
Abstract

Multiple intrathyroidal lymphoepithelial cysts with histopathological features identical to those of branchial cleft cysts have been reported in the thyroid gland (1). Although the histogenesis of intrathyroidal lymphoepithelial cysts remains unclear, an origin from cystically degenerated ultimobranchial body remnants (solid cell nest) seems most probable (2). Lymphoepithelial cysts of the thyroid gland are rare lesions, with only 17 patients described in the medical literature, including 4 patients with bilateral involvement. Here we present a patient with bilateral multiple lymphoepithelial cysts of the thyroid accompanied by Hashimoto's thyroiditis, which is rare phenomenon.
A 49-year-old man who had noticed a huge anterior neck mass for the past year was referred to our department without associated pain, voice change, or obstructive symptoms. The hard, fixed, and nontender goiter was large enough to occupy his whole anterior neck and it had a smooth-surfaced cystic nodule in the isthmic portion of the thyroid gland. The results of thyroid function tests at the time of presentation were within the normal range. Fine-needle aspiration biopsy showed scattered sheets of follicular epithelial cells, many acute inflammatory cells, and histiocytes. An I-123 scintigram displayed homogenous, decreased uptake in the thyroid area. Ultrasonography revealed diffuse, markedly enlarged thyroid glands and an approximately 3 × 4.5 cm mixed echoic lesion with fluid–fluid level visible in the isthmic portion (Fig. 1). On computerized tomography images, a diffuse, enlarged thyroid gland with heterogenous enhancement extended from the carotid bifurcation to the clavicle level. The discrete, smooth-walled, homogenous, hypodense cystic lesions were surrounded by rim enhancement in the isthmus and left lobe, 3 × 2 cm and 2 × 2 cm, respectively. In the right upper lobe, a 1 × 1.5 cm similar hypodense lesion was also identified. Other smaller cysts, two 0.5 × 0.5 cm and 1 × 1 cm, were also seen in the central region and lower pole of the left and right thyroid glands, respectively (Fig. 2). A subtotal thyroidectomy leaving a small portion, which was about 5 g of the right lobe, was subsequently performed. Grossly, the right lobe measured 10 × 8 × 4.5 cm, and the thyroidal parenchyma showed a diffuse multiple nodular appearance and multilocular cyst. Measurement on the isthmus was 2.5 × 2.3 cm, with the cut surface showing a unilocular cyst containing reddish hemorrhagic material. The left lobe measured 11.0 × 5.0 × 3.0 cm, and was identical to the right lobe (Fig. 3). Microscopically, these cysts had a squamous epithelial lining with abundant underlying lymphoid tissue, including lymphoid aggregation with large reactive germinal centers. The remaining thyroid parenchyma showed marked atrophy, oxyphilic change, and diffuse infiltration of lymphocytes and plasma cells with follicle formation characteristic of Hashimoto's thyroiditis. In addition, there were several well-defined solid cell nests lined by squamous cells, which represent ultimobranchial bodies. On immunohistochemistry, the squamous epithelium lining cysts and solid cell nests showed a positive staining for high molecular cytokeratin (Fig. 4). During the routine follow-up, 4 months after surgery, the patient complained of general weakness, hair loss, and hoarseness. On laryngoscopic examination, diffuse true vocal cord swelling was identified. The results of thyroid function tests were consistent with hypothyroidism. After thyroid hormone replacement therapy, the patient's symptoms and vocal cord swelling disappeared and there was no recurrence during the 3 years of follow-up.

