
Abstract
Background:
Papillary thyroid carcinoma (PTC) cells express oncofetal fibronectin (onfFN) mRNA, which may be useful to detect circulating tumor cells. The objective of this study was to determine the fraction of PTC patients having onfFN mRNA in their peripheral blood and to determine if onfFN mRNA levels are correlated with the status of the disease or with thyroid-stimulating hormone (TSH) serum concentrations.
Methods:
This study included 95 PTC patients, who were previously treated by thyroidectomy and radioactive iodine administration. Patients were examined by cervical sonography, whole-body 131I scintigraphy, thyroglobulin measurement, and onfFN mRNA quantification both when they were being treated with L-thyroxine (L-T4) and after L-T4 withdrawal. The mean value for onfFN mRNA in blood from 25 healthy subjects was used as control for the onfFN mRNA assay.
Results:
After L-T4 withdrawal, serum TSH levels rose and onfFN mRNA was found in the peripheral blood of 33 of 64 (52%) disease-free patients, 15 of 23 (65%) patients with local residual disease, and 6 of 8 (75%) patients with known local or distant metastases. Continuous administration of L-T4 repressed serum TSH. In this state none of 17 (0%) disease-free patients and 1 of 4 (25%) patients with local residual disease had an elevated onfFN mRNA level, and 2 of 4 (50%) patients with metastasis had positive tests for serum onfFN mRNA.
Conclusions:
onfFN transcripts are highly abundant in the peripheral blood of patients with PTC. L-T4 withdrawal, which produced elevated serum TSH concentrations in these athyroidic patients, markedly increased the fraction with positive tests for serum onfFN mRNA at all stages of the disease. Analyzing onfFN mRNA in the absence of a TSH stimulus allows a much better discrimination of different states of PTC disease and, based on current concepts of the significance of circulating mRNA, may be a useful tool to detect circulating thyroid cancer cells.
Introduction
The long-term management of patients with PTC includes periodic cervical ultrasonography, whole-body 131I scintigraphy (WBS), and serum thyroglobulin (Tg) measurements. Tg is the most sensitive and specific marker of residual or recurrent disease (4), but its sensitivity is enhanced if there is stimulation of residual or recurrent carcinoma cells by thyroid-stimulating hormone (TSH) (5). TSH levels can be elevated by exogenous administration of recombinant human TSH (rhTSH) or by withdrawal of oral L-thyroxine (L-T4) supplements. L-T4 withdrawal induces hypothyroidism in thyroidectomized patients who often become symptomatic with reduced quality of life. Importantly, TSH is a thyroid growth factor and PTC cells often express TSH receptors (TSHRs) (6). Thus, TSH stimulates all TSHR-expressing cells, including disseminated or circulating thyroid carcinoma cells, thereby facilitating disease recurrence (3,7). This concept is supported by reports of tumor recurrence after L-T4 withdrawal or administration of rhTSH (8).
Several groups have developed alternative approaches aimed at detecting recurrent FTC or PTC at an early stage without the need for a high endogenous TSH levels by analyzing molecular markers of circulating thyroid cancer cells (reviewed in Refs. 2,9 –11). A recent report from our group has described a highly sensitive assay to quantify oncofetal fibronectin (onfFN) mRNA in the peripheral blood of patients with DTC metastatic disease (12). As discussed later, we consider that onfFN mRNA in peripheral blood is probably derived from circulating rather than tissue cells.
In this study we used our previously established assay to determine the fraction of PTC patients having onfFN mRNA in their peripheral blood and to analyze if onfFN mRNA levels are correlated with the status of the disease or with TSH serum concentrations.
