
Abstract
Background:
In general, thyroid carcinomas, when they behave aggressively, metastasize to lungs and occasionally to bone and brain. Metastases to other organs are distinctly unusual. Renal metastases have been reported in only 10 patients. Here we report, to the best of our knowledge, the first patient with Hurthle cell thyroid cancer and renal metastasis. The evaluation of this patient was enhanced by utilizing a variety of imaging techniques.
Summary:
The patient was a 75-year-old man who had a history of a total thyroidectomy 9 years previously for a right thyroid lobe Hurthle cell carcinoma. He postoperatively received 150 mCi (5550 MBq) of 131-I therapy and was maintained on thyrotropin suppressive therapy with levothyroxine. He presented to us with a recent history of a progressively enlarging left neck mass. The serum thyroglobulin was elevated to 1183 ng/mL. Multimodality imaging with fluorodeoxyglucose positron emission tomography–computed tomography, magnetic resonance imaging, and Somatostatin receptor scintigraphy with single photon emission computed tomography (SPECT)-computed tomography revealed numerous foci in the skeleton and right kidney. Anatomic imaging characteristics favored a primary renal cell cancer with the additional evidence of renal vein invasion and thrombosis. Histology later revealed a metastatic renal Hurthle cell cancer with positive thyroglobulin stains. Several of the skeletal foci responded partially to cryoablative therapy. The patient refused noncurative Somatostatin analog therapy. He is alive and doing well clinically.
Conclusion:
The management of thyroid cancers in high-risk groups, such as our patient, frequently requires expert management by the use of novel multimodality imaging and therapeutic techniques.
Introduction
Patient
The patient was a 75-year-old man who presented with recurrent disease 9 years after a total thyroidectomy performed in 1997 for excision of a right thyroid lobe mass; the surgically excised pathology specimen demonstrated Hurthle cell thyroid carcinoma. Postoperatively, the patient was treated with 150 mCi (5550 MBq) 131-I and placed on levothyroxine (L-T4) suppressive therapy with L-T4 0.15 mg daily. Subsequently, the results of 131-I whole body scans in 1999, 2001, and 2003 were all negative and his thyroglobulin (Tg) levels remained undetectable. Other pertinent medical history was significant only for hypertension. The patient was retired, a nonsmoker, had no history of exposure to ionizing radiation, and had no family history of thyroid cancer or any other malignancy.
In early March 2006, clinical surveillance demonstrated gradual rise in Tg levels while under L-T4 suppression, prompting reevaluation with 131-I scan that revealed equivocal faint 131-I activity in the left neck, and administration of 150 mCi (5550 MBq) 131-I for treatment. However, on subsequent clinical examination a left-sided neck mass became palpable, and fine-needle aspiration biopsy of this mass was suspicious for Hurthle cell neoplasm. The patient underwent excision of the left-sided neck mass on March 28, 2006, and the pathology specimen demonstrated recurrent Hurthle cell carcinoma infiltrating the skin and subcutaneous tissues. Despite surgical resection of the recurrent tumor in the neck, biochemical monitoring revealed progressively rising Tg levels to 985 ng/mL in June 2006 and to 1164 ng/mL in August 2006 while under L-T4 suppression therapy (thyrotropin [TSH]: 0.4 mIU/L). Subsequent FDG PET-CT (fluorodeoxyglucose positron emission tomography–computed tomography) scan on September 11, 2006, revealed an intensely metabolically active right kidney mass suspicious for a renal cell carcinoma (Fig. 1). Additional metabolically active foci in the left scapula and the right acetabulum were consistent with skeletal metastatic disease (Fig. 2).
