
Abstract
Background:
Mycophenolate mofetil is a recently identified therapy for disorders associated with systemic fibrosis, but has never been reported in the treatment of Reidel's thyroiditis. We report the first case of Reidel's thyroiditis that became resectable after treatment with mycophenolate and prednisone.
Summary:
A 27-year-old woman presented to an outside hospital with thyromegaly associated with compressive symptoms. The patient underwent a neck exploration with thyroid biopsy that revealed evidence of fibrosing variant Hashimoto's thyroiditis. The patient was then treated with tamoxifen and prednisone at an outside hospital without resolution. After initial evaluation she underwent an open thyroid wedge biopsy that revealed Reidel's thyroiditis. She was subsequently treated with both 1 g mycophenolate twice daily and 100 mg prednisone daily. The patient experienced immediate subjective improvement of compressive symptoms and objective decrease in mass size at 30 days, as seen by serial computed tomography examination. By 90 days of therapy the mass had decreased to a size small enough to allow subtotal thyroidectomy, which was completed over two staged procedures.
Conclusions:
Reidel's thyroiditis remains a primarily surgical disease. Patients who are not surgical candidates have been treated with tamoxifen and prednisone with equivocal results. Our report is the first to suggest the combination of mycophenolate and prednisone as a viable treatment option for patients with Reidel's thyroiditis.
Introduction
Although the etiology of Reidel's thyroiditis is yet to be fully defined, it is believed to occur as a local manifestation of a generalized fibroinflammatory process triggered by unknown autoimmune stimuli (2). Evidence for this pathogenic mechanism comes from associations between Reidel's thyroiditis and other forms of fibroinflammatory disease [idiopathic retroperitoneal fibrosis, inflammatory pseudotumors, sclerosing cholangitis, and Tolosa–Hunt syndrome (3 –6)]. Additionally, Reidel's thyroiditis may have an immune component as evidenced by reports of antimicrosomal and antithyroglobulin antibodies in some patients with Reidel's thyroiditis (7).
Patient
A 27-year-old woman with a history of migraine headaches and pseudotumor cerebri presented with a 5-month history of an enlarging anterior neck mass associated with progressive dyspnea, dysphagia, and subjective hearing loss. The patient was previously seen at an outside hospital where attempted thyroidectomy was unsuccessful in removing the infiltrative thyroid mass that was found to encase the trachea. Thyroid biopsy at the time of surgery displayed inflammatory fibrosis with no signs of thyroid carcinoma or lymphoma, and the initial diagnosis of Hashimoto's thyroiditis fibrosing variant was made. Treatment with tamoxifen and corticosteroids was subsequently attempted, with no effect on mass size or subjective compressive symptoms.
