
Abstract
Background:
Metastatic carcinomas to the pituitary gland are uncommon, occurring in only 1% of the pituitary masses. They often originate from breast or lung carcinomas and may resemble a nonfunctioning pituitary adenoma both clinically and radiologically. Here we describe a patient with pituitary metastasis from follicular thyroid carcinoma and discuss the unique features of these lesions.
Summary:
A 45-year-old woman was admitted to the emergency rescue room of our hospital with a 2-month history of progressive headache and blurred vision. Evaluation revealed right eye amaurosis, with a mild abducens and oculomotor palsy. Pituitary magnetic resonance imaging showed a mass that was hypo-intense in T1-weighted and hyper-intense in T2-weighted-images, located from the sphenoid sinus up to chiasmatic cisterns, raising and deflecting the optic chiasm, down to hypopharynx region, and distorting the cavernous sinuses. No evidence of anterior or posterior hypopituitarism was recorded. The immediate trans-sphenoidal surgery was uncomplicated with partial improvement of the visual fields and headache. Histopathology revealed a metastasis with well-differentiated follicular thyroid architecture. Total thyroidectomy and lymph node dissection was performed with a final histopathological diagnosis of follicular thyroid carcinoma. Subsequently, her headache became more severe. 131-I ablation treatments were performed 15 days and 12 months after thyroidectomy with decrease in headache and a decline in serum thyroglobulin levels.
Conclusions:
Pituitary metastases from thyroid carcinoma are very uncommon. As this patient illustrates, they tend to produce symptoms relating to space-occupying expansion in the parasellar region rather than to those due to destruction of the pituitary gland. Although rare, pituitary metastases caused by thyroid malignancy should be considered in patients with expanding parasellar lesions if they have thyroid cancer or uncharacterized thyroid diseases. They are unlikely to be amenable to complete resection and should be considered for 131-I treatment, perhaps avoiding the need for extensive neurological surgery.
Introduction
Systemic metastases of thyroid cancers usually go to lung and bone. There are only about 13 reported cases of metastatic thyroid carcinomas to the sella turcica and/or pituitary (5). Here we describe a patient with PMs from an unsuspected follicular thyroid carcinoma. She was initially thought to have a hemorrhagic pituitary adenoma or clivus cordoma.
Patient
A 45-year-old woman with a 2-month history of progressive headache and blurred vision in the right eye was referred through the emergency room to the Neurosurgery Division of our hospital. On admission, she was afebrile with stable vital signs. She was not anemic, and her white blood cell count was normal as were electrolytes and tests for renal and hepatic dysfunction. Ophthalmological examination revealed amaurosis of the right eye and a mild quadrantopsia in the left eye, pale optic discs, and mild right abducens and oculomotor palsy. The medical history was positive for a diagnosis of multinodular goiter 10 years previously, which was treated with L-thyroxine. Seven years before presentation a fine-needle aspiration was performed for a 4.5 cm right medio-basal thyroid nodule. Cytology showed cystic-hemorrhagic changes and was negative for cellular atypia. The patient refused a thyroidectomy. One year before presentation thyroid ultrasonography showed a goiter with partial intrathoracic extension. She developed a headache at least 8 months before presentation that did not respond to common acetylsalicylic acid, paracetamol, or nimesulide.
Brain magnetic resonance imaging (MRI) disclosed a 3.5 cm pituitary mass that was hypo-intense in T1-weighted and hyper-intense in T2-weighted images. It was located on the anterior skull base from the sphenoid sinus up to chiasmatic cisterns, raising and deflecting the optic chiasm, and down to hypopharynx region; the cavernous sinuses were bilaterally distorted. The anterior and posterior pituitary were detected and enclosed in the dorsal profile of the lesion. The internal carotid was surrounded by the mass. The major differential diagnosis based on the imaging study was hemorrhagic pituitary adenoma, clivus cordoma, or sphenoidal mucocele (Fig. 1). A computed tomography scan revealed an intense and homogenous enhancement of the lesion with thinning of the enclosing bone structures (Fig. 2). An angiogram showed a hypervascular pituitary lesion.
