
Abstract
Background:
The cytological discrimination between benign and malignant follicular-patterned lesions of the thyroid can represent a diagnostic challenge, even for experienced pathologists. We evaluated the diagnostic use of protein expression of CXC chemokine receptor 4 (CXCR4) and galectin-3 (gal-3) that were found to be upregulated in papillary thyroid carcinoma compared to normal thyroid and of mesothelial cell surface protein recognized by monoclonal antibody Hector Battifora Mesothelial cell (HBME)-1 in thyroid tumors.
Methods:
Expression of CXCR4, HBME-1, and gal-3 was examined immunohistochemically in total of 100 aspirates of thyroid lesions, categorized as benign (n = 22), indeterminate lesion (n = 43), suspicious of papillary thyroid carcinoma (n = 10), or malignant (n = 25) by preoperative cytology.
Results:
Expression of each individual marker was significantly associated with malignancy (p < 0.0001), although the sensitivity of detection ranged from 56% for gal-3 to 94% for HBME-1. When focusing on the indeterminate lesions, only CXCR4 and HBME-1 expression was associated with malignancy; moreover, these two markers either used individually or in combination showed good values of diagnostic accuracy (88.4% and 90.7%, respectively). Further, the combination of CXCR4 plus HBME-1 or the simultaneous use of all the three markers provided absolute value of sensitivity and negative predictive value in the same group of lesions.
Conclusions:
An immunohistochemical panel, including CXCR4, could be useful in the differential diagnosis between benign and malignant well-differentiated follicular-patterned thyroid lesions.
Introduction
The markers Hector Battifora Mesothelial cell (HBME)-1 and galectin-3 (gal-3) have been shown to have the best specificity and sensitivity in distinguishing malignant from benign thyroid lesions (9 –14). The monoclonal antibody HBME-1 was previously shown to be useful in the diagnostic differentiation of the PTCs from its benign mimics (e.g., hyperplastic nodules or FA), both in surgical and FNAB samples (9 –11). Gal-3 is a member of the beta-galactoside-binding lectins and is involved in multiple functions, including cell–cell and cell–matrix adhesion, cell cycle regulation, and apoptosis (15). Its role as a reliable diagnostic marker for preoperative identification of thyroid malignancy has been reported in several studies (11 –14).
To search for an optimal panel of markers, we tested the usefulness of a novel marker, for example, CXC chemokine receptor 4 (CXCR4; also called fusin). This protein is overexpressed in PTC, where it is involved in some biological features of the tumor, such as autonomous proliferation, motility, invasiveness, and metastasis (16).
In this study, we verified the usefulness of a panel of markers, including CXCR4, gal-3, and HBME-1, in the preoperative diagnosis of thyroid lesions.
Materials and Methods
In the current retrospective study, the specimens used for immunohistochemical analysis were obtained from 100 patients who had undergone total or subtotal thyroidectomy for solitary nodule at the Department of Surgery of the University of Pisa from February 2006 to November 2006. Participation in the study required written informed consent.
