
Abstract
Background:
Pregnancy influences thyroid function and may bring to light mild and latent disorders. Thyroid dysfunction has been related to obstetrical complications such as premature delivery, gestational hypertension, preeclampsia, and placental abruption. The aim of our study was to evaluate whether the occurrence and timing of pregnancy loss could be related to thyroid autoimmunity or subclinical hypothyroidism (SH) per se.
Methods:
Two hundred sixteen apparently healthy pregnant women with no previous history of thyroid disease and with diagnosis of early miscarriage (before the 12th week of gestation) were enrolled. Miscarriages were classified as very early pregnancy loss (EPL) or embryo loss (crown rump length ≤10 mm) and EPL or fetal loss (crown rump length > 10 mm). Women were subdivided into four groups: euthyroid (ET), SH, overt hypothyroidism, and thyroid autoimmunity group.
Results:
One hundred seventy-six women had a normal thyroid function (84.6%), 24 patients were found to have positive thyroid antibodies (11.5%), 8 women (3.8%) an SH, and 8 cases were excluded. Thyroid-stimulating hormone levels were found to be higher in the very early (1.4 ± 1.0 mU/L) than in the EPL group (1.1 ± 0.7 mU/L) (p = 0.04), and in patients affected by SH (3.9 ± 0.1 mU/L) compared to ET (1.0 ± 0.5 mU/L) (p < 0.001) and autoimmune women (1.0 ± 0.4 mU/L) (p < 0.001). Although the multivariate logistic regression analysis revealed that both autoimmunity and SH were independently correlated with the onset of very EPL, abortion was more precocious in the SH group (6.5 ± 0.9 weeks), followed by the autoimmune (8.2 ± 2.1 weeks) and ET groups (8.2 ± 1.6 weeks) (p = 0.02).
Conclusions:
Both thyroid diseases SH and autoimmune disorder are independently associated with very early embryo loss, but women suffering from SH have a lower gestational age at abortion.
Introduction
Since pregnancy requires more intensive hormonal production, it influences thyroid function and may bring to light mild and latent disorders (1). Thyroid economy is deeply affected by several changes that occur from very early gestation. These include hormonal and metabolic changes mainly consisting of (i) an estrogen-related increased hepatocyte synthesis of thyroxine binding globulin, (ii) an enhanced renal iodide clearance from plasma and transplacental transfer of iodide, and (iii) thyroid stimulation via a thyrotropin-like action of human chorionic gonadotropin (2,3).
There is evidence that adequate fetal thyroid hormone concentrations are needed from the earliest stages of pregnancy to achieve normal neurodevelopment. Since the fetal thyroid gland becomes fully operative only after midgestation, maternal euthyroidism is vital to ensure the normal psychoneurological development of the fetus (4). Moreover, thyroid dysfunction has been related to obstetrical complications such as premature delivery, gestational hypertension, preeclampsia, and placental abruption (5).
Hypothyroidism is a relatively rare condition in pregnancy (0.3%–0.5%) and is frequently associated with increased infertility. A higher risk of miscarriage seems to be related to subclinical hypothyroidism (SH) and thyroid autoimmunity (TAI), the latter defined by the presence of high levels of thyroglobulin antibody (TGAb) and/or thyroid peroxidase antibody (TPOAb) (6). SH affects approximately 2%–3% pregnant women and may result in infertility and pregnancy wastage; however, the pathogenetic factors involved are unknown (7,8). TAI represents the most common autoimmune disorder, affecting 5%–10% of pregnant women (9).
Several reports have shown that women suffered from thyroid autoimmune disorders have a higher risk of obstetrical complications, including single or recurrent miscarriage (10). However, it has yet to be established whether this risk is related to the presence of circulating thyroid autoantibodies or even to subtle degrees of maternal thyroid insufficiency associated with TAI. On the basis of these considerations, we designed this study to evaluate whether or not the occurrence and timing of early pregnancy loss (EPL) could be related to either of these two factors, namely, TAI or maternal thyroid insufficiency per se.
