
Abstract
Background:
The cytological discrimination between benign and malignant follicular-patterned lesions of the thyroid can represent a diagnostic challenge, even for experienced pathologists. To attempt to clarify this diagnostic problem, we analyzed the BRAF status of thyroid tumors in a group of patients with follicular variant of papillary thyroid carcinoma (FVPTC) and its correlation with cytomorphological features.
Methods:
The BRAF status was evaluated in a total of 187 patients in whom FVPTC was consecutively diagnosed by histology between January 2006 and January 2009. Each case had a previous fine-needle aspiration diagnosis classified according to the British Thyroid Association Guidelines categorized as inadequate (Thy1) (n = 19), benign (Thy2) (n = 19), follicular lesion and follicular lesion with atypia (Thy3) (n = 109), suspicious of PTC (Thy4) (n = 29), or malignant (Thy5) (n = 11). The first 68 cases were selected for a morphological study by a quantitative analysis of four cytological features (grooves, intranuclear cytoplasmatic inclusions, number of cells per high power field (400 ×), and mean nuclear diameter) of the carcinomas.
Results:
The BRAF status of each tumor was correlated with the cytological classes. 54.5% and 27.6% of Thy5 and Thy4, respectively, were BRAF-mutated, against 12.1% of follicular lesions and 9.3% of follicular lesion with atypia (Thy3). This comparison was statistically significative (p = 0.0017). Among the 68 cases selected for the cyto-morphological study, the BRAF status frequency was similar to that of the total case series. No significant differences were found correlating the cytological classes with the number of cells, the number of grooves, and the mean cell diameters. Only the number of intranuclear cytoplasmatic inclusions were associated (p < 0.05) with the Thy5 cytological class.
Conclusions:
BRAF is mutated in a low percentage of FVPTC, and most of these mutated cases are suspicious or positive on fine-needle aspiration. BRAF analysis is of limited value in the preoperative diagnosis of FVPTC.
Introduction
Currently, cytological examination of FNA by expert pathologists provides the most reliable information. However, in a large number of nodules, cytological examination is inconclusive, either because of an insufficient number of follicular cells or because undefined morphological criteria are present. In fact, in a recent series, 20% of indeterminate FNAs were malignant (2). At our institution, 63% of thyroid nodules were reported as either indeterminate or insufficient; among these, 73% were follicular adenoma and 22% were papillary carcinomas. Among the group of papillary carcinomas, 32% belonged to the follicular variant of PTC (FVPTC), suggesting that a major diagnostic dilemma is the distinction between the follicular adenoma and the FVPTC.
In FNA samples, worldwide difficulties reported in a differential diagnosis of follicular adenoma and the FVPTC are reported. These difficulties are due to the fact that many of the typical nuclear findings associated with PTC, such as nuclear grooves, hypochromasia, and pear shaped or ovoid nuclei, are not readily apparent on cytological examination due to artefacts or the sampling of a particular area does not include nuclei with those changes. This fact is supported by the study of Baloch and colleagues (2), which reported that 30% of FVPTC cannot be diagnosed by FNA. Thus, more suitable techniques are needed to differentiate between FVPTC and benign follicular lesions.
Many attempts to identify markers for thyroid carcinoma that can preoperatively distinguish between benign and malignant nodules have been reported. Among these markers, Gal-3, CITED1, HBME-1, Ras, RET/PTC, PAX8/PPAR (3), hTERT (4), and CXCR4 (5) have not been specific enough when used individually. Many molecular studies, including microarray technology and molecular profiling, have been used to differentiate between PTC and benign nodules (6,7). Only a few studies, however, have reported the evaluation of a large series of cases of FVPTC (8).
Materials and Methods
Inclusion criteria
We selected from our files all of the cases that had a diagnosis of FVPTC between January 2006 and January 2009. Three skilled pathologists examined all the cases microscopically and independently. The tumors were classified as FVPTC if they were composed completely or almost entirely (99% of the tumors) of follicles lined by cells that had the nuclear features of PTC. The presence of tumor necrosis or increased mitotic activity (≥5 per 10 high power field [HPF]) excluded the tumors from the FVPTC category.
Pathology review
The three pathologists independently confirmed that there were 187 (87%) FVPTC cases present in the initially selected 216 cases. Therefore, we eliminated 29 of the cases, because at least 1 of the 3 disagreed. Only preoperative-air-dried and alcohol-fixed-Papanicolaou-stained FNAs were considered.