I-123 scintigram displays homogenous and decreased uptake in the thyroid area (
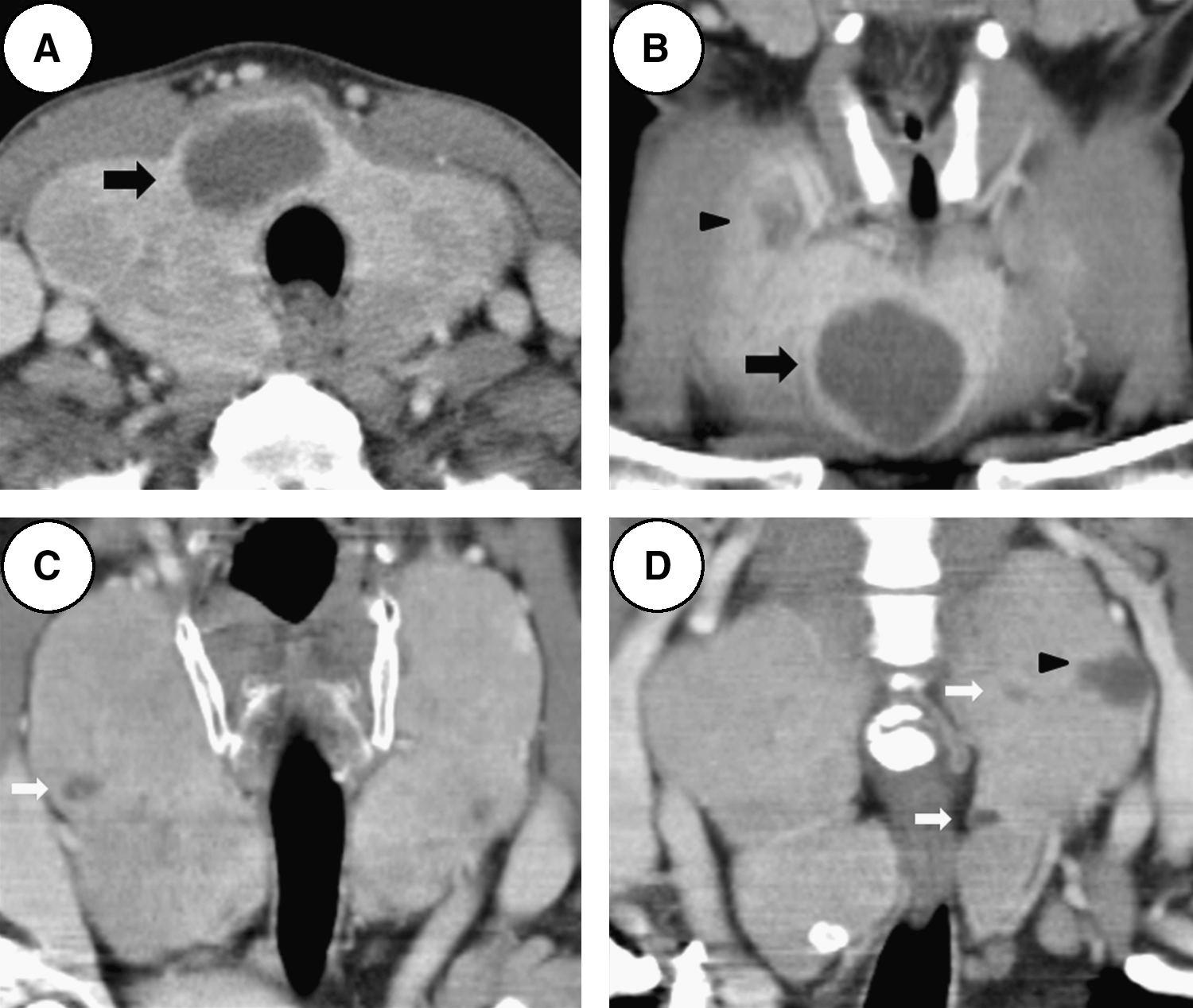
Axial (

Photographs show right (
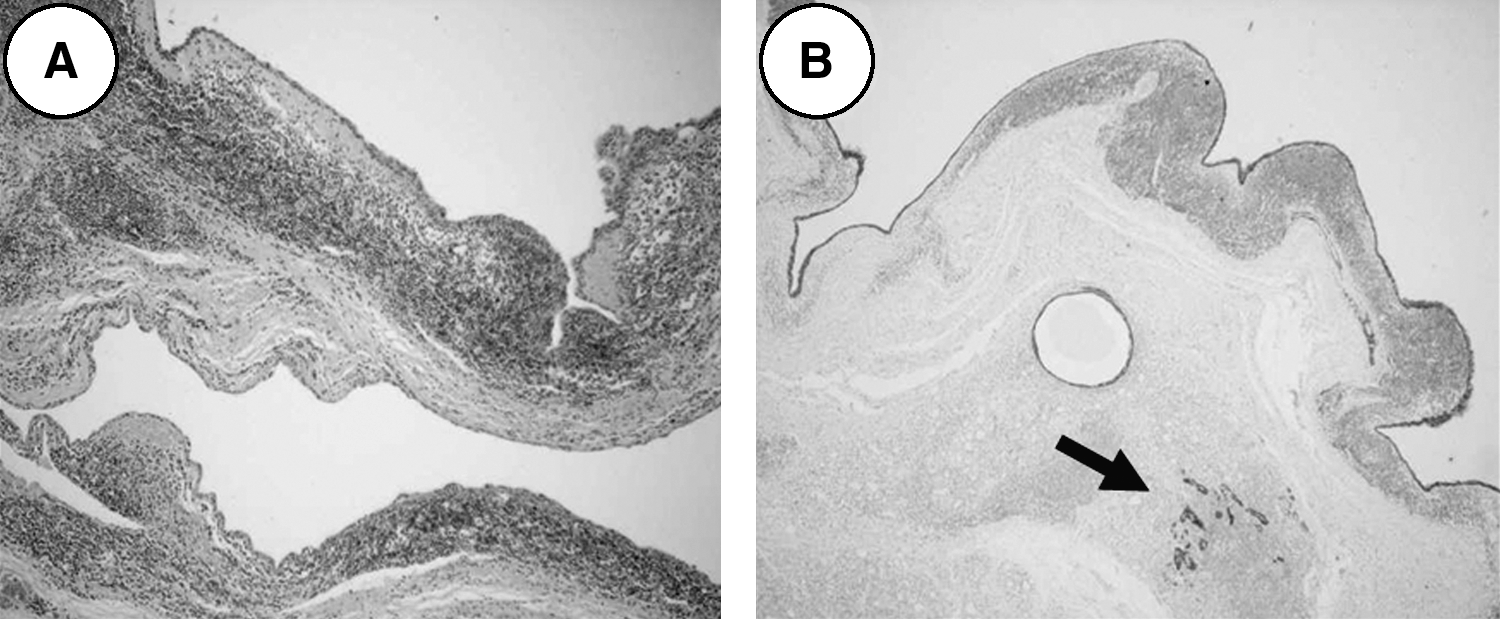
The cyst has squamous epithelial lining with abundant underlying lymphoid tissue, including lymphoid aggregation with large reactive germinal centers (hematoxylin and eosin stain; original magnification, × 100) (
Lymphoepithelial cysts in the thyroid gland are rare and generally assumed to originate from branchial cleft remnants, despite a lack of any direct proof supporting this hypothesis (2). The embryological development of the thyroid gland may explain the presence of intrathyroidal lymphoepithelial cysts. The ultimobranchial bodies give rise to C cells and may contribute to the formation of follicles. Solid cell nests, which have been postulated to be the origin of the lymphoepithelial cysts, also are believed to be of ultimobranchial origin. The lymphoepithelial cysts associated with Hashimoto's thyroiditis were seen in 3 of the previously published 17 cases and in this patient as well. Chronic lymphocytic thyroiditis and varying degrees of chronic inflammation in the thyroid tissue were also identified in the remaining cases. Therefore, development of these cystic lesions may be associated with the chronic inflammation and inflammatory mediators (1). Only 4 of the previously described 17 patient showed bilateral thyroid gland involvement, as in the current patient. Although the pathogenesis of bilateral involvement is unknown, the presence of bilateral