Materials and Methods
The study was carried out at the Department of Gynecological, Obstetrical Sciences, and Reproductive Medicine of University Hospital of Messina between January 2007 and August 2008 on a sample of women resident in the northeastern Sicily, which had previously been classified as a moderately severe iodine-deficient area (11).
Two hundred sixteen consecutive pregnant women with no previous history of thyroid disease were referred to our department with the diagnosis of early miscarriage (before the 12th week of gestation) (12) were enrolled. Exclusion criteria were multiple miscarriages (more than two), pregnancy obtained by assisted reproduction technologies, extrathyroid autoimmune diseases, chronic hypertension, diabetes mellitus, metabolic disorders, uterine malformations (septate or bicornuate uterus), and uterine fibroids. All patients gave their written informed consent and the study was approved by the Institutional Review Board.
On admission, data regarding demographic and obstetrical characteristics (maternal age, gestational age, parity, and previous miscarriage) were recorded, and all women underwent an ultrasonographic examination to confirm the diagnosis and to exclude the above-reported uterine abnormalities. Effective gestational age was calculated using fetal crown rump length (CRL) and/or the size of the gestational sac. Moreover, the ultrasound evaluation allowed miscarriages to be classified as follows: very EPL (VEPL) or embryo loss (CRL ≤ 10 mm), and EPL or fetal loss (CRL > 10 mm) (12). Before treatment, blood samples were taken from the women for the assay of anti-TPOAb, anti-TGAb, serum thyroid-stimulating hormone (TSH), and free thyroxine (FT4). The pregnant women were subdivided into four groups: the euthyroid (ET) group, which included women with negative antithyroid antibodies and normal values of TSH and FT4 (TSH between 0.4 and 2.5 mU/L; FT4 between 11.9 and 20.8 pm/L); the nonautoimmune SH group, which included those with a TSH > 2.5 mU/L, normal FT4, but with negative antithyroid antibodies; overt hypothyroidism (OH) group (TSH > 2.6 mU/L; FT4 < 11.9 pm/L); and the TAI group, comprising those with positive antithyroid antibodies (TGAb > 115 IU/mL; TPOAb > 34 IU/mL) (13,14). Patients with both conditions, subclinical OH and positive antithyroid antibodies, were excluded to avoid possible bias. It is likely that this class of patients is very limited in our area of study, where the main cause of maternal thyroid failure is represented by iodine deficiency, as previously reported (12).
All maternal serum samples were assayed using chemiluminescent immunoassays on an automated platform (Immulite 2000 Analyzer; Siemens Medical Solution Diagnostic, Los Angeles, CA). The TSH assay had a reported analytic sensitivity of 0.002 milliunits/L, and FT4 had an analytic sensitivity of 0.18 ng/dL. The anti-TG and anti-TPO assay sensitivities were 10 and 5.0 milliunits/L, respectively.
Statistical analysis was performed using the SPSS 13 software package (SPSS Inc., Chicago, IL). Continuous data are reported as mean and standard deviation and analyzed applying a two-way analysis of variance followed by a post hoc Tukey test when required. Skewed data were log-transformed before analysis. Categorical data are reported as percentages, and analyzed using the chi-square test or Fisher's exact test when appropriate. Logistic regression analysis was used to assess the correlations between the variables considered in the study and the diagnosis of VEPL. A p-value < 0.05 was considered to be statistically significant.
Results
Eight (3.7%) out of 216 patients were excluded from our series: in 3 patients (1.4%) a history of multiple miscarriages was recorded; 2 women (0.9%) were affected by uterine myomas, a pregnancy (0.46%) that had been obtained by assisted reproduction technologies; and in the remaining 2 cases septate uterus (0.46%) and chronic hypertension (0.46%) were diagnosed. Thus, the analysis was performed on the remaining 208 cases. The mean maternal age was 34.7 ± 5.3 years, and 132 women (63.5%) were multiparous and 76 (36.5%) had a previous history of miscarriage. The mean gestational age at abortion was 8.1 ± 1.7 weeks: 32 out of 208 pregnancies (15.4%) ended in VEPL, whereas the remaining 176 (84.6%) in EPL. Regarding the endocrinological pattern, 176 women had normal thyroid function (84.6%), 24 patients were found to have positive thyroid antibodies (11.5%), and in 8 cases (3.8%) an SH was found. No case of OH was recorded.