Cyto-pathological evaluation
As previously reported (9), the cytological criteria used for the diagnosis of follicular lesions without atypia are the following: (a) increased cellularity with a small uniform follicular organization and scant colloid and (b) follicular cells having small nuclei with regular distributed chromatin. In the follicular lesions with atypia, the most relevant cytological findings were hypercellularity with solid form, well-defined nests, the rare exhibition of overlapping nuclei, the presence of a large number of isolated cells, and the absence of colloid. In addition, the follicular cells showed enlarged nuclei with sparse or irregularly distributed chromatin, rare prominent nucleoli, and occasional mitosis. All of the cases were classified according to the British Thyroid Association Guidelines (10). This classification comprises five cytological classes (Unsatisfactory, Thy1; Benign, Thy2; Indeterminate, Thy3; Suspicious for malignancies, Thy4; Malignant, Thy5). The Thy3 category includes the classes in the Bethesda system for reporting thyroid cytopathology that are “atypia of undetermined significance or follicular lesion of undetermined significance,” “suspicious for a follicular neoplasm,” and “suspicious for a Hürthle cell follicular cell neoplasm” (11).
Evaluation of the four selected pathological features of PTC (grooves, intranuclear cytoplasmatic inclusions, number of cells per HPF, and mean nuclear diameter)
In the first 68 histologically diagnosed FVPTC cases, various microscopic criteria were studied, by a quantitative analysis. These criteria (the number of neoplastic cells, the mean nuclear diameter, the number of grooves, and intranuclear cytoplasmatic inclusions [ICI]) are largely described as a gold standard for the diagnosis of PTC (12 –14). In each case, we evaluated three HPF (400 ×). The images were acquired by the LEICA DFC400 (Leica Microsystem, Herbrugg, Switzerland), and the data was elaborated by the software LEICA LAS (Leica Microsystem). We considered the above-mentioned parameters, whose presence is necessary and sufficient for the diagnosis of PTC, and they are, thus, the most reliable among the quantifiable cytological features of PTC (Fig. 1).

Evaluation in one randomly selected FVPTC case in high power field (40 ×) of the four selected pathological features of PTC (
Microdissection and DNA extraction
Serial 5-μm sections were taken from paraffin blocks for histological examination on glass slides and for DNA extraction on membrane slides (Nikon, Firenze, Italy). The presence of the tumor tissue was confirmed in the first and the last section for each section series. Unstained sections were deparaffinized with Bio-Clear (Bio-optica, Milano, Italy), rehydrated in graded ethanol, and then stained with hematoxylin and eosin. Microdissections were performed using the laser-assisted SL microcut Microtest (MMI GmbH distributed by Nikon). For each sample, 3 to 5 microareas of 5-μm were obtained. Each area contained 200–500 cells. The micro dissected cells were placed in the SL microcut transfer film (Nikon), and the DNA was extracted overnight in a humidified chamber at 56°C in 200 μL of tissue lysis buffer (ATL DNeasy Tissue kit; Qiagen GmbH, Hilden, Germany), containing 20 μL of proteinase K. The DNA was isolated by Qiagen spin column, and carrier tRNA was added to improve recovery of the DNA. Finally, the DNA was eluted in 40 μL of Tris EDTA (TE) buffer and immediately processed for polymerase chain reaction (PCR) amplification. A mock control in which no tissue was added was processed in parallel with each sample.