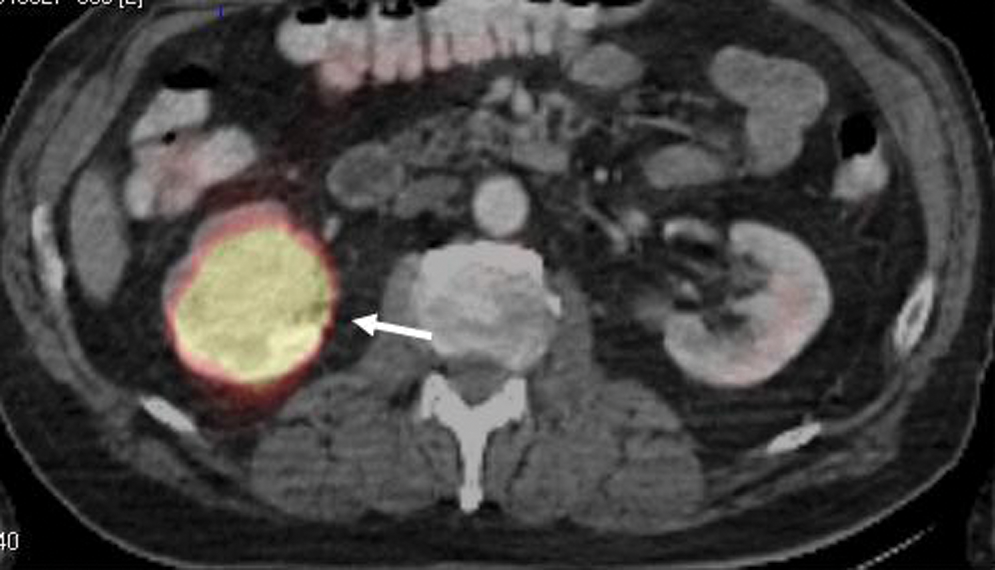
Initial fluorodeoxyglucose positron emission tomography–computed tomography renal mass (white arrow). Hurthle cell metastatic focus. Color images available online at
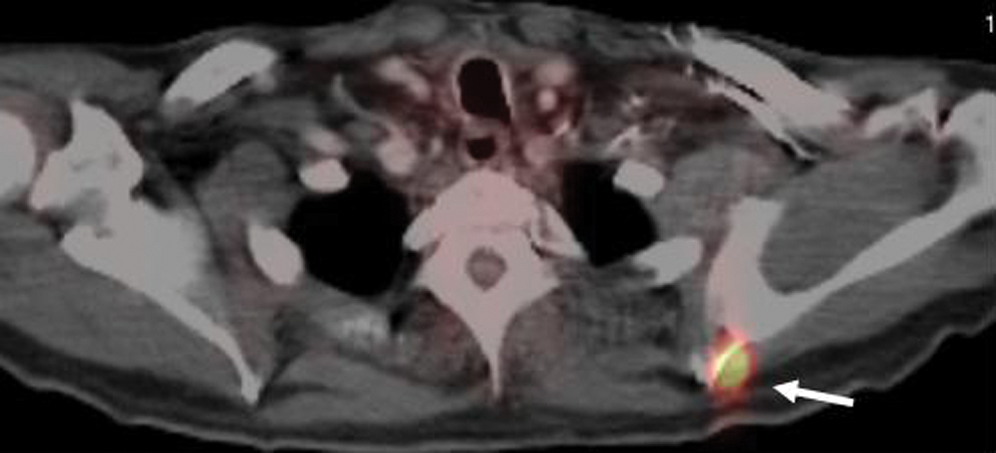
Initial fluorodeoxyglucose positron emission tomography–computed tomography with a metabolically active left scapular lesion (white arrow). Color images available online at
A magnetic resonance imaging revealed a large lobulated enhancing mass in the interpolar region and lower pole of the right kidney suspicious for a renal cell carcinoma invading the central renal sinus and suspicious for a tumor thrombus in the right renal vein but without extension into the inferior vena cava. Right radical nephrectomy and adrenalectomy on December 14, 2006, revealed a 5-cm tumor with a histological pattern consistent with Hurthle cell carcinoma and positive Tg staining (Fig. 3) involving the renal vein and invading the renal sinus fat. Vascular and ureteral margins were negative; the resected adrenal gland was negative for neoplastic involvement.

Renal Hurthle cell cancer pathological specimen. (
Immediately after surgery Tg levels decreased temporarily to 256 ng/mL (TSH: 0.09 mIU/L) but rose again to 595 ng/mL (TSH: 0.14 mIU/L), prompting another FDG PET scan on January 3, 2008, uncovering new metastatic lesions in the left supraclavicular fossa, right proximal humerus, and right pubic bone and interval worsening of abnormal FDG uptake in the right acetabulum. The left scapular lesion demonstrated a patchier uptake that extended into the adjacent soft tissues (Fig. 4).