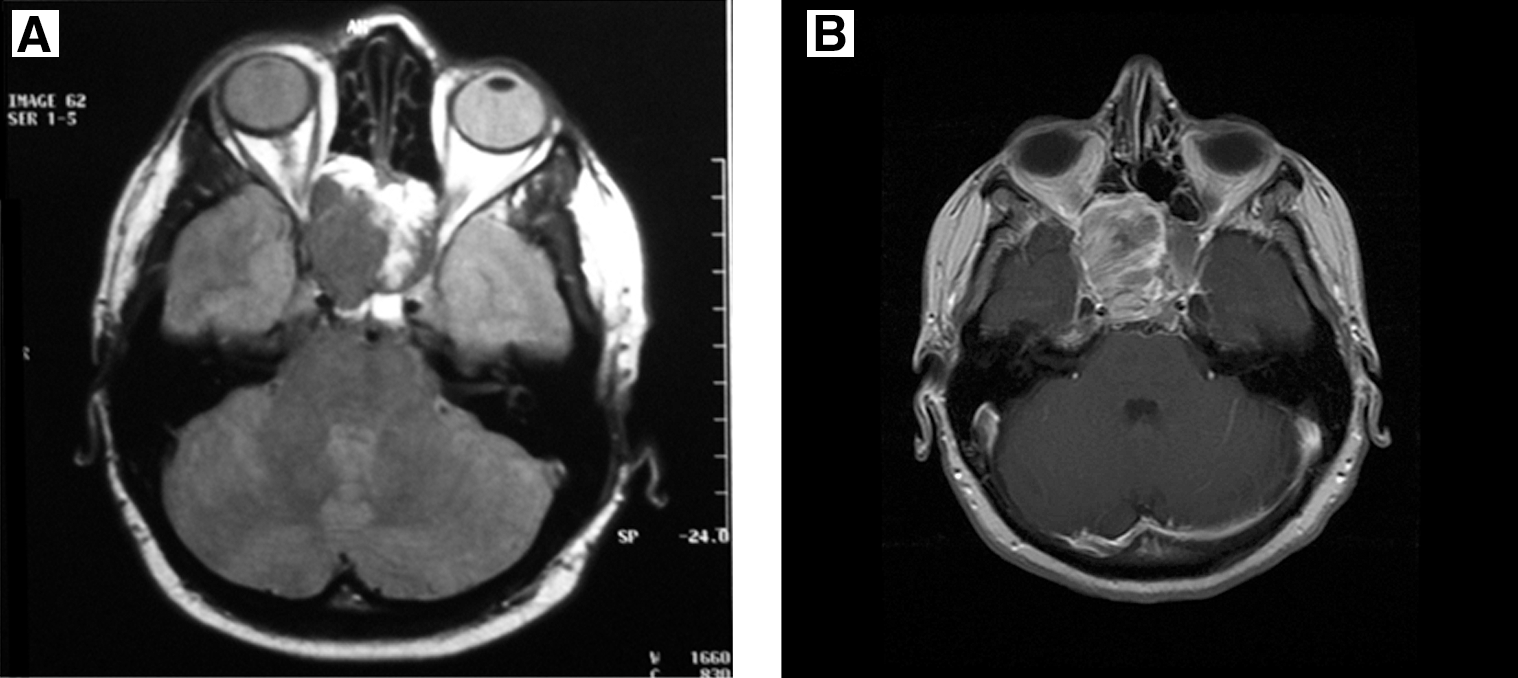
Multiple magnetic resonance imaging (MRI) views with reference mark for bone and pituitary location. (
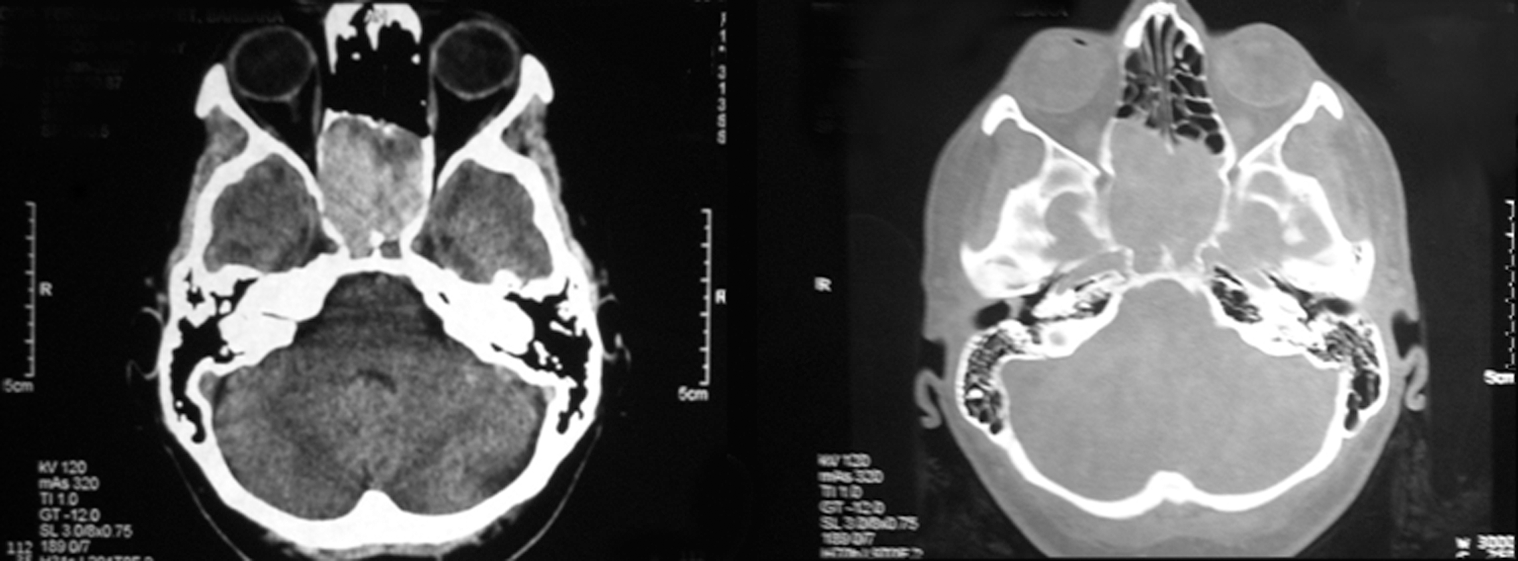
Computed tomography images showing the localized pituitary lesion that shaped and thinned the bone-closing structures.
Other than mild hyperprolactinemia with a serum prolactin of 31.5 ng/ml, there were no biochemical tests suggestive of hypopituitarism; however, these were performed while the patient was on thyroid hormone (Table 1). There were no clinical signs of overt diabetes insipidus, suggesting normal posterior pituitary function. As a precaution she was started on cortisone, and transsphenoidal surgery with removal of the pituitary mass was performed.
Tests conducted few days before (T0) and 18 months after (T1) trans-sphenoidal resection of pituitary metastases. Assays—prolactin: IRMA (PRL-CTK, Sorin; Saluggia); FSH: IRMA (C.T.; Radim); LH: IRMA (C.T.; Radim); TSH: IRMA (C.T.; Biocode); free thyroxine: RIA (Techno Genetics, Cassina dé Pecchi); GH: IRMA (hGH-CTK, Sorin; Saluggia); IGF-I: radioimmunoassay (RIA) (Nicholls Institute); ACTH: IRMA (Allegro HS-ACTH; Nicholls Institute Diagnostic); Cortisol: RIA (CORT–CTK 125, DIA Sorin; Diasorin Diagnostics, Saluggia).
During l-thyroxine treatment (125 μg/day).
During cortisone acetate treatment (37.5 mg/day).
ACTH, adrenocorticotropic hormone; TSH, thyrotropin; FSH, follicle-stimulating hormone; GH, growth hormone; IGF-I, insulin-like growth factor-I; LH, luteinizing hormone; NE, not evaluated; IRMA, immunoradiometric assay.