Detection of the BRAF mutation by PCR-single strand conformation polymorphism and direct DNA sequencing
PCR-single strand conformation polymorphism (SSCP) screening of BRAF mutations was performed by amplifying exon 15 according to a standard procedure. The DNA was used as a template in a 20 μL PCR mixture containing 10 mM Tris-HCl, 50 mM KCl, 1.5 mM MgCl2 (pH 8.3), 0.2 mM dNTPs, 8 pmol of primers, and 1.25U of AmpliTaq Gold DNA Polymerase (Applied Biosystems, Foster City, CA). The PCR primers for the BRAF exon 15 were as follows: 5′ (F)-TCCTTTACTTACTACACCTCAGAT-3′ and 5′ (R)-AGTGGAAAAATAGCCTCAAT-3′. The amplicon size was 167 bp. The cycling conditions were as follows: an initial denaturation (94°C, 5 minutes), followed by 35 cycles (denaturation, 94°C for 40 seconds; annealing, 55°C for 40 seconds; synthesis, 72°C for 40 seconds), and followed by a final extension of 5 minutes at 72°C. All of the PCR products were visualized by electrophoresis in a 2% agarose gel and purified using a PCR purification kit (Qiagen, Crawley, West Sussex, United Kingdom). The purified products were then diluted 1:1 with a denaturing solution (1% xylene cyanol, 1% bromophenol blue, 0.1 mM EDTA, and 99% formamide), boiled for 5 minutes, and then immediately placed on ice to prevent the annealing of single-strand products. The SSCP screening was carried out on the GenePhor Electrophoresis Unit using GeneGel Excel 12.5/24 (12.5% T, 2% C), according to the manufacturer's instructions (GE Healthcare, Milano, Italy). Electrophoresis (600V, 25 mA, 15 W) was performed at 18°C for 100 minutes. The gels were stained with the PlusOne Silver Staining Kit (GE Healthcare), according to the manufacturer's instructions. Altered migration patterns in two or three independent PCR-SSCP runs were indicative of DNA mutations. The purified PCR products were then sequenced by an ALF II automated sequencer (GE Healthcare) using the Thermo-Sequenase-Cy5 Dye Terminator Cycle Sequencing Kit (GE Healthcare). The DNA sequences were compared with those of the normal BRAF gene exon 15 by using the Basic Alignment Search Tool software available at the National Centre for Biotechnology Information. As a control, two human thyroid cancer cell lines, ARO and TPC, that are heterozygous and negative for the BRAF mutation, respectively, were used.
Statistical analysis
The statistical analysis was performed with nonparametric tests by means of PASW statistics 18.0 software (SPSS, Chicago, IL).
The kind of statistical analysis was established after the Shapiro-Wilk test and the Kolmogorov-Smirnov test adopted to verify the null hypothesis that the distributions are normal. This preliminary study influenced our choice to perform nonparametric tests.
The introductive phase was concluded with a statistical power analysis to estimate the sample size required to accept the outcomes of the tests.
In a first step of the analysis (Fig. 2), we used the Kruskal–Wallis test to evaluate the relation between the BRAF status and the FNA classes (Thy1–5). BRAF status was considered the “dependent variable” and Thy was identified as “variable of group.” We opted for the Kruskal–Wallis test, because the data are unpaired and the sample groups are independent.
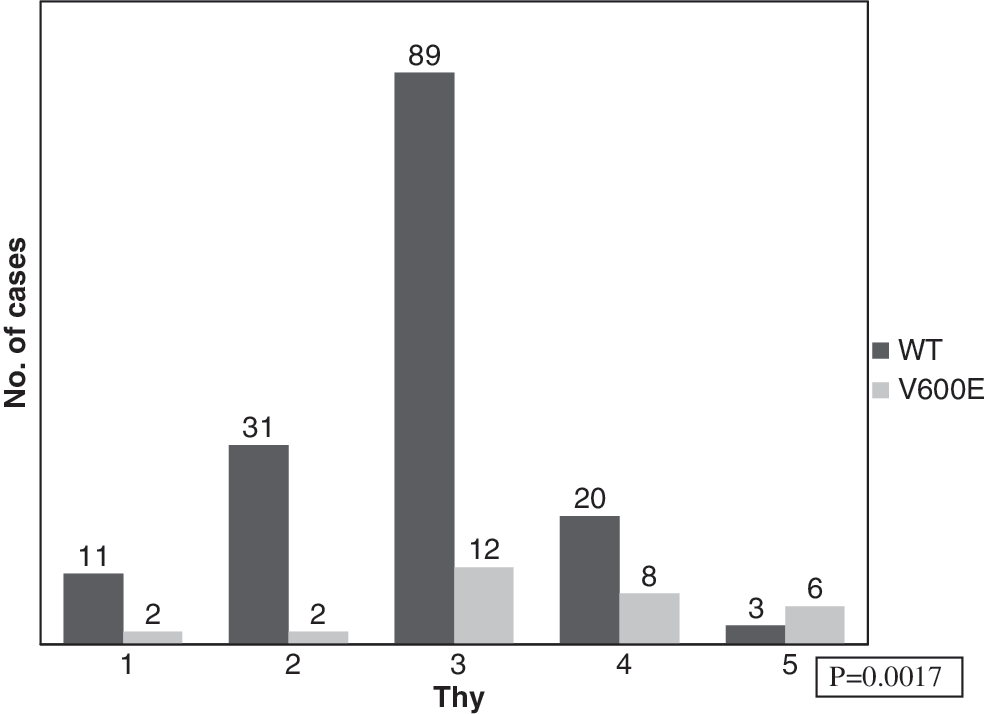
Correlation between BRAF status and fine-needle aspiration classes (Thy) of 187 FVPTC analyzed cases, with comparison between classes. FVPTC, follicular variant of papillary thyroid carcinoma.