The preoperative FNAB cytological diagnosis was (i) “benign thyroid nodule” in 22 samples, histologically classified as adenomatoid nodules (21 cases) and FA (1 case); (ii) “indeterminate lesion” in 43 specimens, histologically proven as FAs (19 cases), adenomatoid nodules (9 cases), and FV-PTCs (15 cases); (iii) “suspicious of PTC” in 10 samples, histologically confirmed as pure FV-PTCs (4 cases), classic variants (4 cases), and tall cell variants (2 cases); (iv) “malignant lesions” in 25 specimens, histologically confirmed as PTCs in all cases, in particular, as FV-PTCs in 8 cases, as classic variants in 13 cases, and as tall cell variants in 4 cases (Table 1). Since in the literature there is only evidence of CXCR4 overexpression in PTC (16), each case of indeterminate lesion with a final histological diagnosis of follicular carcinoma was ruled out of the present investigation. Cytological classification was performed according to the second edition of the guidelines for the thyroid cancer management published by the British Thyroid Association (17). The FNAB was performed using a 21-gauge needle attached to a 10-mL syringe preoperatively, under sonografic guidance, or during the surgical procedure. The cytological material was mixed into a hemolytic alcohol-based fixative collection medium, Cytorich Red® Collection Fluid (ThermoElectron Corporation, Waltham, MA). After an incubation of at least 30 minutes in Cytorich Red, to maximize the hemolytic effect, cell suspensions were spun down at 600 g for 10 minutes. The supernatant was poured off and the cell pellet was resuspended in 5 mL of Cytorich Red. In each case, four or five thin-layer slides were prepared (one slide was stained with a rapid haematoxylin & eosin method for the evaluation of adequacy, and three or four were used for immunocytochemistry) using Shandon Cytospin 4® (ThermoElectron Corporation), a thin-layer-cell preparation system capable of producing monolayer of cells, deposited in a defined area of the slide, by use of centrifugal force. This method eliminates cell debris and necrotic material, and lyses red blood cells. Several reports have suggested that thin-layer preparation techniques may achieve a diagnostic sensitivity as high as that found in conventional preparations (18,19). Moreover, this type of processing of cytological samples allows an immunocytochemical staining, both for morphological details and purity of background, of high quality to be performed. In addition, this type of processing allows for the preparation of additional slides for immunocytochemistry from stored cytological material.
FNAB, fine-needle aspiration biopsy; FV-PTC, follicular variant of papillary thyroid carcinoma; CVPTC, classic variant of PTC; TCVPTC, tall cell variant of PTC.
The results of the FNAB and immunohistochemistry were matched with the thyroidectomy biopsy report (gold standard). Histological classification was performed according to the World Health Organization (20).
Immunostaining
All of the immunocytohistochemical analyses were performed automatically using the Ventana Benchmark® immunostaining system (Ventana Medical Systems, Tucson, AZ), preceded by antigen unmasking by heating slides at boiling temperature in prewarmed 1 × Target Retrieval Solution (DakoCytomation, Glostrup, Denmark) for 30 minutes, using a steamer. Any nonspecific staining caused by endogenous biotin was blocked by preincubation with the Endogenous Biotin Blocking Kit (Ventana Medical Systems). Immunostaining for gal-3 and HBME-1 was performed using mouse monoclonal antibodies, provided by Novocastra Laboratories (Newcastle, United Kingdom) and DakoCytomation, respectively, and diluted at 1:100. Immunostaining for CXCR4 was performed using a rabbit polyclonal antibody raised against amino acids 176–293 of fusin, diluted at 1:100, and provided by Santa Cruz Biotechnology Inc. (Santa Cruz, CA). To validate the reliability of the CXCR4 immunostainings with the Santa Cruz's primary antibody, we performed immunocytochemical analysis using another rabbit polyclonal antibody whose immunogen is represented by a synthetic peptide corresponding to N-terminal amino-acids 1–14 of human CXCR4 protein provided by Abcam (Cambridge, United Kingdom; ab 2074), at dilutions of 1:100. Analysis with the second antibody was performed in a subgroup of thyroid lesions, consisting of 20 PTCs and 20 benign thyroid nodules. Further, CXCR4 antibody specificity was assessed using a specific blocking peptide (Abcam; ab 8126) both on cytological and histological specimens, following the manufacturer's instructions. The cytological slides were stained using a diaminobenzidine detection system (Ventana Medical Systems), following the manufacturer's instructions. Diaminobenzidine was used as a chromogen, and commercial hematoxylin was used for counterstaining.
Positive controls included cases of pleural mesothelioma for HBME-1, histiocytes for gal-3, and colon epithelium for CXCR4. For the negative control, all of the reagents described above were used without the inclusion of the primary antibody.
The surgical specimens were fixed in 10% buffered formaldehyde and embedded in paraffin, and then 4-μm-thick sections were cut and stained with hematoxylin & eosin. For immunohistochemistry, paraffin sections (3–5 μm) were dewaxed in xylene, dehydrated through graded alcohols, and processed using the diaminobenzidine detection system, as described above.
Immunostaining was performed with the four above-mentioned antibodies, particularly in those cases that did not show a complete positivity in the panel of tests in the cytological specimens.