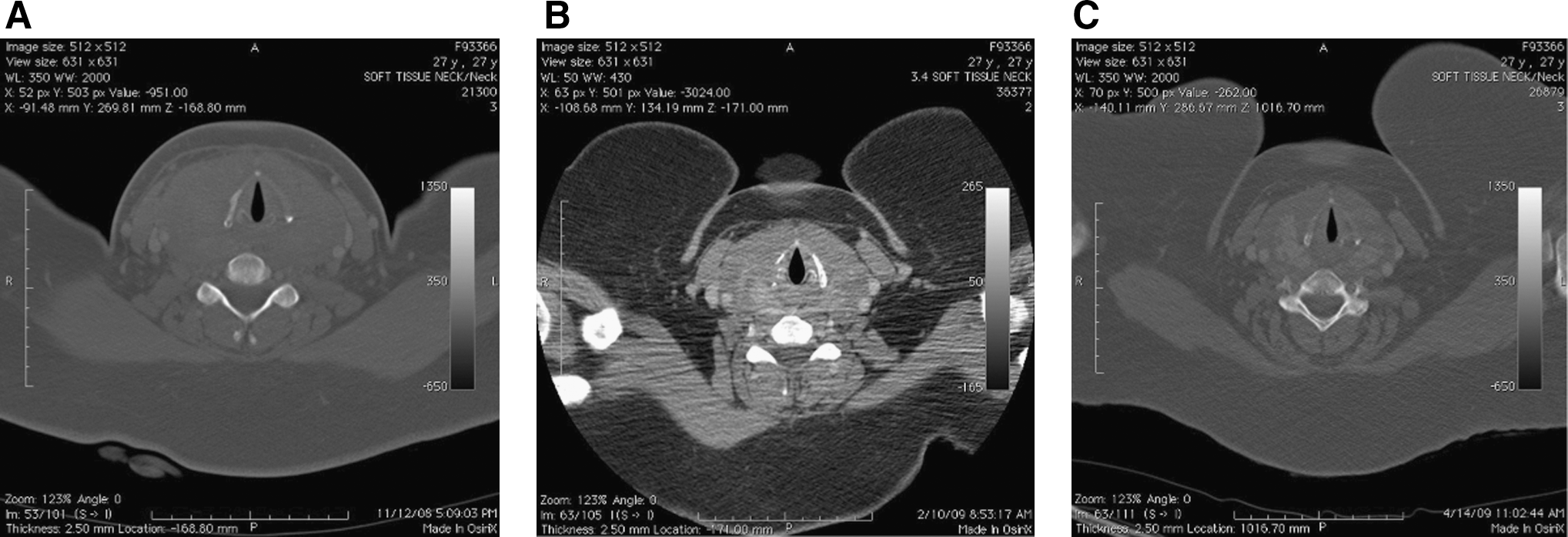
On presentation to our facility, physical examination revealed a warm, hard, enlarged thyroid with uniform consistency involving the entire mid-neck with substernal extension. Flexible direct laryngoscopy revealed mild obliteration of the right piriform sinus without mucosal lesions or other signs of airway obstruction. Computed tomography displayed a diffusely enlarged thyroid measuring 343.9 cm3 with mild homogenous enhancement. The mass laterally displaced the carotid vessels, and posterior extension around the trachea to the esophagus (Fig. 1A). Prior tissue samples were reviewed and repeat wedge biopsy of the thyroid was done to further characterize the ongoing fibrotic process. Pathology showed diffuse inflammatory fibrosis and local invasion consistent with Reidel's thyroiditis (Fig. 2A). In addition, audiometric analysis was completed, displaying an asymmetric sensorineural hearing loss associated with presumed Tolosa–Hunt syndrome. With unsuccessful attempted surgical excision and unsuccessful prior treatment with tamoxifen, it was decided to proceed with a treatment regimen consisting of both mycophenolate mofetil (1 g twice daily) and prednisone (100 mg daily).
(
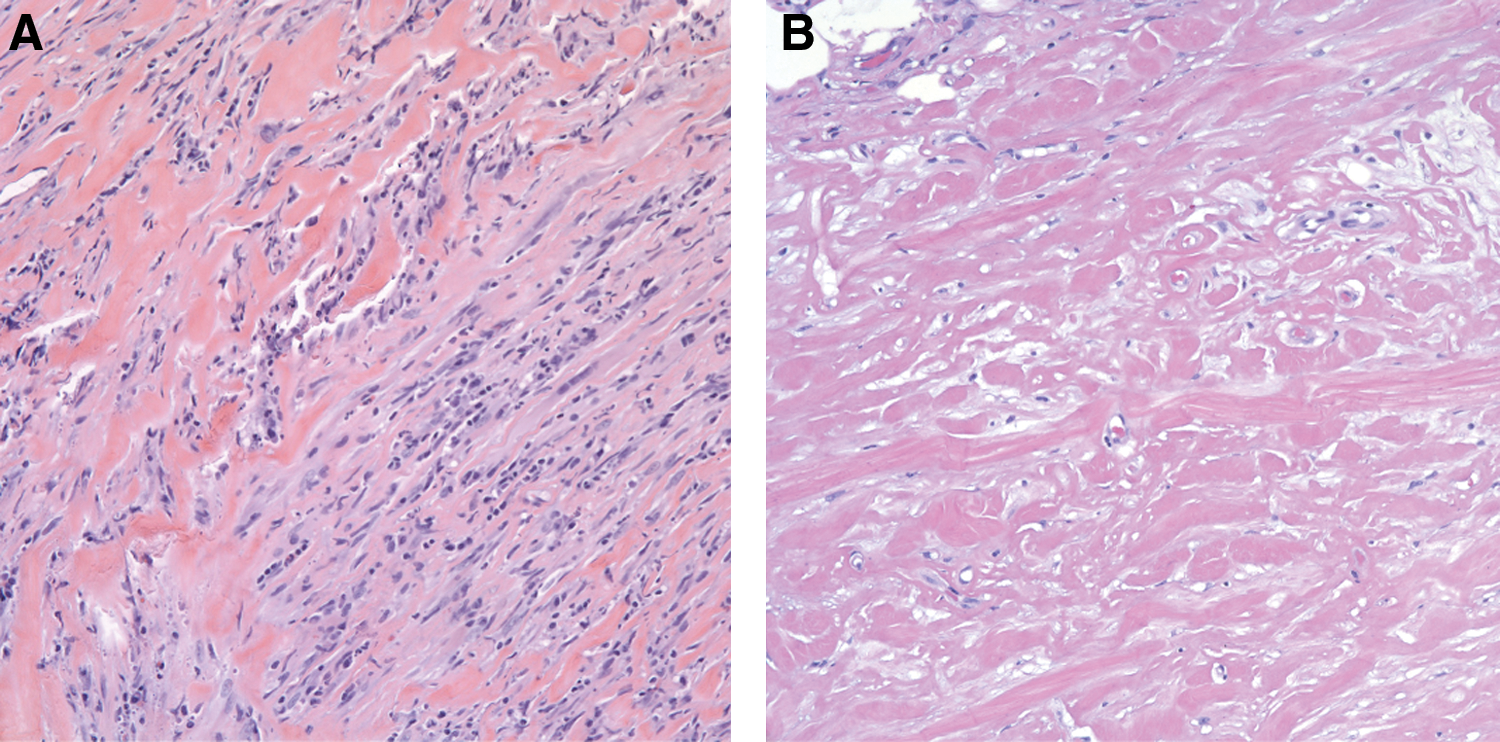
Section of thyroid tissues (hematoxylin & eosin, × 20) before treatment (
The patient experienced improvement in symptoms with subjective reports of mass softening and decreased size. She also reported subjective improvement in hearing at 7 days of therapy and decreased dyspnea and dysphagia at 30 days. Serial computed tomography showed decreasing mass size at both 30 and 90 days, with established protocols for thyroid volumetric analysis (8,9) measuring a mass size of 8.6 × 5.2 cm and 264.9 cm3, respectively, after 1 and 3 months of therapy (Fig. 1B, C), for a total decrease of 79.0 cm3 after 3 months of treatment. Radiographic evaluation revealed persistent bilateral displacement of the great vessels. However, considering the impressive response to the described regimen, a staged subtotal thyroidectomy was attempted with successful excision of the fibrotic thyroid.
