
Abstract
Background:
Primary peripheral nerve sheath tumors (PNSTs) of the thyroid gland are exceptionally rare tumors that usually present as asymptomatic neck nodules in adults. This article presents a literature review of these tumors.
Summary:
PNSTs of the thyroid can be classified into benign and malignant. Only three cases of malignant PNSTs have been reported. Benign PNSTs of the thyroid include neurofibromas and schwannomas. Only two cases of isolated neurofibroma of the thyroid have been reported. Schwannomas are typically benign, slow-growing tumors that originate from neuronal schwann cells, with a clinical picture depending on the anatomic size and site. Pathologically, schwannomas are classified into Antoni A and Antoni B. Only 17 cases of schwannomas of the thyroid exist in literature to date.
Conclusions:
Schwannomas of the thyroid gland are extremely rare and usually asymptomatic. Complete surgical resection is mandatory for care.
Benign PNSTs include neurofibromas and schwannomas (2). Neurofibroma is a benign tumor arising from a cutaneous or peripheral nerve. This tumor occurs sporadically or is associated with neurofibromatosis. Neurofibromas mainly occur on the trunk and extremities but may also be found in the head and neck region. Cosmesis is the major concern in these cases. Neurofibromas arise from Schwann cells that exhibit biallelic inactivation of the NF1 gene, which codes for the protein neurofibromin (7).
Isolated neurofibroma of the thyroid is extremely rare. Only two cases have been reported (8,9).
On the other hand, schwannomas originate from neuronal sheath cells(Schwann cells). They are slow-growing tumors that produce other symptoms by compressing vital structures. Their highest incidence has been reported between 40 and 60 years of age (10). Schwannomas are classified microscopically into two types, Antoni type A, which has pallisading, compact, and spindle-shaped nerve-sheath cells, and Antoni type B, which has a sparsely cellular pattern with either cystic degeneration or xanthomatous change. Both types may occur within a single schwannoma (11). The list of differential diagnosis is short, as benign nonepithelial tumors of the thyroid glands are rare and include vascular, smooth muscle, and nerve tumors (12).
Schwannomas generally occur as growths that are closely associated with, but relatively circumscribed from nerves. Most patients with malignant schwannomas are usually between 20 and 50 years of age. A few patients have shown overt evidence of Von Recklinghausen's neurofibromatosis (13,14). It is difficult to make the diagnosis before surgery and the only treatment for thyroid schwannoma is surgical removal (15,16). Fine-needle aspiration is generally unsuccessful for the diagnosis of schwannomas of the thyroid because follicular cells are absent and the remaining cells are difficult to identify. Fine-needle aspiration was able to diagnose thyroid Schwannoma preoperatively in only one patient (15) and there was a report of spindle cells in another patient (10). In an illustrative patient to be presented later, the tumor totally replaced the thyroid tissue and there was no evidence of follicular cells in the preoperative fine needle aspiration (FNA) biopsy to confirm adequacy of the biopsy. Resection results in excellent prognosis (10). Malignant degeneration has been reported, but is very rare (17). Malignant peripheral sheath tumors can be differentiated from other malignant thyroid neoplasms through histological diagnosis with the presence of gross fusiform tumors in relation to nerves, microscopic features of spindle cells with fasicular pattern, areas of necrosis and tumor calcification, and significant cytological atypia or mitotic activity. The immunohistochemical staining for schwannomas is usually positive for S-100 protein and neuron-specific enolase as well as actin, vimentin, cytokeratin, and smooth muscle actin, differentiating this type of tumor from other spindle cell sarcomas. There is also the presence of the MIB1 proliferation marker, which is also used for the grading and prognosis of the tumor (18).
There have been only 17 previously reported cases of schwannomas in the literature summarized in Table 1. Of 17 cases, 9 (53%) were female patients. Their age ranged from 12 to 69 years. Only one of the reported cases had a definitive diagnosis by fine-needle aspiration cytology. Twelve patients of the cases reported had both Antoni A and B features, four cases had only Antoni A, and none of the patients had Antoni B only. Three of the reported lesions appeared hypoechoic on ultrasonography.
FNA, fine needle aspiration biopsy.
The main treatment for thyroid schwannoma is surgical removal. Although it is very rare for schwannoma to occur in the thyroid gland, surgeons and pathologists should be aware that this lesion can occur in this gland and present with the clinical features of a malignancy.
Illustrative Patient
A 70-year-old African American man with a long-standing history of tobacco use presented with hoarseness, 40 pounds weight loss in the year prior to presentation, and progressive dysphagia over a 3-year period. He could only tolerate a liquid diet. Computed tomography scan revealed a left thyroid mass replacing the entire left thyroid lobe measuring 3.6 × 5.4 cm and extending posteriorly causing esophageal compression (Fig. 1).