No significant differences were found among the three groups for the demographic and obstetrical characteristics analyzed with the exception of gestational age at miscarriage (Table 1).
Analysis of variance.
ET, euthyroid; TAI, thyroid autoimmunity; SH, subclinical hypothyroidism; GA, gestational age.
The mean overall levels of serum TSH and FT4 were 1.1 ± 0.8 mU/L and 16.9 ± 2.7 pm/L, respectively. Regarding TSH levels in relation to gestational age, a significant difference was found between the VEPL (1.4 ± 1.0 mU/L) and the EPL groups (1.1 ± 0.7 mU/L) (p = 0.04). Moreover, the mean TSH value was 1.0 ± 0.5 mU/L in the ET group, 1.0 ± 0.4 mU/L in the TAI group, and 3.9 ± 0.1 mU/L in the SH group (p < 0.001). A significant difference was found only between the ET and SH groups and between the TAI and the SH groups (p < 0.001). In contrast, no difference was found for serum FT4 levels (ET, 16.8 ± 2.8 pm/L; TAI, 18.1 ± 1.7 pm/L; SH, 16.4 ± 0.6 pm/L; p = 0.09).
The mean gestational age at miscarriage was 8.2 ± 1.6 weeks in the ET group, 8.2 ± 2.1 weeks in the TAI group, and 6.5 ± 0.9 weeks in the SH group (p = 0.02). A significant difference was found between the ET and SH groups (p = 0.016), and between the TAI and SH groups (p = 0.037). No difference was found between the ET and TAI groups (p = 0.99). However, an analysis of the split into VEPL and EPL showed the former group to be composed of 8 patients affected by TAI (25%), 4 by SH (12.5%), and 20 with a normal thyroid function (62.5%), while the latter included 16 cases of TAI (9.1%), 4 of SH (2.3%), and 156 ET women (88.6%) (p < 0.001). The two groups were found to be statistically different with respect to TAI (p = 0.004) and SH (p = 0.002) (Fig. 1). In the VEPL group a significant difference in TSH values was found between SH and TAI (4.1 ± 0.1 vs. 1.0 ± 0.1 mU/L; p < 0.001) and between SH and ET (0.9 ± 0.1 mU/L; p < 0.001), while TAI and ET did not differ (p = 0.68). A similar result was found in EPL (SH, 3.8 ± 0.2 mU/L; TAI, 1.0 ± 0.5 mU/L; ET, 1.0 ± 0.5 mU/L; SH vs. ET, p < 0.001; SH vs. TAI, p < 0.001; TAI vs. ET, p = 0.99).
