
Abstract

We read with interest the report of Lee et al. (1) concerning their patient with soft tissue implantation of thyroid tissue after endoscopic thyroid surgery. We recently saw a patient with subcutaneous implantation of a benign adenomatous goiter of the thyroid after endoscopic surgery. A 22-year-old woman was referred to our hospital with a thyroid nodule. The ultrasound showed a 4 × 3 cm nodule in the right lobe of the thyroid. The results of a fine-needle aspiration biopsy (FNAB) of the nodule supported the diagnosis of an adenomatous goiter. The patient received TSH suppression therapy with 100 μg of L-thyroxine per day for 1 year. However, the size of the nodule did not change. The patient was referred to another hospital for endoscopic surgery, and an endoscopic right hemithyroidectomy, by the breast approach, was performed at that hospital (Fig. 1). The histopathology of the surgical specimen supported the diagnosis of an adenomatous goiter of the thyroid. During regular follow-up at our hospital, multiple palpable subcutaneous nodules developed in the left anterior neck and the anterior chest, within 2 years after the endoscopic surgery. The ultrasound and computed tomography findings showed a subcutaneous nodule in the left lower neck, two subcutaneous nodules in the left upper chest wall, and two small nodules in the right breast (Figs. 1 and 2). The locations of these nodules were thought to be along the tracks of the trocars inserted during the previous endoscopic surgery. FNAB of these nodules showed that they were all benign thyroid adenomatous goiters; they had the same histological features as the previously removed thyroid nodule (Fig. 3). These nodules were likely subcutaneous implants from the thyroid adenomatous goiter that occurred after the endoscopic thyroidectomy. We performed