Evaluation of immunoreactivity
CXCR4, HBME-1, and gal-3 immunostainings were evaluated by two pathologists (L.T. and F.B.), independently. Differences were resolved by reviewing the slides together. The immunostaining was graded using the following semiquantitative scoring: 0, absent or scant reactivity (<10% of the follicular cells); 1+, focal reactivity (10%–30% of the follicular cells); 2+, moderate reactivity (30%–60% of the follicular cells), and 3+, diffuse reactivity (>60% of the follicular cells). The cases that showed specific staining of more than 10% of the follicular cells, regardless of staining intensity, were scored as positive. The same scoring was used on both the cytological and histological specimens. Cellular localization of the immunostaining was also recorded. Gal-3 immunostaining was always observed in the cytoplasm of the follicular cells; an additional staining in the nucleus was seen only occasionally. HBME-1 immunoreactivity was always observed at the level of the cell membrane; additional cytoplasmic staining was also recorded. In each case, CXCR4 showed a cytoplasmic pattern of immunoreactivity with occasional perinuclear (Golgi-like) staining.
Statistical analysis
Diagnostic accuracy, sensitivity, and specificity were calculated for CXCR4, HBME-1, and gal-3 for the three antibodies individually and in combination as follows: Diagnostic accuracy = true positive + true negative/all positive + all negative Sensitivity = true positive/true positive + false negative Specificity = true negative/true negative + false positive Positive predictive value (PPV) = true positive/all positive Negative predictive value (NPV) = true negative/all negative
The two-sided Fisher's exact test was used to determine the statistical significance with StatSoft 6.0 statistical software (STATISTICA, Tulsa, OK). Concerning the discrimination between benign and malignant lesions, the p-value was calculated as difference between two proportion by STATISTICA software. The level of statistical significance was set at ≤0.05.
Results
CXCR4 expression
