
Abstract

Lung metastases from differentiated thyroid carcinoma (DTC) are potentially curable, particularly in children and young adults who often live for decades with diffuse pulmonary metastases that have been appropriately treated. Moreover, radioiodine (131I) therapy, also with high cumulative activity, can lead to longer survival time or complete recovery (1). Up to the present time, 131I was the only available systemic modality to treat patients with metastatic disease and for this reason was repeatedly administered, even when it was not clearly effective (2). Since effective therapeutic strategies are scarce at present, severe complications of radioiodine treatment of pulmonary metastases from thyroid cancer, including radiation pneumonitis and fibrosis, cannot be ignored. Herein, we present a patient with DTC lung metastases, who developed pulmonary fibrosis following repeated high-dose radioiodine therapy with high cumulative 131I activity.
A 12-year-old girl, who had a near-total thyroidectomy and functional lymph node resection for papillary thyroid carcinoma in November 2001, presented to our clinic due to suspected extensive pulmonary metastases from thyroid carcinoma. On computed tomography (CT) plain scan of the chest, the pulmonary lesions were described as “innumerable micro-nodules scattered throughout the lungs” (Fig. 1). In January 2002, 3.7 GBq (100 mCi) of 131I was initially given, since miliary tuberculosis had been excluded. Four weeks before 131I therapy, L-thyroxine replacement therapy was withdrawn and low iodine diet protocols were applied. Serum thyroid-stimulating hormone, thyroglobulin (Tg), and Tg autoantibody levels, which were measured by chemiluminescent immunoassay system just before the radioiodine administration, were 125 ng/mL, 5120 ng/mL, and 26 U/mL, respectively. A high retention of radioiodine in the lungs was observed 5 days after radioiodine therapy via 131I scintigraphy, which revealed minimal uptake in the neck and intense uptake throughout both lung fields (Fig. 2). 131I treatment was then repeated periodically with an interval of 6 months using a high fixed dose of 5.55 GBq (150 mCi) due to persistent lung uptake and continuous decrease of serum Tg level. Thyroxine treatment was given at suppressive doses between 131I treatment courses. In July 2007, when cumulative activity of 131I achieved 64.75 GBq (1750 mCi), her stimulated serum Tg decreased to 514 ng/mL and minimal uptake in both lung fields was noticed, suggesting obvious reduction of functional metastases (Fig. 3). Blood cell counts and liver enzymes were always within normal ranges. Unfortunately, a few months later, she developed dyspnea on exertion, and radioiodine therapy was stopped. Over the next 6 months, her shortness of breath progressively increased. Her hypoxia continued to worsen to the point where she could not walk upstairs more than a few meters without becoming severely short of breath. Pulmonary function test revealed a significant decrement in total lung capacity, suggesting interstitial pulmonary fibrosis and restrictive lung disease. Chest CT scan also demonstrated pulmonary fibrosis and thickness of the pleura, in agreement with radiation fibrosis (Fig. 4).