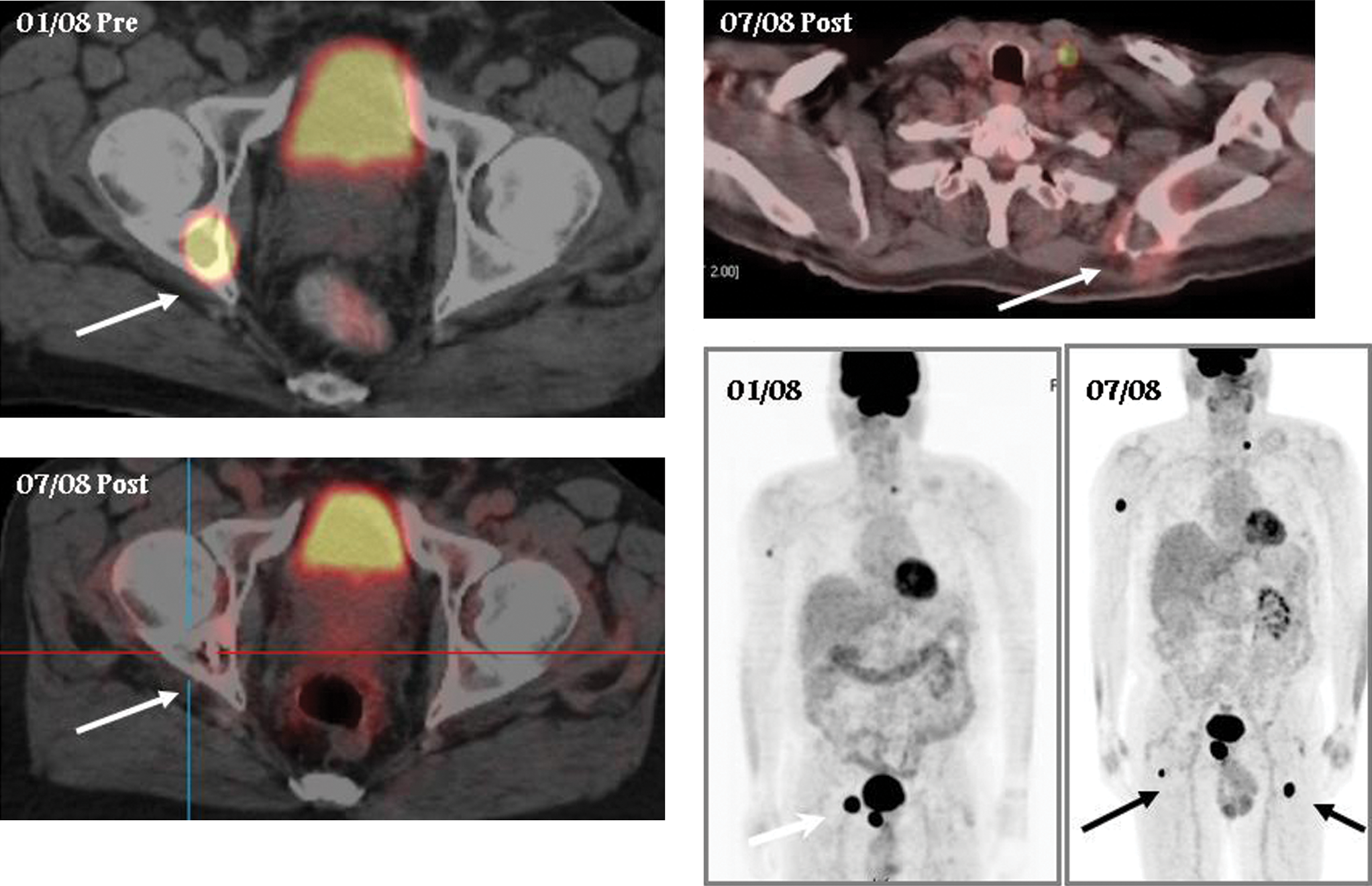
Follow-up scan 6 months postcryoablation → Treatment. Response: right acetabulum and left scapula. 01/08 and 7/24/08 (white arrows) → new lesions (black arrows). Color images available online at
In anticipation of possible Sandostatin long acting release (LAR) therapy, an Octreotide scan was performed, which revealed Somatostatin receptor expressing lesions in the left scapula, right pubic bone, right acetabulum, the right mid humerus, and the right posterior elements of C5 (Fig. 5). The patient underwent cryoablation of his scapular lesion and right acetabulum with some improvement; however, his disease continued to progress clinically with rising biomarkers. The Tg level was 974 ng/mL on July 22, 2008, when his TSH was 0.04 mIU/L, and there was progression of disease on his follow-up FDG PET-CT scan (Fig. 4).