In a second phase (Fig. 3), we still adopted the Kruskal–Wallis test to investigate the association between four selected features of PTC (number of cell, grooves, ICI, and mean nuclear diameter) and the FNA classes.

Correlation between preoperative fine-needle aspiration diagnosis and four selected pathological features of PTC evaluated on tissue samples (grooves, intranuclear cytoplasmatic inclusions (ICI), number of cells per high power field, and mean nuclear diameter).
Then, we studied the same pathological features of PTC, considering the influence of the BRAF status; the conditions induced us to use the Mann–Whitney test, because we focused just on two groups (V600E and WT) (data not shown).
With the aim to know the relation between the BRAF mutation and the clinico-pathological parameters described in Table 2 (age, gender, tumor size, histologic growth pattern, extrathyroidal extention, and lymph node metastases), we employed the chi-squared test with the Yates' correction for continuity.
Results
Clinico-pathological parameters of 187 cases of PTC
All of the 187 cases of FVPTC were included after a histological re-review by three experienced pathologists. As reported in Table 1, the mean age for all of the cases was 44.7 years (range 14–79). Among those, 91 patients were over 45 years old at the time of diagnosis, and 148 out of 187 patients (79.1%) were women. The median tumor size was 2.0 cm (range 0.4–6.5) with 110 tumors smaller than 2 cm, 62 tumors ranging from 2 to 4 cm, and 15 tumors larger than 4 cm. More than half (123 of 187, 66%) of FVPTC were encapsulated; the remaining 64 cases had an infiltrative growth pattern, and 19 had a focal extra thyroidal extension. Only 7 cases had lymph node metastases at diagnosis, and no distant metastases were observed. As reported in the same table, only 16.6% of the cases were BRAF-mutated, specifically, 30 cases showed V600E alterations, and in 1 case there was a K601E mutation.
FVPTC with infiltrative growth pattern.
FVPTC, follicular variant of papillary thyroid carcinoma.
Correlation between BRAF status and clinico-pathological parameters
There was no association found between the 31 cases with BRAF mutations and the clinico-pathological parameters (Table 2). Interestingly, 3 out of the 19 cases with extra thyroidal extension were BRAF-mutated.
2 × 2 χ 2 test calculated by STATISTICA software.
ns as p-value >0.05.
FVPTC with infiltrative growth pattern.
Correlation between preoperative FNA diagnosis and clinico-pathological parameters in 187 histologically diagnosed FVPTC
As reported in the Materials and Methods section, all of the 187 cases were preoperatively diagnosed by FNA. As reported in Table 3, >50% (109 out of 187) of the cases were diagnosed as follicular lesions; whereas 43 of those were follicular lesions with atypia. No significant differences were found regarding the mean size of the carcinoma, ranging from 1.4 to 2.6 cm. Interestingly, 86 out of 109 (78.9%) cases of Thy3 lesions were encapsulated carcinomas at the final histological diagnosis; whereas more than half of both the suspicious lesions, Thy4 and Thy5, FNA diagnoses were histologically diagnosed as FVPTC with an infiltrative growth pattern. The same histological feature was observed in 16 nondiagnostic cases (Thy1) and in 9 cases of the benign group (Thy2).
It represents the tumors that were surrounded by a complete capsule.
It represents the tumors with lymph-node metastases at the time of surgery.
FNA, fine-needle aspiration.
Correlation between preoperative FNA diagnosis and BRAF status in 187 histological diagnosed FVPTC
All of the 187 FVPTC tissue samples were evaluated for BRAF status to clarify the possible diagnostic role of BRAF in these type of tumors. As reported in Table 4, 12.1% of follicular lesions (Thy3) and 9.3% of follicular lesions with atypia (Thy3) were BRAF-mutated. Nineteen cases were reported as benign by cytopathologists but resulted in FVPTC at final tissue diagnosis; and among these, only 1 case showed BRAF alterations. As expected, 54.5% and 27.6% of Thy5 and Thy4, respectively, were BRAF-mutated.