Typical examples of CXCR4 labeling using rabbit polyclonal antibodies provided either by Santa Cruz or by Abcam are shown in Figures 1 –3. CXCR4 was found in 48 out of 100 cases, among which none was classified as benign thyroid nodule, 14 as indeterminate lesion, 9 as suspicious of PTC, and 25 as malignant by cytology (Table 2). The same results were observed when CXCR4 immunodetection was performed on corresponding paraffin-embedded tissue sections. Normal thyroid tissue neighboring the nodule was consistently negative. No difference was noted between the anti-CXCR4 antibodies provided either by Santa Cruz or by Abcam.

CXCR4 expression in follicular adenoma. Absence of CXCR4 immunoreactivity in the neoplastic cells in both cytological samples (
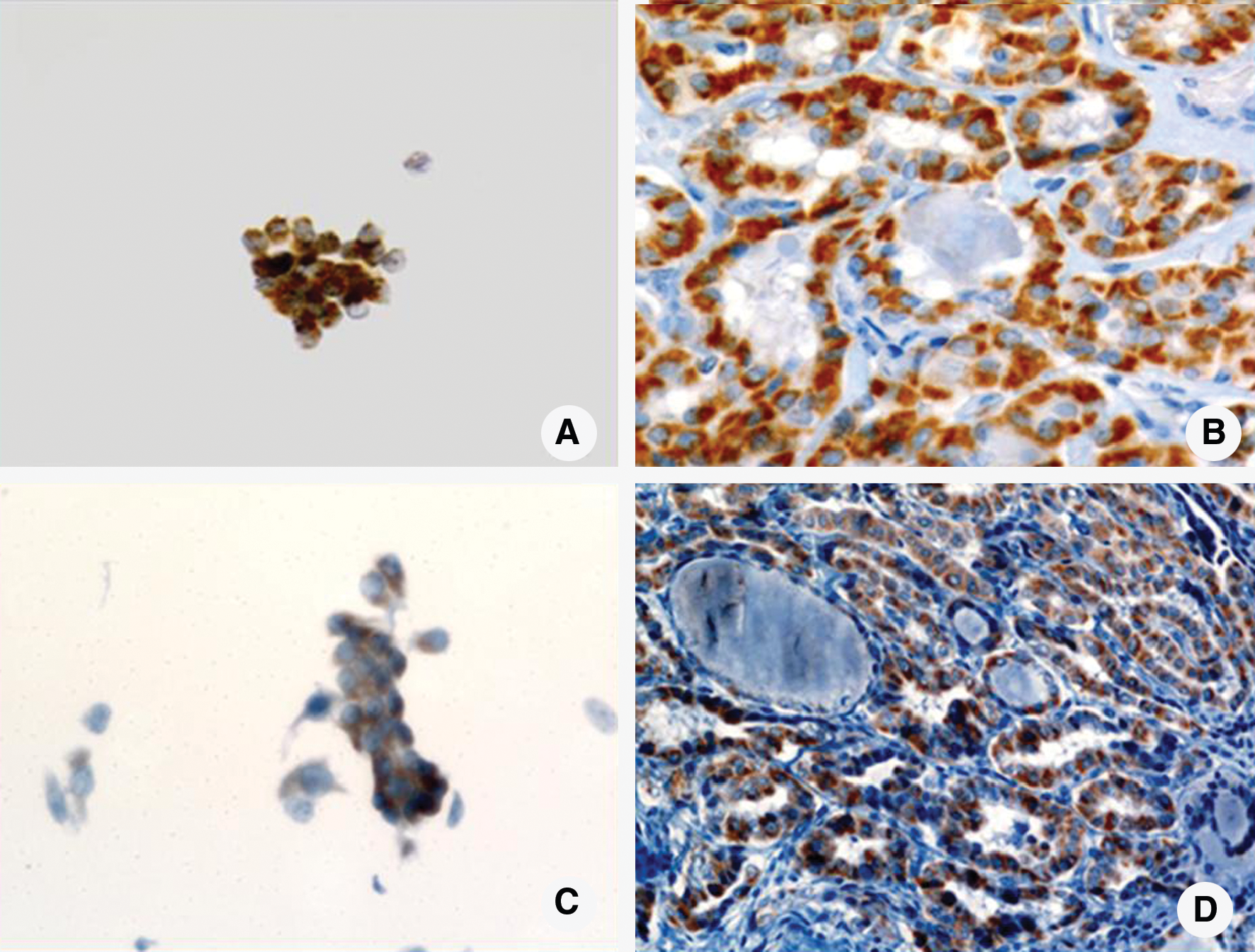
CXCR4 expression in follicular variant of papillary thyroid carcinoma (FV-PTC). (

Comparison between CXCR4 and Hector Battifora Mesothelial cell-1 expression in FV-PTC. (
Benign: follicular adenoma (n = 20); adenomatoid nodule (n = 30). Malignant (PTC): follicular variant (n = 27); classic variant (n = 17); tall cell variant (n = 6).
N.S., not significant (level of statistical significance set at ≤0.05).
Gal-3, galectin-3; HBME-1, Hector Battifora Mesothelial cell; CXCR4, CXC chemokine receptor 4.
Among the 14 indeterminate lesions positive for CXCR4, 12 were diagnosed as malignant (FV-PTCs) and 2 as benign (FAs) by histology. Histological evaluation of the latter two cases demonstrated the presence of a heavy lymphocytic infiltration in the thyroid tissue surrounding the lesion. Moreover, CXCR4 immunodetection in these tissues showed scattered and weak staining in the follicular cells with oxyphilic metaplasia in areas with nonspecific chronic inflammation (Fig. 4).

Thyroid parenchyma. (
Considering all the malignant lesions (n = 50), most tumors (n = 46, 92%) were positive for CXCR4. Positive cases were histologically diagnosed as FV-PTCs in 23 cases, as classic variants in 17 cases, and as tall cell variants in 6 cases. The CXCR4 staining was observed in a variable percentage of cells: in more than 30% cells in 25 cases out of 46 (54.3%) and in more than 60% cells in 12 cases (26%). Among twenty-one malignant cases (45.6%) showing a focal pattern of CXCR4 immunostaining (1+), histology found FV-PTCs in 16 cases and classic variants in 5 cases. The negative cases consisted of four FV-PTCs.
