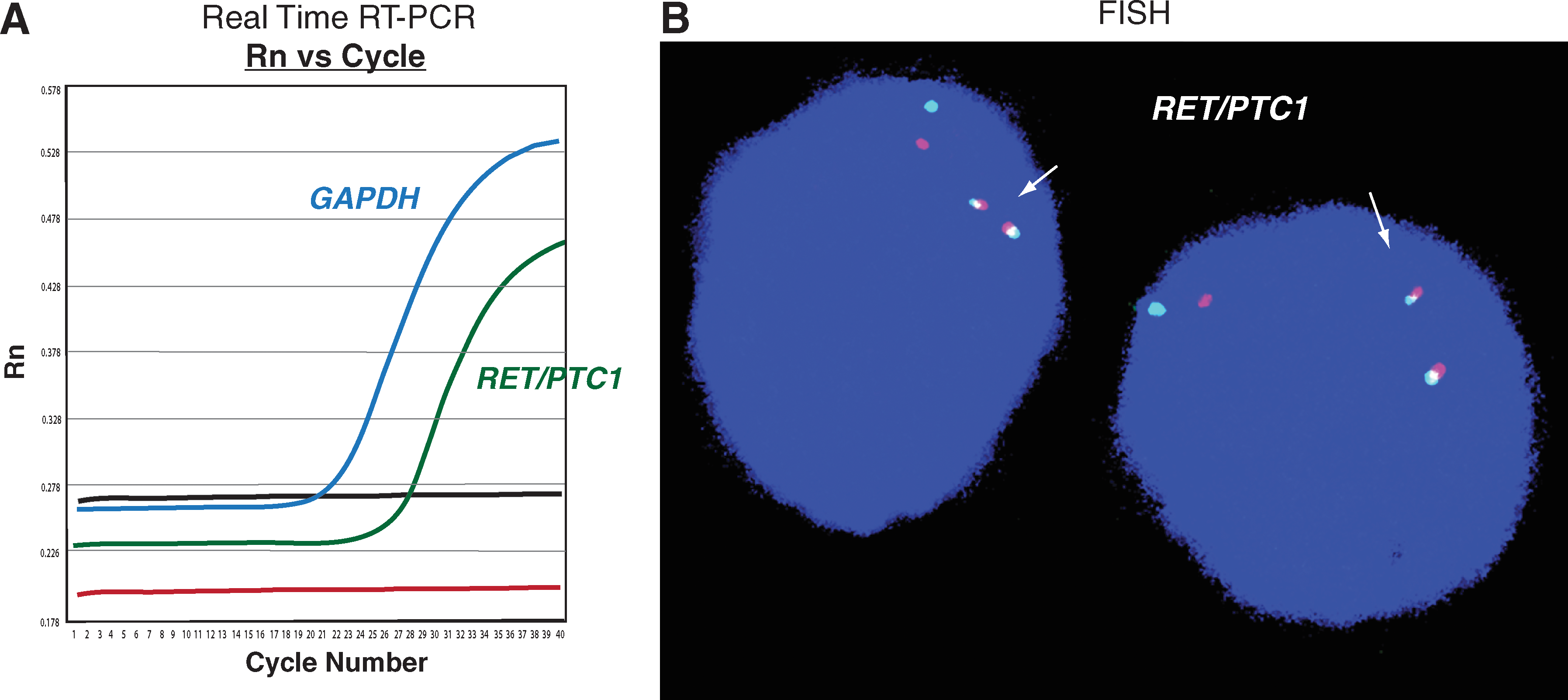
Diagnostic methods for RET/PTC rearrangement. (
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.