Octreotide avid right acetabulum site (arrow).
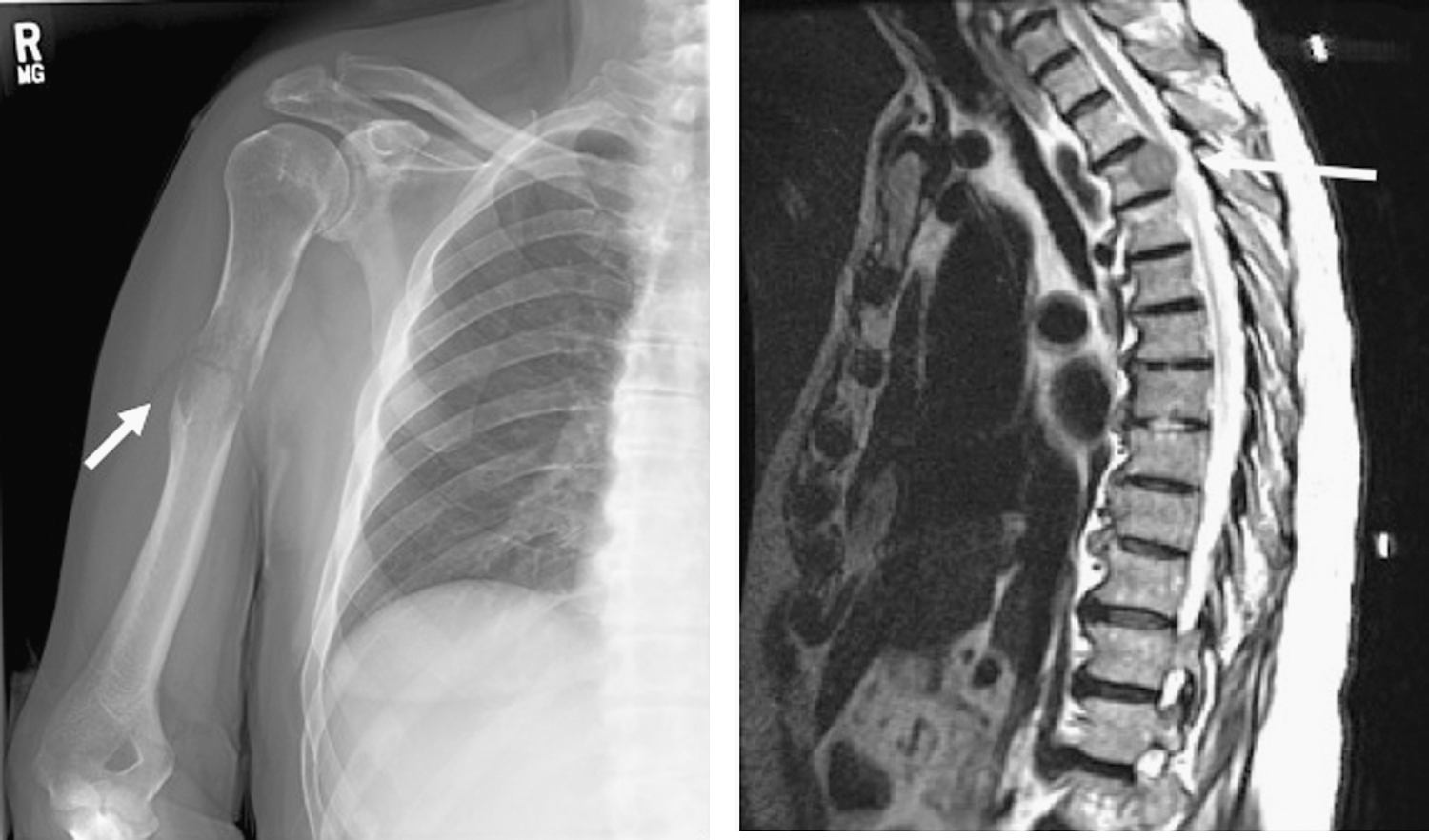
The patient refused Sandostatin LAR or biphosphonate therapy and opted for a holistic medicinal approach using dichloroacetate and vitamin C infusions. In August 2009, the patient presented with a pathologic fracture of the right humerus (Fig. 6). The patient declined surgical resection of the osseous metastatic lesion opting for a Sarmiento brace to stabilize the bone. In September 2009, the patient presented with difficulty ambulating and a focal sensory deficit in the left lower extremity, and a magnetic resonance imaging performed on September 28, 2009, demonstrated a new T3 vertebral lesion with encroachment upon the spinal cord (Fig. 6). He was treated with Decadron and conventional fractionated radiation therapy delivering a total of 30 Gy in daily 3 Gy fractions over the course of 2 weeks. Currently, he is clinically stable; however, his Tg levels continue to rise (most recent level on October 22, 2009: Tg 14113 ng/mL; TSH 0.08 mU/L) consistent with continued advancement of his metastatic disease.
(
Discussion
Kidney metastases are usually a rare occurrence and even less commonly of thyroid origin. Only 10 patients have been reported so far, 7 of follicular and 3 of papillary origin (3 –5). Hurthle cell cancer is considered a variant of follicular cell thyroid cancer and represents 3% of thyroid carcinomas; it is defined by the presence of more than 75% of oncocytic cells with an eosinophilic cytoplasm and a trabecular/follicular growth pattern.
With the advent of novel imaging techniques and therapy options, a more aggressive management approach and expert opinion involvement is necessary in the management of high-risk thyroid cancer patients. Our patient had several adverse prognostic indicators, including age, sex, the Hurthle cell histology, and distant aggressive metastatic disease involving the skeleton and a large renal metastasis occurring more than 5 years after initial diagnosis. His metastatic disease did not concentrate radioiodine, as evidenced by negative 131-I scans, and was highly metabolically active on fluorine-18-labeled FDG PET-CT scans.