As stated in Figure 1, the correlation of the BRAF status and cytological classes was statistically significant (p = 0.0017). In particular, we found that the V600E BRAF mutation was more frequent in the Thy4 and Thy5 classes. In the group of mutated cases, there was a statistically significant correlation (p < 0.05) between the Thy1, Thy2, Thy3, and Thy4 cases against the Thy5.
Correlation between preoperative FNA diagnosis and four selected pathological features of PTC (grooves, ICI, number of cells per HPF, and mean nuclear diameter)
To relate the cyto-nuclear features of PTC at histology and the cytological diagnosis, we evaluated the presence of grooves, the number of ICI, the mean nuclear diameter, and the number of cells per HPF, in 68 FVPTC cases and reported to the cytological Thy diagnosis in Figure 2. No significant differences were found regarding the number of cells, the number of grooves, and the mean cell diameters in the Thy1, Thy2, Thy3, and Thy4 cases. Only the numbers of ICI were statistically associated with the Thy5 cytological class.
Correlation between BRAF status and 4 selected pathological features of PTC (grooves, ICI, number of cells per HPF, and mean nuclear diameter)
To evaluate whether the BRAF mutation is associated with typical cyto-nuclear alterations, the presence of grooves, the number of ICI, the mean nuclear diameter, and the number of cells per HPF were analyzed. No significant differences (p > 0.005) were found between the selected pathological features and the presence of a BRAF mutation (data not shown).
Discussion
FVPTC is one of the most common variants of PTC (9%–25% of patients with PTC) (14). Nevertheless, there is still some difficulty and controversy in the diagnosis of this tumor. Several attempts, either morphologically or at the molecular level, have been performed to clarify this (15).
In 2004, 10 expert thyroid pathologists evaluated 87 histological cases of FVPTC selected from the Mayo Clinic files. A concordant diagnosis for all of them was made with a cumulative frequency of 39% (16). In this series, 24.1% of the patients had metastatic disease. In these cases, a diagnosis of FVPTC was made by all 10 of the reviewers with a cumulative frequency of 66.7%. These results suggest that although the diagnosis of FVPTC is variable, even among experienced thyroid pathologists, most reviewers agreed on this diagnosis for the patients with metastatic disease. The use of well-defined histopathological features should improve the consistency of diagnosing of FVPTC. Since most cases with metastatic disease had obvious invasion, caution should be taken while making a diagnosis of FVPTC in the absence of the major histopathological features or clear-cut invasive growth. It is also well established that distinguishing FVPTC from follicular adenoma and follicular carcinoma might be difficult if nuclear features of papillary carcinoma are not well developed or are only focally present. More recently (17), another analysis was done by a six thyroid expert committee of 15 cases for which original pathology reading was FVPTC. There was unanimous expert agreement in only two cases (13%) and a majority agreement in six cases (40%). Intra-observer agreement ranged from 17% to 100%. This group stated that the histological features which were most helpful in diagnosing FVPTC were nuclear clearing, nuclear grooves, nuclear overlapping and crowding, nuclear membrane irregularity, and nuclear enlargement. The diagnosis of FVPTC is also complex for prospective cytological analysis. We evaluated 187 cases that were read by all our three pathologists and eliminated 29 of the cases, because at least one of the three disagreed with the other two pathologists.
It is well known that FNA is a technique which is used in the diagnosis and management of thyroid nodules. Although the role of this technique in the evaluation of PTC and follicular neoplasms is well established, its value for the diagnosis of FVPTC is controversial. Separation of the noncancerous lesions from the cancerous ones is often very hard, if not impossible. Among the reasons for these difficulties are the following: (a) colloid may be abundant or scant in both lesions; (b) the microfollicular pattern may be encountered in benign adenomatous goiters as well as in follicular neoplasms; (c) the nuclear alterations, typical of a classical variant of PTC, may be, at least in some cases of FVPTC, subtle and present in only a small number of cells, and thus may not be clearly appreciated. For example, ICI that are considered the most specific diagnostic features of PTC are only rarely seen (18).
Several reports have analyzed the sensitivity of FNA, specifically for the diagnosis of FVPTC. In most of the studies reported, the sensitivity ranged from 25% to 55% (19), although Tielens et al. (20) found a surprising sensitivity of 75%. However, the authors included suspicious FNA results in the true-positive category, leading to an apparent increase in the calculated sensitivity.