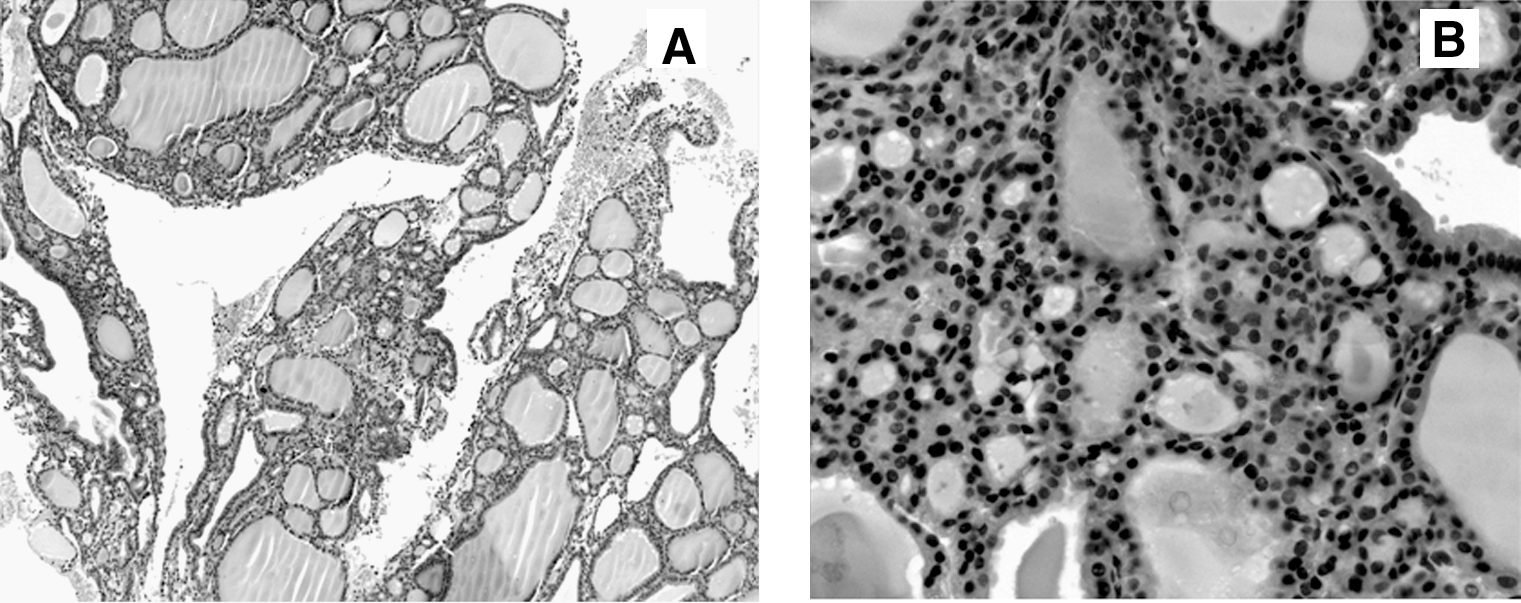
On macroscopic examination the tumor appeared as a hemorrhagic mass; the sphenoidal sinus was downsized to a paper-thin plate. On microscopic analyses no pituitary cells were found. Instead, there was a well-differentiated follicular thyroid tumor. Immunohistochemical analysis revealed no chromogranin A or neuron-specific enolase expression. Rather there was diffuse expression of thyroglobulin (Tg) and cytokeratin-7 and a focal positive staining for cytokeratin-19 and thyroid transcription factor-1 (Fig. 3).
(
After pituitary surgery, the patient developed transient diabetes insipidus. Her visual field defect improved partially and her headaches were less severe. Thyroid ultrasonography as well as neck and chest computed tomography scans showed thyroid enlargement with multiple nodules and marked retrosternal extension that dislocated vessels, trachea, and esophagus. Multiple areas were suggestive for neoplasm degeneration. Ultrasonography demonstrated laterocervical lymph node abnormality, suspicious for neoplastic involvement.
A total thyroidectomy with central and laterocervical lymph node dissection was performed. Histopathology showed a well-differentiated but widely invasive follicular thyroid carcinoma. It was partially encapsulated, but the margins were infiltrated and there was extensive vascular invasion. The structural features varied: there was follicular architecture combined with solid and trabecular areas. The histological characteristics of the thyroid lesion were different compared to the pituitary lesion (Fig. 3). Moreover, lymphonodal metastasis was found (pT2N1M1) (6).