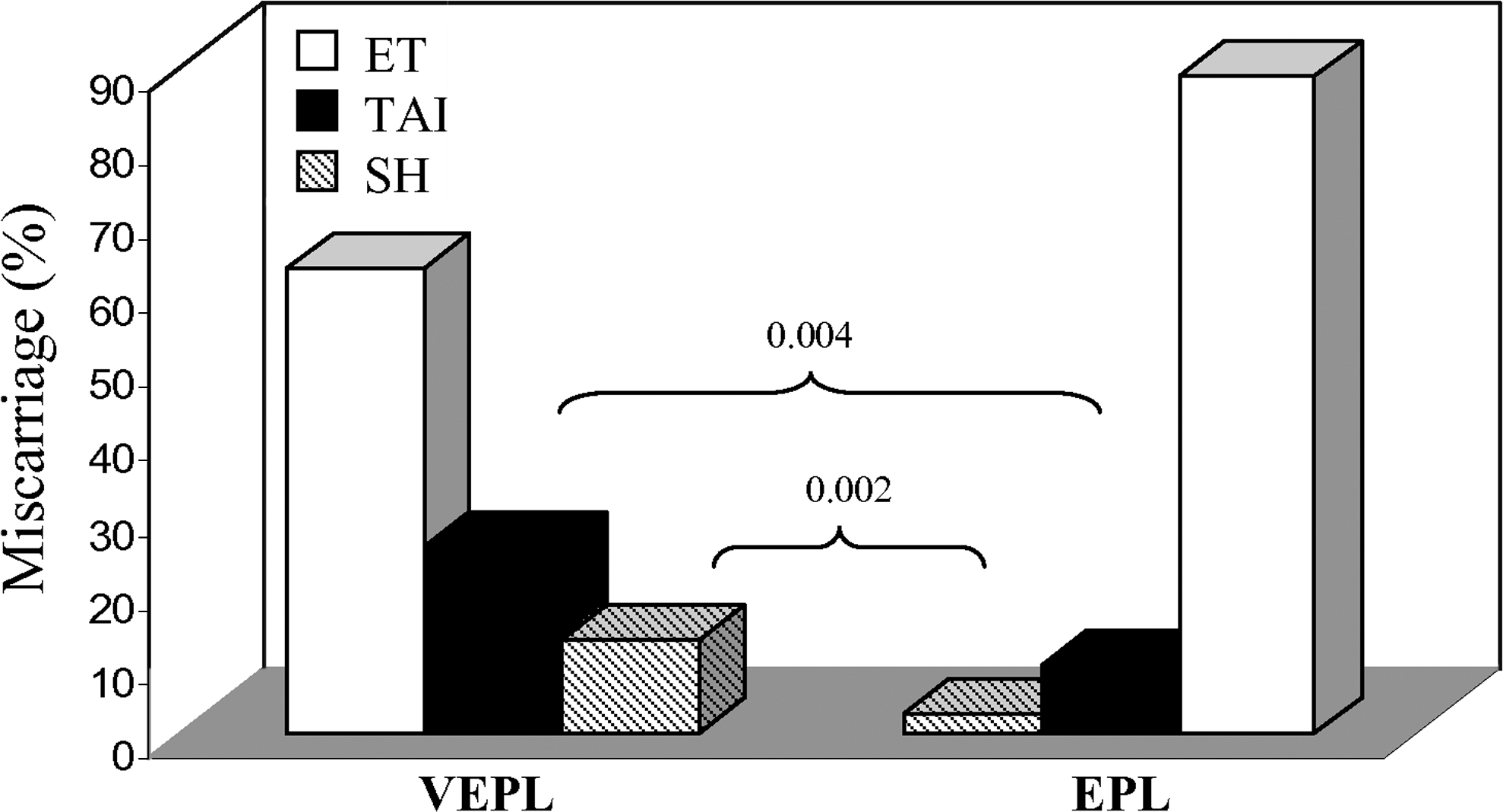
Thyroid function in the two kinds of miscarriage. ET, euthyroid; TAI, thyroid autoimmunity; SH, subclinical hypothyroidism; VEPL, very early pregnancy loss; EPL, early pregnancy loss.
On applying the logistic regression analysis to the variables considered in our sample, VEPL was found to be correlated with the presence of a higher levels of TSH (SH group) (odds ratio [OR], 6.14; 95% confidence interval [CI], 1.45–25.4; p = 0.014) and with the presence of autoantibodies (TAI group) (OR, 3.33; 95% CI, 1.28–8.62; p < 0.013), whereas no significant correlations were found for the remaining variables (Table 2). The multivariate analysis revealed that both variables were independently correlated with the onset of VEPL (TSH level: OR, 7.8; 95% CI, 1.8–33.6; p = 0.006; autoantibodies: OR, 3.9; 95% CI, 1.4–10.2; p = 0.006).
Logistic regression analysis.
OR, odds ratio; CI, confidence interval.
