
Abstract

Graves' disease is an autoimmune thyroid condition in which autoantibodies against the thyrotropin (TSH) receptor stimulate the autonomous production of thyroxine and triiodothyronine. It is characterized by diffuse goiter and thyrotoxicosis and may be accompanied by an infiltrative orbitopathy and dermatopathy. A seldom-recognized feature of this disease is thymic hyperplasia. We would like to highlight this association and consider the pitfalls that can occur when this is encountered by describing a patient with Graves' disease and massive thymus hyperplasia.
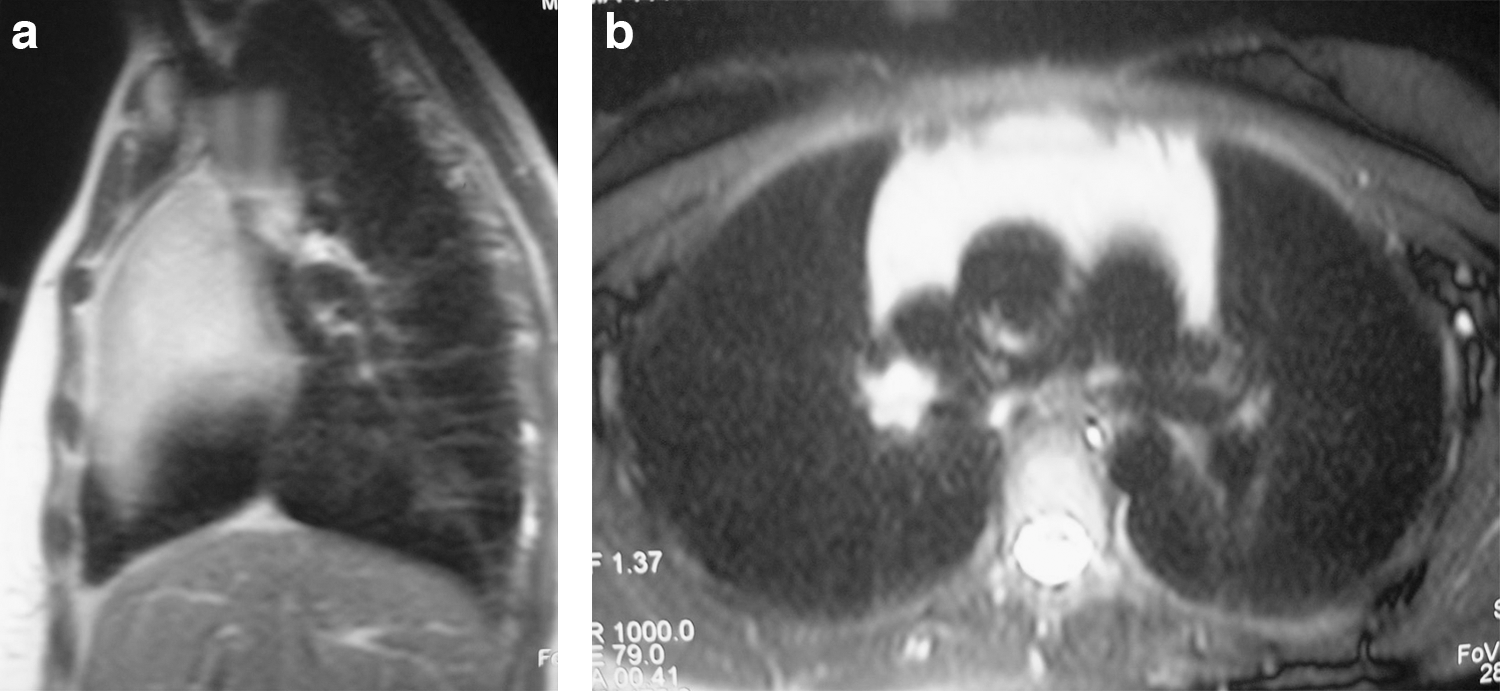
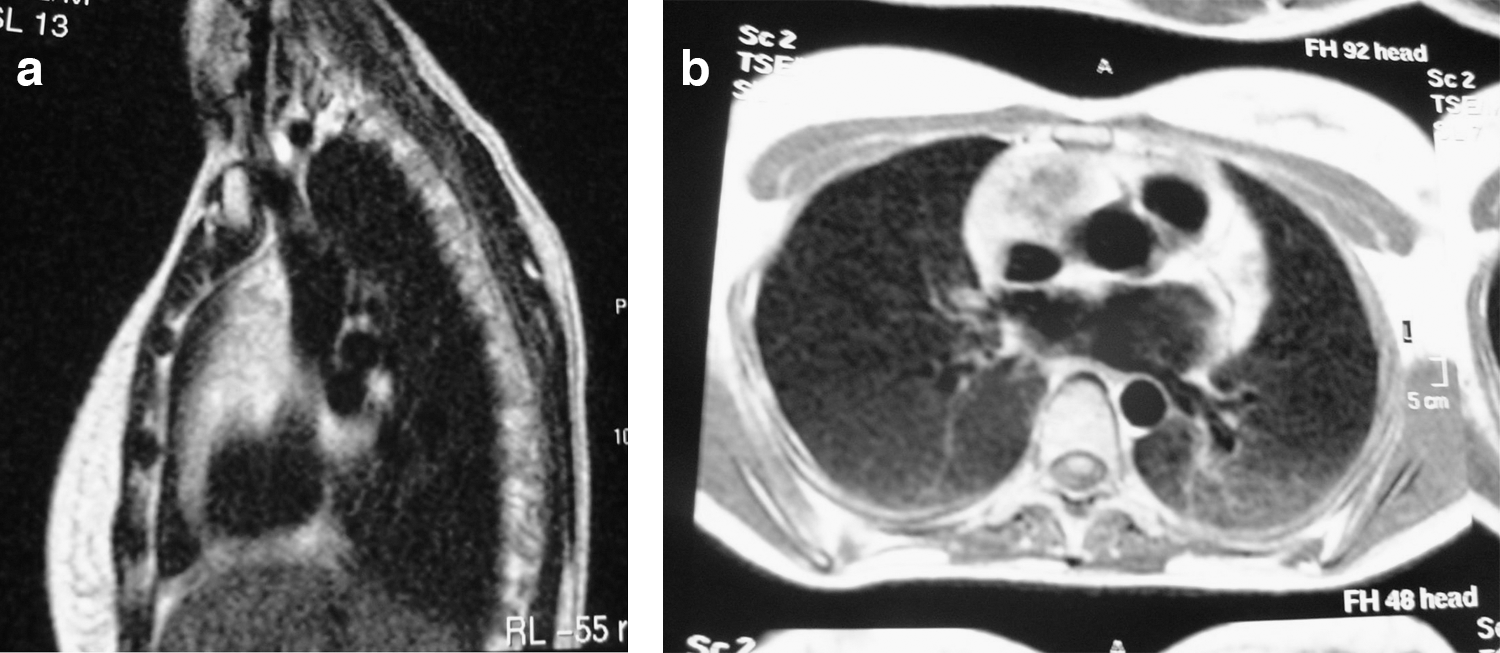
A 22-year-old woman presented with Graves' disease. Serum biochemistry revealed TSH receptor autoantibodies (TRAbs) 178 U/L (normal range: <10 U/L; RIA TRAK-assay [Brahms, patterns MRC LATS-B 65/22 and TSAb Who 90/672), TSH <0.01 μU/mL (0.35–5.5 μU/mL), free thyroxine 4.37 ng/dL (0.89–1.8 ng/dL), and free triiodothyronine 19.41 pg/mL (2.3–4.2 pg/mL). TSH, free triiodothyronine, and free thyroxine levels were determined by a chemiluminescent assay (ADVIA Centaur; Bayer). The patient had marked Graves' ophthalmopathy and an incidentally discovered anterior mediastinal mass (8 × 5 cm) with no invasive characteristics on magnetic resonance imaging (Fig. 1a, b). She was started on treatment with methimazole. There was marked improvement of her thyrotoxic state and concomitant reduction in the size of her thymus (Fig. 2a, b). The patient was treated with total thyroidectomy. Ten months after surgery, the thymic mass regressed to its normal involutionated size at this age—total reduction of 80% (Fig. 3a, b).
(
(

(
Thymic hyperplasia is a common and reversible feature in Graves' disease (1). There are no consistent data between thymic hyperplasia and other hyperthyroid states. It has been suggested that one-third of patients with Graves' disease have microscopic abnormalities in the thymus (2). In most cases, however, thymic enlargement is minimal. Indeed, massive enlargement of the thymus has been reported only infrequently in Graves' disease (1,3). The pathophysiology of thymic hyperplasia in this setting has not been fully