Computed tomography plain scan of chest shows innumerable metastatic micronodules scattered throughout the lungs before radioiodine treatment (
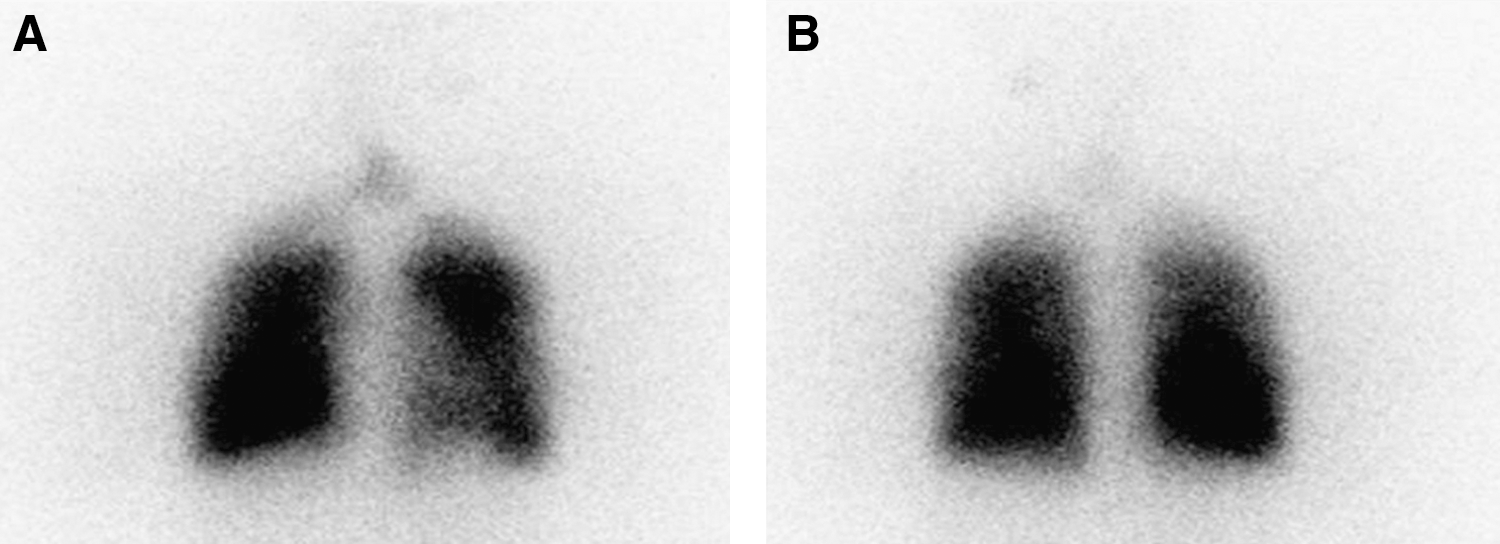
Radioiodine scintigraphy of chest shows intense uptake throughout both lung fields and minimal uptake in the neck 5 days after the first radioiodine administration (
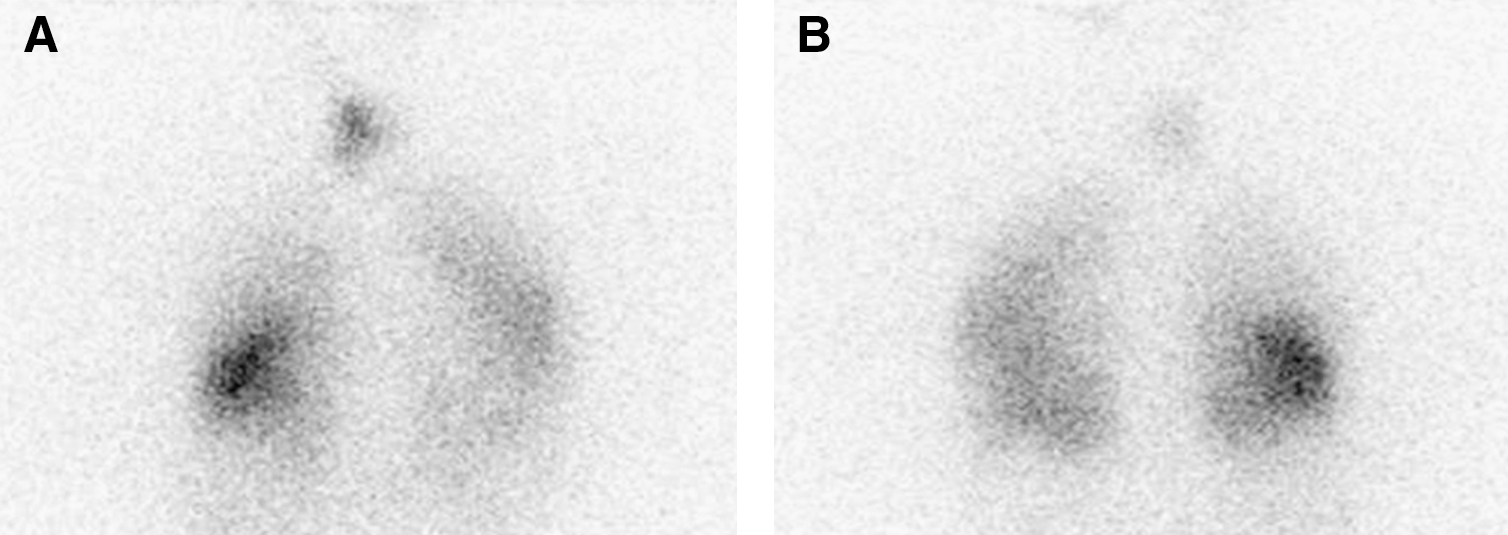
Radioiodine scintigraphy of chest shows minimal uptake in both lung fields and neck 5 days after the last radioiodine therapy (
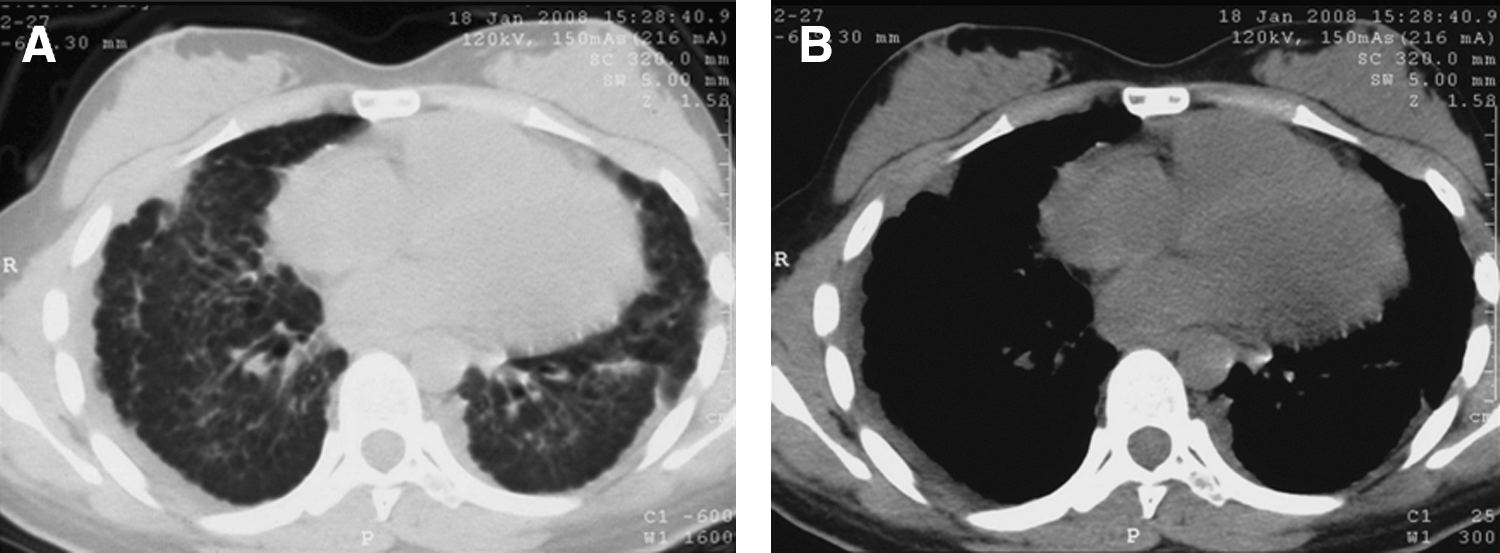
Computed tomography plain scan of chest shows pulmonary fibrosis and thickness of the pleura 10 months after the last administration of radioiodine (
Approximately 10% of adults and 20% of children with DTC develop lung metastases sometime in the course of their disease. Fortunately, long-term survival is especially high when lung metastases are too small to be seen on the standard chest radiograph or CT. Ten-year survival rates are 100% when the metastases are only evident on the posttreatment whole body scan. The 10-year survival rates steadily decline as the metastases become larger, falling to about 40% when there are micronodules (<1 cm) on the chest X-ray and about 15% when the nodules are larger than 1 cm (3).