A computed tomography scan of the upper chest revealing the mass replacing the entire left lobe of the thyroid.
Fine-needle aspiration biopsy of the mass was nondiagnostic because of absence of follicular cells in the aspirate. A standard left thyroid lobectomy was performed and the patient's symptoms resolved.
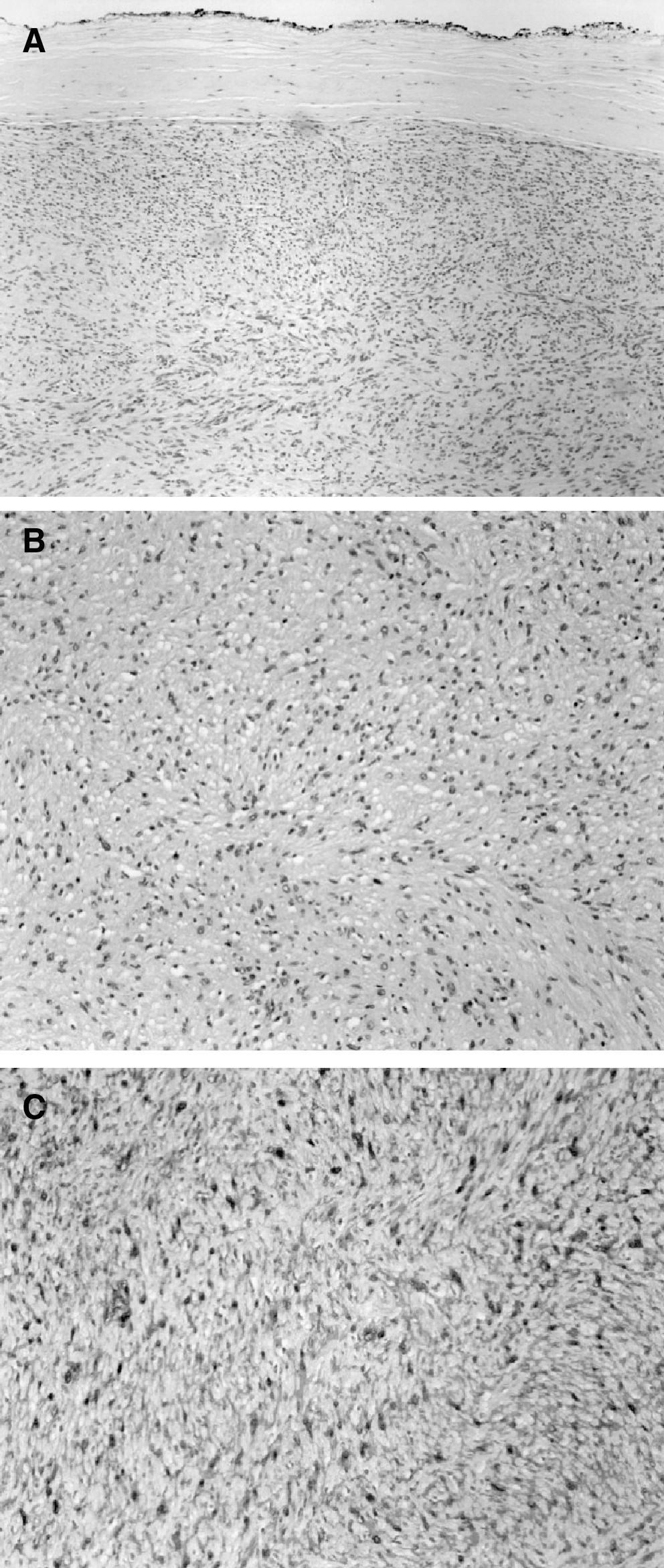
On frozen section, the thyroid mass was noted to be a spindle cell neoplasm. Histological examination showed typical Antoni A and B areas in a well-encapsulated tumor (Fig. 2A, B, respectively). Immunohistochemistry showed that the tumor cells expressed S-100 and vimentin but did not express desmin, muscle-specific antigen, thyroid transcription factor-1 (TTF-1), cytokeratin (AE1/AE3), thyroglobulin, chromogranin, synaptophysin, or smooth muscle actin, consistent with a diagnosis of thyroid schwannoma (Fig. 2C). Interestingly, the schwannoma totally replaced the thyroid tissue and the TTF-1 and thyroglobulin stains were not expressed.
(
The patient was followed up for 1 year with no recurrence of symptoms. Although illustrative, this patient was unusual because of his symptomatic presentation.
In summary, PNSTs of the thyroid gland are quite rare and usually asymptomatic. Most tumors are benign. Schwannomas are the most common type of PNSTs. Isolated neurofibromas are exceedingly rare and usually asymptomatic. Surgical resection is mandatory for symptomatic cases.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.