Taking into account all the lesions classified as benign either by cytology or after surgery (n = 50), the majority of these (96%) was negative for CXCR4. Concerning the two positive lesions, the percentage of labeled cells was less than 30%.
HBME-1 expression
HBME-1 immunostaining was negative in 47 out of 50 (94%) benign specimens. The remaining three samples, all cytologically diagnosed as indeterminate lesion, showed a pattern of staining classified as focal (1+) in one case, and as moderate (2+) in two cases. Histologically, all three of the cases were diagnosed as FAs.
HBME-1 immunoreactivity was found in 94% (47 out of 50) of PTCs, showing a strong pattern of cell membrane positivity (3+) in the majority of the cases (34 out of 47). At histological evaluation, positive cases were diagnosed as FV-PTCs in 25 cases, as classic variants in 17 cases, and as tall cell variants in 6 cases. Figure 3 shows an example of HBME-1 immunostaining in a case of FV-PTC. Only three of the FNAB samples with a histological diagnosis of malignancy were negative to HBME-1 immunodetection. Among these, two had a cytological diagnosis of indeterminate lesion and one was cytologically classified as suspicious of PTC. Histologically, all of these cases were classified as FV-PTCs. The same pattern of cytological staining was observed in the corresponding surgical specimens.
Gal-3 expression
Immunocytochemical analysis with anti-gal-3 antibody showed no expression in any of the cases cytologically classified as benign. Among the cases with a preoperative diagnosis of indeterminate lesion, only three cases showed gal-3 positivity. All of these cases were diagnosed as FV-PTC at histological evaluation. Gal-3 immunoreactivity was observed in 6 out of 10 cases cytologically diagnosed as suspicious of PTC and in 19 out of 25 cases with a preoperative diagnosis of malignancy. Histologically, gal-3 positive cases were classified as FV-PTCs in 5 cases, as classic variants in 17 cases, and as tall cell variants in 6 cases.
When gal-3 immunodetection was performed on tissue, normal follicular cells surrounding the nodule were negative, but macrophages, fibroblasts, and endothelial cells expressed gal-3 as expected (12,13).
Gal-3 immunodetection performed on the tissue showed an overlapping pattern that was observed during cytological immunostaining in all cases, except for two neoplasms. These cases, cytologically classified as indeterminate lesion in one case and as suspicious of PTC in the other, showed no gal-3 expression in FNAB specimens. Histologically, they were proven as encapsulated FV-PTC and showed focal gal-3 immunoreactivity limited to the subcapsular regions of the neoplasm.
In summary, Table 2 shows that all the markers (CXCR4, HBME-1, and gal-3) were expressed at a significantly higher level in the carcinomas than in benign lesions (p < 0.0001). Regarding the analysis of immunomarkers on the group of indeterminate lesions, CXCR4 and HBME-1 expression was significantly higher when associated with malignancy (p < 0.0017 and p < 0.0005, respectively). Gal-3 recognized only three of the cases histologically proven as malignant, although none of the benign lesions showed immunoreactivity for this marker (p = 0.36, not significant).
Discrimination between benign and malignant lesions for all the aspirates
Table 3 shows the values of diagnostic accuracy, sensitivity, specificity, PPV, and NPV for all the aspirates, using a single marker or a combination of markers. No statistical difference was found between CXCR4 and HBME-1 (data not shown). Additionally, we investigated the difference between the highest value of CXCR4 or HBME-1 versus gal-3. Only sensitivity and NPV reached the cut-off of statistical significance set at p ≤ 0.05 (p = 0.001 and p = 0.0001, respectively). Further, we evaluated the p-value between the highest value of single marker and the highest value of combination of markers. Although the values of diagnostic accuracy, sensitivity, and NPV of the combination of CXCR4 plus HBME-1 or of all the three markers were higher than those of the single marker, no statistical difference was found. Moreover, no combination of markers showed the absolute value of specificity and PPV of gal-3.
For statistical analysis, when a marker was positive (namely, at least 10% of follicular cells showed specific immunoreactivity), the result was considered as positive.
p-Value was calculated as difference between two proportions by STATISTICA software.