Although management strategies for lung metastases vary, 131I will continue to be a major weapon in the fight against metastatic disease from DTC (4). Most centers use a fixed-dose approach to radioiodine therapy and prescribe 7.4 GBq (200 mCi) of radioiodine for adults, regardless of the extent or size of the lung metastases. Treatment of children with lung metastases is done in the same way, except that the amount of radioiodine administered is adjusted to the child's size (body surface area). An elegant study by Tuttle et al. showed that this empiric dosing strategy frequently results in administered 131I doses exceeding the maximum tolerable activity safety limit of 200 cGy to the blood or bone marrow in patients who are 70 years old or older. The authors suggested that dosimetry-guided radioactive iodine (RAI) therapy be preferable to fixed-dose RAI treatment strategies in older patients with thyroid cancer and in patients with RAI-avid diffuse bilateral pulmonary metastases, even when renal function is normal (5).
Radiation pneumonitis and pulmonary fibrosis, specifically relative to the presence of lung metastases, were first reported by Rall et al. as potential complications of high activity of radioiodine therapy. The risk of pneumonitis probably increases with disease burden, but this is not a clinically useful indicator of the likelihood of pneumonitis in patients who are known to have lung metastases unless both lungs are diffusely involved with tumor deposits. In this study, the authors pointed out that the most important factor in the development of symptomatic pneumonitis in patients with lung metastases is probably the amount of radioiodine per administration. Specifically, radiation pneumonitis and fibrosis soon after administration of >9.25 GBq (250 mCi) of radioiodine over a wide range of total cumulative doses were reported as complications of radioiodine treatment of pulmonary metastases from thyroid cancer (6).
Our adolescent patient was repeatedly treated with a fixed interval of 6 months, using a fixed-dose approach. Radioiodine activity for single treatment was limited to merely 5.55 GBq (150 mCi), which has been adjusted to the body surface area. Excellent therapeutic effect was obviously noted as Tg levels and the uptake of radioiodine declined steadily, whereas bone marrow suppression was not found. Although we have demonstrated that providing large activities of radioiodine versus smaller ones may have advantages of augmenting the absorbed dose up to two- to threefold and shortening the therapeutic course (7), pneumonitis and lung fibrosis really happened to her 5 years after the first 131I treatment, indicating that a cumulative dose of 64.75 GBq (1750 mCi) possibly induces severe side effects in DTC patients with diffuse lung metastases. This relatively aggressive regime has not been well discussed, because documented cases of pulmonary fibrosis resulting from radioiodine therapy are very few, but the persistent lung uptake and continuous decrease of serum Tg level encouraged us to give a high total administered activity. Compared with macronodular pulmonary metastases in which complete remission is not common and survival remains poor, pulmonary micrometastases have been suggested to be treated with radioiodine and repeated every 6–12 months as long as the disease continues to respond, as the highest rates of complete remission are reported in this subgroup (1,8,9). Besides high single activity, it seems that high cumulative activity is another determinant of pulmonary fibrosis after radioiodine therapy of extensive lung metastases from DTC.
Recent strategies for radioiodine treatment of thyroid cancer in children and adolescents include fixed activities, lesion-based dosimetry, and bone marrow limited approach (10). Reiners group reported that the protocol for children from Belarus treated in their institution included the administration of 50 MBq/kg (1.35 mCi/kg) bodyweight for remnant ablation and 100 MBq/kg (2.7 mCi/kg) for treatment of metastases. They successfully treated many children from Chernobyl with lung metastases with no problems of fibrosis using this tailored therapeutic approach, indicating that this less aggressive regime is less likely to induce fibrosis. Since the ideal activity of radioiodine to treat metastatic thyroid carcinoma is the lowest possible amount of radioiodine that delivers a lethal dose of radiation to the entire lesion/metastasis while minimizing side effects, this individualized regime should be aimed at due to the high life expectancy of this special patient group and the potential impairment of the quality of life. Although fixed activity approach fails to consider the individuality of the patient, it is clinically more widely adopted when compared with lesion-based dosimetry and bone marrow limited approach. More recently, Reiners et al. have also pointed out that pulmonary fibrosis may be a severe side effect in children with thyroid cancer with disseminated lung metastases and intense radioiodine uptake, so the indication for repeated courses of radioiodine therapy has to be thoroughly decided (11). As a result, further studies are still needed to clarify whether another less aggressive regime with longer time intervals between treatments is less likely to induce fibrosis.