Discussion
Over the past 20 years there has been an increasing interest in the effects of hormonal and metabolic changes of pregnancy on thyroid function in addition to the repercussions of thyroid disorders on the outcome of pregnancy. The aim of our study was to evaluate thyroid function in a wide sample of pregnant women whose pregnancy ended in early abortion. The prevalence of TAI in our series was 11.5%, which is similar to the percentage reported by Negro et al., but slightly higher than that reported in female population by Glinoer et al. (5,15). This finding is probably related to the characteristics of our sample that included exclusively pregnancies complicated by miscarriage. The same consideration may be applied to the prevalence of SH (7). These findings concur with those reported in our previous study, which had also provided evidence for a low relative risk of hypothyroidism in antibody-positive women (16). In our study, no case of OH was recorded, and this may be linked to the low prevalence of this disorder in pregnancy (0.3%–0.5%) (13) since it is frequently associated with ovulatory disorders and consequently with sterility (17). However, the most interesting finding of our study is the association between TSH levels and gestational age at abortion. The SH group was characterized by a lower mean gestational age at abortion compared to the other two groups, whereas no significant difference was found between the TAI and the ET groups. The association between TSH and gestational age at miscarriage was also confirmed by subdividing miscarriages into VEPL and EPL, since higher levels of TSH were found in the former group. These deleterious effects are not directly caused by high serum levels of TSH per se, but likely reflect a reduced capacity of the thyroid to meet the increased demand due to pregnancy. Indeed, maternal thyroid status is important for trophoblast function and to maintain pregnancy since the earliest stages of gestation (18).
Regarding the effects of thyroid antibodies on precociousness of abortion, no significant difference was found in the mean gestational age at miscarriage between autoimmune and ET women. However, the VEPL group was found to contain a higher percentage of Ab-positive patients than the EPL group. It has been reported that patients with recurrent in vitro fertilization (IVF) failure have a higher incidence of TAI also in the presence of a normal thyroid hormonal pattern (19) and that patients with spontaneous conception and who are Ab positive have a higher incidence of miscarriage (5). Our finding not only confirms the high incidence of TAI in women affected by abortion, but also suggests that the presence of autoantibodies may play a role in the early miscarriage. However, the exact mechanism of the association of TAI with miscarriage remains largely unknown. Stagnaro-Green et al. hypothesized that the presence of thyroid autoantibodies may reflect a generalized activation of the immune system and specifically a heightened reactivity of the immune system against the feto-placental unit (20). The presence of thyroid autoantibodies may act as an infertility factor and may delay conception. Thus, when women with thyroid autoantibodies do become pregnant, they are older and face a higher risk of miscarriage (21). However, in the study reported by Poppe et al. (22) and in our study, the mean age of women with thyroid autoantibody did not significantly differ from those negative for TAI. Other authors have reported that the presence of thyroid autoantibodies in ET women could be associated with a subtle deficiency in thyroid hormone concentrations or a lower capacity of the thyroid gland to adequately adapt to the demands of pregnancy. Indeed, the mean serum TSH values, while being within normal range, were significantly higher in thyroid-autoantibody-positive women than in women with negative thyroid autoantibodies. This may reflect lower thyroidal reserve during pregnancy when a greater amount of thyroid hormones is demanded (23). In our study, the mean serum TSH values did not differ between patients with and without thyroid antibodies, and this, as stated above, may be due to the early gestational age of our sample, the low autoantibody titers that indicate early autoimmune disease, and the application of an internal first-trimester-specific reference range for TSH. Patients with high autoantibody titers are more likely to be in an advanced stage of the disease and to develop a condition of hypothyroidism (15). Moreover, it has been reported that in thyroid-autoantibody-positive women, serum TSH levels gradually increased as gestation progressed, with 19% of them having an increased serum TSH at delivery (24).
Conclusions
Women suffering from SH have a lower gestational age at abortion than those affected by autoimmune disease, and this suggests a more important role of TSH, one that better reflects the hormonal capacity of the thyroid. Given these results, it could be useful to perform a preconceptional or a very early screening for thyroid disorders, to evaluate the need for hormonal supplementation. However, since there are only few reports showing that thyroxine treatment may be effective in reducing the number of miscarriages, further studies are required to reach definitive conclusions.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.