Gross examination of the excised tissue revealed a composite 161.2 cm3 mass with complete obliteration of the thyroid architecture. Glandular elements were replaced by hyalinized fibrous tissue with a subtle infiltrate of acute and chronic inflammatory cells including a rare atypical lymphocyte but lacking giant cells (Fig. 2B). The infiltrate was slightly reduced relative to the pretreatment tissue sample, which exhibited a more prominent lymphoplasmacytic infiltrate with occasional histiocytes and neutrophils.
The patient's postoperative course was uneventful with resolution of compressive symptoms. The patient was continued on mycophenolate due to return of her hearing loss presumed secondary to Tolosa–Hunt syndrome. On mycophenolate, her hearing again improved. The patient is currently recovering without residual sequelae of her disease.
Discussion
The primary treatment of Reidel's thyroiditis is surgical resection. Pharmacotherapy including glucocorticoids and tamoxifen is usually aimed at attenuating the fibroinflammatory process in cases where surgical excision is not feasible (10 –13).
Mycophenolate mofetil, an immunomodulatory agent, has recently shown to have success in the treatment of fibrotic disorders in both case series (14 –16) and in vitro models (17,18). These studies have elucidated the anti-fibrotic effects of mycophenolate mofetil in retroperitoneal fibrosis and other idiopathic fibrotic diseases. However, mycophenolate has not previously been reported in the treatment of Reidel's thyroiditis. In this report we describe the first case of Reidel's thyroiditis and Tolosa–Hunt syndrome successfully treated with mycophenolate mofetil and prednisone.
Although Reidel's thyroiditis remains a primarily surgical disease, we have shown that combined therapy with prednisone and mycophenolate mofetil can produce a dramatic reduction in thyroid volume in patients with this disorder. Although the exact etiology of Reidel's thyroiditis remains unclear, recent reports have described the pathogenesis as a localized manifestation of a generalized fibroinflammatory process, thus associating the disease with the likes of idiopathic retroperitoneal fibrosis, sclerosing cholangitis, and Tolosa–Hunt syndrome. This association provides new treatment modalities for this rare disease, as immunomodulatory agents are typically utilized to blunt the fibroinflammatory process seen in such generalized conditions.
The anti-fibrotic effects of mycophenolate mofetil have not been previously evaluated in patients with Reidel's thyroiditis. Our report is the first to suggest the combination of mycophenolate and prednisone as a viable treatment option for patients with Reidel's thyroiditis. This observation lends further support to both the antifibrotic effects of mycophenolate mofetil and the fibroinflammatory mechanism of Reidel's thyroiditis.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.