Lungs bearing diffuse metastases are often dose limiting after the bone marrow in patients undergoing radioiodine therapy for thyroid cancer. Accurate calculation of lung absorbed dose, however, is difficult in the presence of disseminated tumors, because the micrometastatic disease leads to a heterogeneous tissue density and composition that complicate dose calculation. The assumption that electron energy is locally deposited also becomes invalid due to low density of normal lung tissue. Further, due to the arborizing anatomic structure of the lungs, dose deposition at different locations, such as at bronchi versus alveoli, will likely have different consequences in terms of toxicity. Accurate dose calculation in the lungs, therefore, favors the use of three-dimensional imaging–based, patient-specific Monte Carlo calculations. Additionally, it is important to note that dosimetry-based planning of administered activity has not yielded superior tumor control compared with standard fixed activity (4,12). This may reflect the state of sophistication of dosimetry at the time; the issue needs to be reexamined in light of recent innovations in dosimetry methodology and advances in instrumentation and reconstruction software (13).
There are several considerations to avoid the presence of pulmonary fibrosis caused by radioiodine therapy of lung metastases from thyroid carcinoma. Clinically, one widely adopted dose-planning method developed by Benua and Leeper constrains the therapeutic administered activity so that the absorbed dose to blood does not exceed 200 cGy and the whole body retention does not exceed 4.44 or 2.96 GBq (120 or 80 mCi) at 48 hours after administration in the absence or presence of iodine-avid diffuse lung metastases, respectively (14). In 1991, Hughes et al. suggested the use of spirometry and oxygen diffusion capacity to identify patients who are likely to be at a high risk for lung fibrosis, but this simple approach overestimates the contribution of diffusion limitation by about 30% (15). In the next year, Hsieh et al. established a strategy of low dose radioiodine treatment of thyroid carcinoma, in which progressive decrease of both Tg level and intensity of radioactivity of the lung was noted. After 131I therapy using a cumulative activity of 7.14 GBq (193 mCi), neither pulmonary fibrosis nor bone marrow suppression was seen (16). Recently, Cooper et al. pointed out that limiting single treatment to 7.4 GBq (200 mCi) was almost always sufficient to avoid serious lung injury, but higher cumulative amounts of radioiodine given over an extended period increase the risk of causing lung fibrosis (17). The present patient confirms their findings, as a high cumulative amount of 64.75 GBq (1750 mCi) radioiodine was given over an extended period of 5 years. On the other hand, transforming growth factor-β1 has been suspected, even if not proven, as a key cytokine in progressive fibrogenesis (18). Transforming growth factor-β1 is a multifunctional cytokine critically involved in the pathogenesis of fibrosis through its potent effects on fibroblast differentiation, extracellular matrix formation, and epithelial-to-mesenchymal transition. However, measurement of such a factor as a way of monitoring children treated with radioiodine has not been reported.
Patients who develop pneumonitis must be closely watched, as life-threatening problems can rapidly develop. When symptoms are progressive or severe, steroid therapy is usually indicated. However, Cooper et al. do not advocate using steroids prophylactically before radioiodine therapy, as the withdrawal of steroids may precipitate radiation pneumonitis in patients who would otherwise not develop this problem (17). Recently, Lee et al. pointed out that once end-stage lung disease develops due to radioiodine-induced pulmonary fibrosis or diffuse pulmonary metastases, lung transplantation is often the only feasible option for continued survival and should be considered (19).
In summary, both single and cumulative doses are determinants of pulmonary fibrosis after radioiodine therapy of extensive lung metastases from DTC, and the therapeutic activity of radioiodine has to be limited to a reasonable range. Establishment of a guideline identifying the risk for developing pneumonitis and lung fibrosis would be of great value.
Footnotes
Acknowledgments
This work was sponsored by the National Natural Science Foundation of China (30700187), the Shanghai Rising-Star Program (08QA14040), and the Public Health Bureau of Shanghai Municipality (2006Y34).