Two weeks after thyroid surgery, the patient presented with deterioration of her clinical condition and sudden intensification of her headache. An MRI showed that the pituitary lesion had grown from 3.5 to 4.5 cm. Because of the concern for hemorrhage and postoperative edema, neurosurgery was considered to be contra-indicated. Therefore, 80 mCi 131-I was administered. The dosage for ablation was determined by quantitative dosimetry as the patient's serum creatinine had increased to 2.5 mg/dL (normal value in our lab: 1–1.5 mg/dL). The patient's pituitary lesion persisted on imaging studies (pituitary MRI), but her clinical status improved. Subsequently, L-thyroxine was temporarily stopped at which time the serum Tg became markedly elevated to 3000 ng/ml. Both whole-body scintigraphy with 131-I and positron emission tomography with flourine-18 fluorodeoxyglucose (FDG/PET) showed marked uptake in the pituitary level and the region of the pelvis (Fig. 4). Therefore, a second 131-I treatment with 80 mCi was performed. This was done 12 months after her thyroid surgery and 15 months after her pituitary surgery. Her last MRI, performed 9 months after the second 131-I treatment, revealed a reduction (RECIST criteria: class PR-30% from baseline in the sum of the individual measurements, confirmed after 4 weeks) (7) in the mass size that was still located on anterior skull base from the sphenoid sinus up to chiasmatic cisterns, raising the right oculomotor nerve and the omolateral cavernous sinus (Fig. 1). The patient's clinical condition improved without headache and bone pain, and with normal vitality and energy. Serum follicle-stimulating hormone, luteinizing hormone, and estradiol levels were in the menopausal range. Serum insulin-like growth factor-I was normal according to age (Table 1). Although there was no definitive evidence for anterior pituitary deficiency, glucocorticoid replacement was maintained as a precaution.
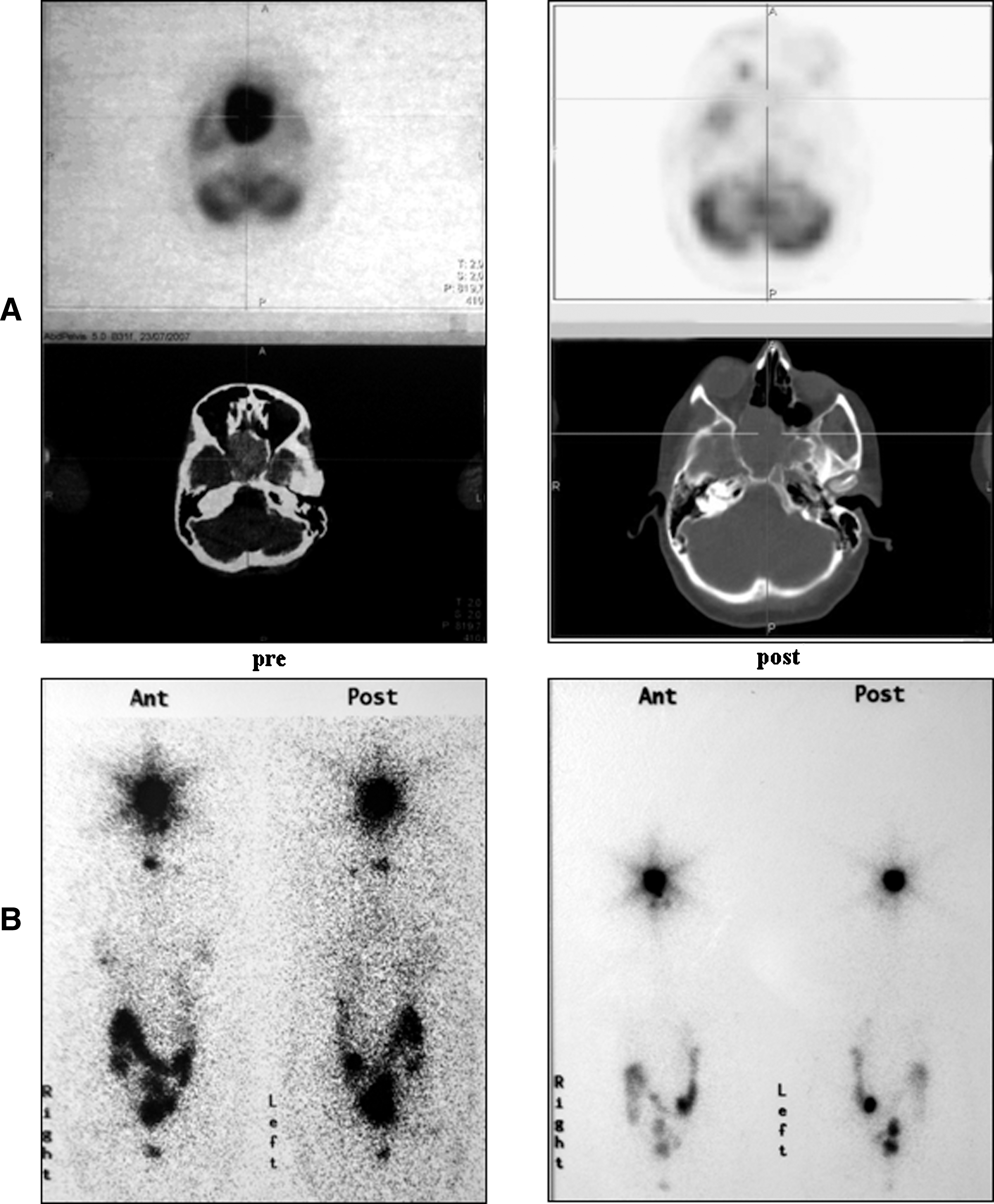
Comparison between PET (
After the second 131-I treatment there was a progressive reduction of serum Tg (Fig. 5). However, because a persistent pituitary uptake on the whole-body scintigraphy, a third 131-I treatment was planned if the patient's clinical and hematological tests permit this.