molecular and immunohistochemical analyses of the original nodule to exclude differentiated thyroid cancer. Mutational analyses for BRAFV600E and codons 12, 13, and 61 for K-RAS were negative. The expression of galectin-3 and cyclin D1 were negative, but the expression of HBME-1 and CK19 were positive (data not shown). Based on the results of these analyses, we could not find any evidence that the nodule was malignant. The patient is currently followed under close observation without any specific management, and the subcutaneous nodules are stable.
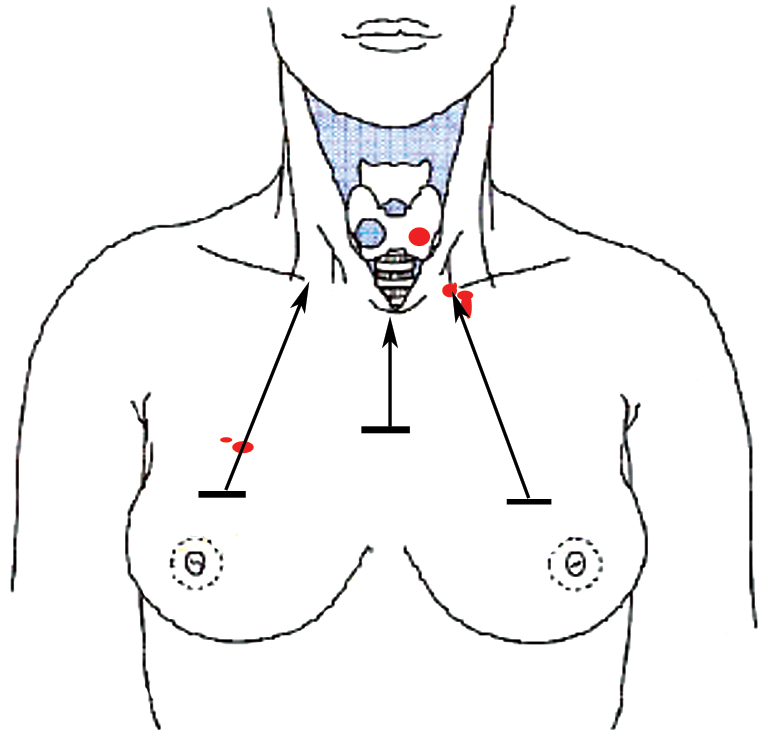
Breast approach for the endoscopic hemithyroidectomy (arrows) and the locations of the subcutaneous nodules. Color images available online at
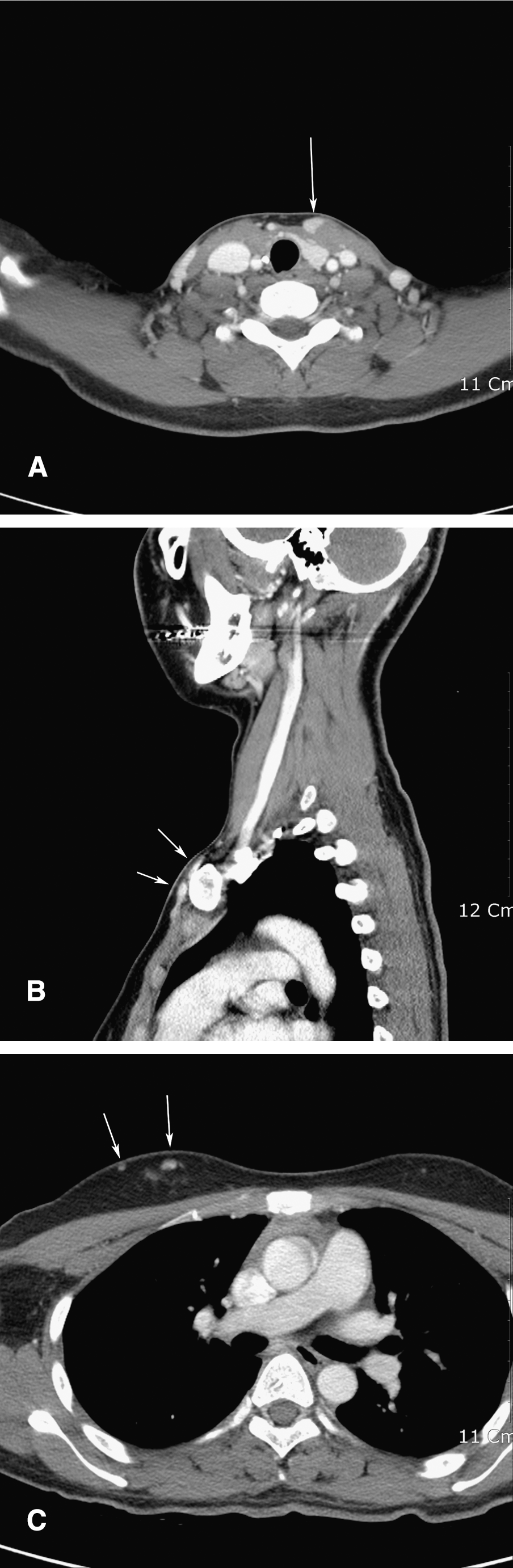
Computed tomography showing subcutaneous nodules (arrows) in the left lower neck (
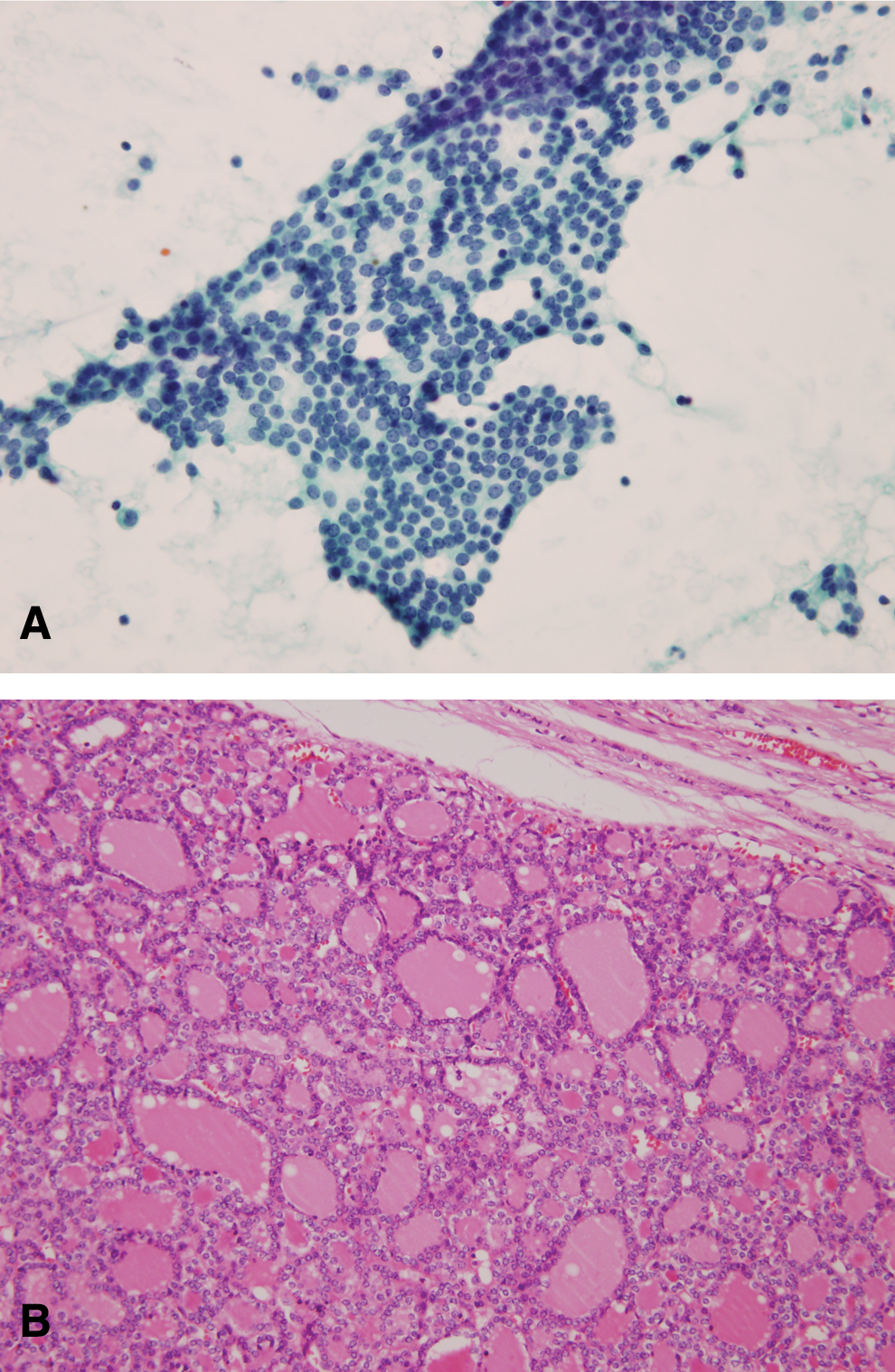
The aspirates from the subcutaneous nodule showing flat sheets of uniform follicular cells (
Needle tract implantation of thyroid cancer after FNAB is rare but a well-established occurrence (2). However, the soft tissue implantation of benign thyroid tissue is very rare. Moses et al. reported ectopic thyroid tissue in the neck, which developed several years after surgery of nodular colloid goiter (3). Harach et al. reported nine patients with the implantation of thyroid tissue after surgery or trauma (4). In seven of the patients, the nodules were confirmed to be pathologically benign. The rupture of thyroid tissue during surgical manipulation or trauma is presumed to be the cause of such implantations; they occurred within the surgical field and birefringent particles consistent with material derived from the previous operations were found close to the recurrent nodules. Nodular thyroid tissue was cut across in all or the majority of the cases during the original surgery (4).