Recently, we reported that in 505 patients with thyroid nodules who underwent thyroidectomy after a cytological diagnosis of follicular and Hurtle cell neoplasia, 25% of them were carcinomas (9); and as expected, most of them were the FVPTC. Interestingly, when a preoperative cytological diagnosis of the follicular lesions was divided into two groups, without atypia and with atypia, 20% and 45% of carcinomas were found at the histology level, respectively. However, when the follicular-derived neoplasms, with focal nuclear features indicative of PTC, were analyzed as a single category, the malignancy rate increased up to 72% (86/120) (21). In only 11 out of 187 cases, cytopathologists made a diagnosis of malignancy, whereas suspicious carcinomas were reported in 29 cases. In the majority of the cases, the cytological diagnosis was follicular lesion. Our analysis also suggests that a cytological diagnosis of FVPTC is a gray zone, and other methodologies should be applied to better differentiate this extensive group.
All of the previous reports indicate that, from a histological point of view as well as a cytological one, the diagnosis of FVPTC and follicular adenoma is, at least in some cases, very difficult for experienced pathologists. For these reasons, in the last few years, many groups have attempted to evaluate whether the use of other techniques, such as those with a molecular approach, may help in diagnosis. Many studies have revealed that thyroid carcinomas commonly have one of the three genetic alterations: RET/PTC rearrangements, RAS point mutations, and BRAF point mutations.
Although it is well known that the BRAF mutation represents the most oncogenic event in sporadic PTC, there are significant discrepancies regarding the overall frequency of the BRAF mutations in PTC (29%–83%) (22). In a number of studies in which the histotype variant was reported, the BRAF mutation was strongly associated with papillary morphology; and hence, in papillary tumors with a follicular pattern, the alterations of the same gene were significantly lower (8,23). This phenomenon may be due, as hypothesized by Costa et al. (24), to the fact that the BRAF mutations are present with a frequency lower than the threshold of detection of the commonly used mutation scanning techniques. However in our study, we found the V600E BRAF mutation in 16.6% of the cases we analyzed, suggesting that this type of genetic alteration is not a common event in FVPTC. Moreover, we observed a direct association between the BRAF-mutated cases observed in the histopathology section and in the presurgical FNA classes. The FNA cases, diagnosed as suspicious PTC (Thy4) or PTC (Thy5), that had an infiltrative growth pattern in 55.2% and 27.8% of cases, showed the BRAF mutations in 27.6% and 54.5%, respectively; and there was a significant statistical difference, in the group of mutated cases, between the true neoplastic classes (Thy5) and the other four categories (Thy1, Thy2, Thy3, and Thy4). The follicular lesions diagnosed with or without atypia had the BRAF mutation in only 11% of the corresponding FVPTC cases. These data demonstrate that the evaluation of BRAF in the follicular lesion is a rare event and that its analysis cannot be considered the gold standard in the diagnostic process of FVPTC, as the large number of V600E mutated cases were previously diagnosed as PTC by cytology. In the wider group of indeterminate cases (Thy3), searching for a BRAF mutation is not sufficient to rule out PTC. In fact, as recently reported by Nikiforov et al. (25), the accuracy of FNA, in particular, in thyroid nodules with indeterminate cytology, can be enhanced by a molecular testing, not by testing one gene alone but by testing a panel of genes (BRAF, H-RAS, N-RAS, K-RAS, RET/PTC, PAX8/PPAR9γ, and CXCR4) that are involved in the thyroid cancerogenesis. Indeed, the authors demonstrated that the presence of any mutation was a strong indicator of cancer, as 97% of mutation-positive nodules had a malignant diagnosis after surgery.
In conclusion, we found that BRAF is mutated in a low percentage of cases of FVPTC. The presence of positive BRAF mutation status alone is not predictive of a worse prognosis in FVPTC, as is largely considered to be the case for other variants of PTC (8,22). There needs to be a focus on particular morphological criteria and a wider molecular analysis. This can be microarray analysis as suggested by Nikiforova et al. (26) to correctly diagnose PTC. This analysis should be performed in cytological samples, but it cannot be the only guide to the therapeutic management of indeterminate and nondiagnostic findings.
Footnotes
Disclosure Statement
The authors declare no conflict of interest.