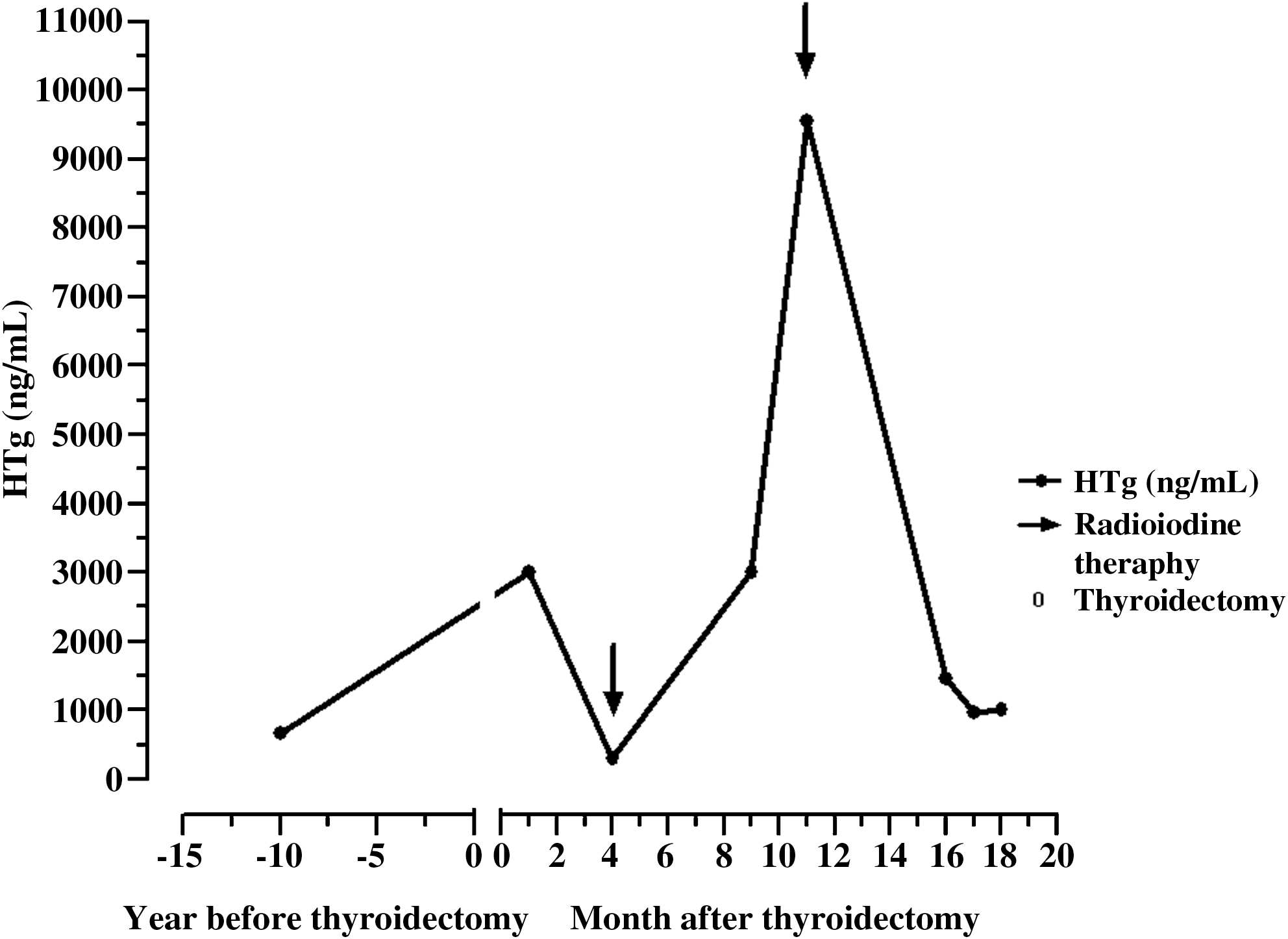
Serum thyroglobulin (HTg) levels in relation to thyroidectomy and 131-I treatment.