Port-site tumor implantations following laparoscopic surgery have been reported since the introduction of laparoscopic treatment for malignant disease. Current indications for endoscopic thyroidectomy include the presence of a benign single thyroid nodule less than 4 cm in diameter and a low-risk papillary carcinoma with nodules smaller than 1 cm. Recently, Lee et al. reported a patient with soft tissue implantation of benign thyroid adenomatous hyperplasia after endoscopic thyroid surgery (1). Rupture of the relatively large nodule during surgical manipulation might cause subcutaneous implantation, similar to the patient reported here. Implantation of a benign adenomatous goiter could occur over a 5- to 20-year period after surgery (1,4). However, in our patient, the recurrence of the nodule occurred within a relatively short period, 2 years after surgery.
Currently, the number of patients undergoing endoscopic thyroid surgery is rapidly increasing because of the excellent cosmetic results, more rapid recovery, and reduced tissue trauma. However, it is important to recognize that surgery for a benign thyroid nodule might lead to implantation of thyroid cells, and this complication is not uncommon. Thus, precaution against rupture of a nodule, such as avoiding cutting or morselization of the nodule, should be carefully considered during endoscopic surgery even in patients with a benign thyroid nodule. Packing of the surgical specimen into a bag during retrieval is another preventive measure. The diagnosis should be suspected clinically when soft tissue nodules occur around the surgical field after thyroid surgery for benign lesions.
Disclosure Statement
The authors declare that no competing financial interests exist in connection with submitted manuscript.