determined. However, the fact that treatment of the hyperthyroid state in Graves' disease with concomitant decrease in TRAbs leads to regression of the dimensions of the thymus suggests that thymic hyperplasia is more likely to be the result of Graves' disease (4). Actually, Murakami et al. postulated that both an indirect action of the lowering of thyroid hormone levels and the lowering of TRAbs could induce reduction in the thymus size. It seems that antithyroid drugs, besides causing a blockade of thyroid hormone synthesis, can also have an immunosuppressive effect, namely, reducing TRAbs levels. The same authors have demonstrated the presence of TSH receptor in nonneoplastic thymic tissue, suggesting that this receptor may serve as an autoantigen (5). Their findings support the concept that TRAbs in Graves' disease stimulate that thymic receptor causing thymus enlargement as they induce goiter in Graves' disease.
When the degree of thymic enlargement noted in this patient is encountered, the differential diagnosis must include thymoma, the most common malignant neoplasm of this gland. Adding to the complexity of the correct approach of such cases, it is well known that thymomas are frequently associated with paraneoplastic disorders some of which are endocrine in nature (6). Hyperthyroidism is one of these (7). Although Graves' disease is commonly associated with thymus enlargement, it is much less frequently found in association with thymoma. When the radiological characteristics of the mass suggest benignity (mass homogeneity, no calcifications, and no spreading into surrounding structures), one should rely on these radiological features, treat the hyperthyroid state, and maintain radiological follow-up. Because the benign course of the association between Graves' disease and thymic hyperplasia has been well established in the literature (1), an immediate biopsy in this setting is not required.
Recognition of the common association between Graves' disease and thymic hyperplasia by clinicians is important so that major unnecessary surgery is spared.
Footnotes
Acknowledgment
The authors would like to thank Dr. Paula Campos for reviewing the magnetic resonance images.