No statistical difference was found between CXCR4 and HBME-1 (data not shown).
p-Value was calculated between the highest value of CXCR4 or HBME-1 versus gal-3 (boldface indicates the value analyzed).
p-Value was calculated between the highest value of the single marker versus the highest value of the combination of markers (boldface indicates the value analyzed).
PPV, positive predictive value; NPV, negative predictive value.
Discrimination between benign and malignant lesions for the aspirates diagnosed as indeterminate lesion by cytology
Table 4 shows the values of diagnostic accuracy, sensitivity, specificity, PPV, and NPV for the aspirates with a cytological diagnosis of indeterminate lesion, using a single marker or a combination of markers. No statistical difference was found between CXCR4 versus HBME-1 (data not shown). In addition, we investigated the difference between the highest value of CXCR4 or HBME-1 versus gal-3. Only sensitivity and NPV reached the cut-off of statistical significance (p = 0.001 and p = 0.03, respectively). Next, we analyzed the statistical difference between the single marker and the combination of markers showing the highest value. No combination of markers reached the cut-off of statistical significance.
For statistical analysis, when a marker was positive (namely, at least 10% of follicular cells showed specific immunoreactivity), the result was considered as positive.
p-Value was calculated as difference between two proportions by STATISTICA software.
No statistical difference was found between CXCR4 and HBME-1 (data not shown).
p-Value was calculated between the highest value of CXCR4 or HBME-1 versus gal-3 (boldface indicates the value analyzed).
p-Value was calculated between the highest value of the single marker versus the highest value of the combination of markers (boldface indicates the value analyzed).
Discussion
In the assessment of a follicular lesion using FNABs, one of the most common pitfalls is the failure to recognize the nuclear features of FV-PTC (4,5). The malignancy rate in cases diagnosed as follicular neoplasm is nearly 20% (5). A revision of the recent literature about follicular lesions, diagnosed on FNAB samples, has shown that the incidence of FV-PTC on histological follow-up ranges from 2% to 22.9% (21). Clinically, it is not necessary to distinguish the FV-PTC from the other variants of PTC on an FNAB, but it is important to distinguish the FV-PTC from an FA or adenomatous nodule (22). The cytological diagnosis of FV-PTC can be extremely challenging because the classical cytological criteria of PTC (i.e., nuclear grooves, pseudoinclusions, and clearing of nuclei) may be partially lacking, or not completely straightforward, and subject to interobserver variation (23 –25).
Several molecules have been identified by immunohistochemistry and reverse-transcriptase polymerase chain reaction to be potential markers (i.e., CD10, thyroid peroxidase, oncofetal-fibronectin, cytokeratin-19, CITED1, and S100C) for the identification of thyroid malignancy (26 –30).
Here, we have compared expression of two well-characterized proteins, HBME-1 and gal-3, to CXCR4 in 100 FNABs, performed on benign and malignant thyroid lesions. We show that certain combinations (such as, CXCR4 and gal-3, or HBME-1 and gal-3) could not provide a marked advantage in separating benign thyroid lesions from malignant thyroid lesions, when compared to the use of a single antibody. Nevertheless, two antibodies, CXCR4 and HBME-1, used individually or in combination, may be useful in the discrimination of benign from malignant lesions in the group of the indeterminate, both in terms of sensitivity and NPV.
CXCR4 is a member of a family of seven-transmembrane G-protein-linked receptors for chemokines, which are capable of mediating several biological responses, such as chemotaxis, cytoskeletal rearrangements, and adhesion (31). Several reports have shown that chemokines and their receptors are involved in the recruitment of leukocytes in the context of a proinflammatory program (32). In cancer, the function of these molecules extends beyond the regulation of leukocyte migration. In particular, the interaction between CXCR4 and SDF-1 (a ligand for CXCR4) promotes metastasis by acting directly on tumor cell migration and invasion (33 –35). Additional evidence supports a role of the CXCR4/SDF-1 axis in the metastatic process (36). It has been shown that high CXCR4 expression in breast, colon and prostate tumors is correlated with neoplastic progression and metastasis (36 –38). As reported by Melillo and colleagues (16), upregulation of CXCR4 is a common event in thyroid cells expressing rearranged during transfection (RET)/PTC rearrangement, suggesting that CXCR4 has an important role in neoplastic proliferation and invasion. Further, expression of CXCR4 by PTCs seems to be associated with indicators of tumor aggressiveness, such as tumor size, extrathyroidal extension, and lymph node metastasis (39).