Early-stage thyroid cancers have a benign course; however, in cases presenting with advanced (stage IV) disease where the tumor exhibits an aggressive biological behavior, expert multimodality imaging is essential for accurate assessment of the extent of disease, guiding treatment to halt progression and improve survival. Recently, fluorine-18-labeled FDG PET-CT has been shown to detect the aggressive transformation of thyroid cancers and uncover dedifferentiated disease characterized by a loss of capacity to concentrate iodine, the so-called noniodine avid thyroid cancer. FDG PET-CT may also occasionally be used to image these more aggressive iodine avid thyroid cancers (6,7). Hormone withdrawal and recombinant human TSH stimulation have been used with variable success. Finally, somatostatin receptor scintigraphy may image various types of thyroid tumors (8), especially when Tg is above 10 ng/mL. This appears to have the potential for therapy use with somatostatin analogs.
It is crucial to understand the natural course, genetics, and biology of these more aggressive tumors and develop adequate therapies. The current approach is aggressive tumor resection both locally and at distant sites, as it offers the best survival. If bony lesions are resected, a prosthesis may be inserted. The multitude and locations of the skeletal lesions in our patient limited this option.
Radiofrequency and cryoablation for various cancers has gained clinical interest recently. These procedures have been used to treat difficult metastases in liver, lung, renal, and prostate cancers. They have rarely been used to treat thyroid metastasis, however (9,10). They may alleviate pain and reduce tumor bulk, but survival data are not readily available. In our patient, cryoablation was used effectively with some relief of pain caused by multiple skeletal metastases.
In summary, the management of high-risk thyroid cancers can be enhanced by the use of novel multimodality imaging and therapeutic techniques.
Footnotes
Disclosure Statement
All authors have no relevant disclosures.