Discussion
PMs are an uncommon cause of sellar masses, but the 5% of patients with known malignancies should have a PM according to autopsy data (8). In about two-thirds of patients with PM, their pituitary is macroscopically normal and many are clinically asymptomatic. The prevalence of unsuspected PMs in autopsy examinations ranges up to 27% of all brain metastases (8). In patients with known cancer, a pituitary mass should be strongly considered as a PM from that cancer because the prevalence of pituitary adenomas in patients with a diagnosis of cancer is low, under 2%, according to some sources (1,9).
As noted, PMs from lung and breast cancers are not unusual, but only approximately 13 cases of metastatic thyroid carcinomas involving the sella turcica and/or the pituitary gland have been reported (10 –12). None of these patients had overt anterior or posterior pituitary dysfunction, differing from the situation that commonly occurs when PMs from other cancers occur and are detected ante mortum (4). PMs of thyroid carcinomas generally produce signs and symptoms related to mass effect such as blurred vision, ptosis, oculomotor and abducens nerves palsies, and headache. These symptoms suggest a parasellar lesion with relatively fast growth rather than an intrasellar lesion that destroys pituitary tissue or disconnects the pituitary stalk (11,12). This behavior is also characteristic of thyroid carcinoma in loco, which grows outwardly rather than invasively (13). The only cases of hypopituitarism or diabetes insipidus as first clinical condition at the diagnosis were displayed by a papillary but not follicular thyroid carcinoma (12,14) (Tables 2 and 3).
MRI, magnetic resonance imaging.
PM-T, pituitary metastases of thyroid follicular carcinoma.
On MRI most PMs from cancers other than the thyroid are smaller than adenomas and tend to be hyso-intense characterized by brain parenchyma in T1- and T2-weighted images (3,15,16), lack of sella enlargement, a dumb-bell morphology, and occasional invasion of the third ventricle (2,15). In contrast, the PMs of differentiated thyroid carcinoma do not have these MRI features because they usually show hypo-intense in T1-weighted and hyper-intense in T2-weighted images, destroying the enclosing bone structures. Therefore, if these features are encountered in a PM, this could be a reason to perform thyroid ultrasonography before neurosurgery. However, it is unclear if neurosurgery should be considered as the first therapeutic approach for PMs due to well-differentiated thyroid cancer. This is because 131-I treatment is generally the first choice of therapy for metastatic follicular thyroid cancer (17).
Immunohistochemistry of the PM in our patient revealed diffuse staining for Tg, confirming the diagnosis of metastatic thyroid carcinoma. It was also positive for cytokeratin-7 and for focal staining of cytokeratin-19 and thyroid transcription factor-1. Normal thyroid follicular epithelium is often negative to cytokeratin-19, and the focal staining of this marker is usually distinctive for a follicular adenoma or carcinoma (13).
Conclusions
PMs from thyroid cancers are rare and have different MRI features compared with the far more common PMs that come from lung and breast cancers. They tend to produce signs and symptoms related to mass effect rather than to hypopituitarism. If a patient with a PM has these features, or a known thyroid cancer, the possibility that the PM is from thyroid cancer should be considered. If the patient has a thyroid lesion, this should be characterized in conjunction with the pituitary work-up to rule out PM from thyroid cancer. If there is good evidence that the PM is from thyroid cancer, the possibility of doing minimally invasive surgery to confirm this should be considered along with a consideration of 131-I as the first line of treatment.
Footnotes
Acknowledgments
This study was supported by Regione Piemonte (Ricerca Finalizzata 2008 bis, prot. n. 2133). The authors thank Bastiaan Arler for English revision.
Disclosure Statement
The authors declare that no conflicts of interest or competing financial interests exist.