lymphoepithelial cysts may support the hypothesis that these lesions originate from ultimobranchial body remnants rather than from thymic or thyroglossal duct remnant because of their midline location in the body. The clinical impact of bilateral involvement as opposed to unilateral cysts might be greater perioperative morbidity and postoperative hypothyroidism due to the necessity of subtotal or total thyroidectomy. There does not seem to be a propensity for malignant changes to occur in unilateral or bilateral lymphoepithelial cysts or for there to be associated thyroid cancer (1). Therefore, radical surgery is not necessary even in bilateral involvement. As the number of reports with multiple intrathyroidal lymphoepithelial cysts is small, the characteristics of this disease have not yet been clarified and preoperative diagnosis is still difficult. As far as the treatment is concerned, it is sufficient to remove the cyst completely. Histologically, attenuated squamous-lined cysts containing dense lymphoid follicles infiltrating within their walls and the solid cell nests are characteristic. Positive immunohistochemical staining of the lining of the squamous epithelium and solid cell nest for cytokeratin and carcinoembryonic antigen are also helpful (3). When we find multiple cystic lesions in the thyroid gland, it is necessary to make an effort to differentiate lymphoepithelial cysts from other common cystic lesions. Postoperative careful monitoring for hypothyroidism is also mandatory, especially with bilateral involvement accompanied by Hashimoto's thyroiditis.