Our immunohistochemical studies showed that CXCR4 was overexpressed in the majority of PTCs. However, we have noted the prevalence of a focal type (1+) of CXCR4 reactivity among FV-PTCs. This finding needs careful consideration because the semiquantitative scoring could induce differences in the reproducibility of the results, as a consequence of the subjective nature of the evaluation. In addition, we have found low levels of immunoreactivity in some benign lesions (4%) and thyroid tissue, only in association with strong lymphocytic infiltration.
As previously reported by Miettinen and Karkkainen (9), in a study of 463 thyroid tumors, HBME-1 showed strong positive staining in most tumor cells of all PTCs (145 of 145), and no reactivity or only focal staining was seen in one-third of the cases of the benign thyroid lesions. Nevertheless, de Matos et al. (11) have found a focal staining of this marker also in FA (65%) and in adenomatous nodules (33.3%), suggesting that only a diffuse positivity for HBME-1 may be considered to be characteristic of malignancy. Our findings have confirmed the high diagnostic value of this monoclonal antibody by correctly identifying the most PTCs, compared to the other antibodies used here, although 3 out of 50 benign lesions (6%) showed a weak to moderate pattern of HBME-1 expression.
A series of reports have demonstrated that PTC displays an intense and consistent expression of gal-3, without exception (12,13). Accordingly, our analysis has shown that gal-3 expression is significantly associated with PTCs with a classical or a tall-cell pattern of growth (p < 0.001). However, in the group of FV-PTC only a minority of the cases showed gal-3 positivity. As reported by other studies performed on histological samples, or by proteomic analysis on cytological materials (40,41), gal-3 seemed to be expressed less frequently in FV-PTC than in the classical variants, suggesting that there is some difference of immunophenotypic features among these two variants of PTC. Moreover, as we have previously reported (42), the cases of FV-PTC without a diffuse type of growth upon histological examination showed gal-3 immunoreactivity only in a minority of cases. In contrast to other investigators reporting a variable number of false-positive cases (27,29,30), we observed that gal-3 showed an absolute value of specificity (100%); in fact, no one benign thyroid lesion showed gal-3 immunoreactivity in our investigation. However, diagnostic accuracy and sensitivity of gal-3 were low, especially in the discrimination between benign and malignant lesions in the group of indeterminate lesions (72.1% and 20.0%, respectively).
In the present study the values of diagnostic accuracy, sensitivity, and NPV were slightly improved by the addition of CXCR4 to HBME-1 staining, although no statistical difference was found. Additionally, in the discrimination between malignant and benign lesions in the group of indeterminate, the combination of CXCR4 plus HBME-1 or the simultaneous use of all the three markers showed the highest value of diagnostic accuracy, sensitivity, and NPV than did the combination of CXCR4 or HBME-1 plus gal-3. However, this improvement did not reached the cut-off of statistical significance, probably due to the small number of analyzed cases. Moreover, only gal-3 provided absolute value of specificity and PPV in discrimination between malignant and benign lesions both in all aspirates and in the group of indeterminate. No combination of markers reached the level of performance of gal-3, although no statistical difference was noted.
The current study may show some bias regarding the retrospective nature of the investigation and the higher malignancy rate of thyroid lesions (50%) than that more commonly observed (∼20%). Accordingly, the data reported here need independent confirmation in a prospective blinded study, preferably multicenter.
Conclusions
We have shown that two proteins, CXCR4 and HBME-1, were significantly associated with FV-PTC and seemed useful in differentiating the benign from the malignant follicular-patterned lesions, although no statistical difference was observed. Moreover, the NPV of this combination of immunomarkers was very good even in addition to gal-3, suggesting that it could potentially be used safely to spare patients surgery.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist for any of the authors.