Subjects and Methods
Study subjects
The university ethics committee approved the study, and written informed consent was obtained from all participants. Twenty-five age- and sex-matched healthy control subjects and 95 patients with a history of PTC without anti-Tg antibodies were included in this study. PTCs were removed by total or near-total thyroidectomy, and ablation of remaining thyroid tissue was performed in all patients using 3.7 GBq of 131I. Patients were operated again if residual thyroid tissue was found within 3 months after surgery. If thyroid tissue was still persistent after surgery, a dose of 3.7 GBq 131I was administered. In most patients with metastases, 3.7 GBq 131I were given followed by 7.4 GBq 131I 1 week later. In addition, routine long-term follow-up examinations were performed in all patients to detect residual or metastatic PTC. Follow-up examinations were performed 4 weeks after withdrawal of the oral L-T4 supplementation. Serum TSH was elevated to >30 mIU/L in all patients when they were studied again to include cervical ultrasonography, WBS, and serum Tg measurement. Even if the imaging was negative, patients were considered to have DTC metastases if their serum Tg level was increased to at least >2.0 μg/L. Clinical data such as tumor characteristics, including the pathological tumor classification and affected lymph nodes and metastasis, were evaluated according to the sixth edition of the TNM classification for thyroid carcinoma (13). On the basis of these results all 95 patients were divided into three groups: disease free, local residual disease, and local or distant metastases. Sixty-four patients were disease free, 23 were found to have local residual disease, and local or distant metastases were found in 8 patients (Table 1).
p < 0.005.
ND, not determined; onfFN, oncofetal fibronectin; TSH, thyroid-stimulating hormone; WBS, whole-body 131I scintigraphy.
A second follow-up examination was performed after patients were put back on L-T4 supplementation to achieve low endogenous TSH levels. This second examination included 17 disease-free patients and 4 patients with residual or metastatic disease (Table 2). This was done to determine the influence of L-T4 administration with reduction in serum TSH on serum onfFN mRNA.
Cervical ultrasonography
Two experienced physicians performed the cervical ultrasonography independently using a real-time sonographic scanner equipped with a 7.5-MHz transducer (Siemens Sonoline versa pro, Munich, Germany) before the administration of the tracer dose of 131I, which was required for the WBS. The scan covered the entire neck region and revealed lymph nodes or tumor lesions in the thyroid bed, the area below the clavicles, the upper mediastinum, areas lateral to the carotid arteries and jugular veins, as well as in the submandibular region.
131I whole-body scintigraphy
A tracer dose of 370 MBq 131I was administered orally. After 48–72 hours, a diagnostic WBS was performed for 15–20 minutes using a dual-head Anger camera equipped with a high-energy collimator (Siemens Bodyscan, Munich, Germany). WBSs were counted as positive if an increased focal activity was found in regions that do not normally accumulate 131I. Two experienced physicians independently evaluated all WBSs in a random and blinded fashion.
Measurement of serum TSH and Tg
Serum TSH was quantified using a routine chemiluminescence test (Chiron Diagnostics, Wiesentheid, Germany). The physiological range for serum TSH was 0.27–4.2 mIU/L. Serum Tg was quantified by radioimmunoabsorbent assay (Medipan, Dahlewitz, Germany) with a lower detection limit of 0.3 μg/L and an interassay variability of 5%–10%. A Tg level <0.3 μg/L was defined as negative, and a Tg level between 0.3 and 2.0 μg/L was classified as intermediate. A serum Tg level >2.0 μg/L was considered indicative of local disease recurrence or metastases.
Quantification of onfFN mRNA
Mononuclear cells were isolated from 5.0 mL ethylenediaminetetraacetic-acid-treated peripheral venous blood by Ficoll-Paque (Nycomed, Oslo, Norway) density gradient centrifugation. Total RNA was isolated using the RNeasy Kit (Qiagen, Hilden, Germany) followed by a DNase I (Roche Diagnostics, Mannheim, Germany) digest to eliminate genomic DNA. cDNA was synthesized using 1.0 μg total RNA and oligo dT20 oligonucleotides. onfFN mRNA transcripts were quantified by real-time polymerase chain reaction analysis (LightCycler; Roche Diagnostics). Copy numbers were normalized to porphobilinogen desaminase, and results were expressed as arbitrary units. All procedures have been described previously in all details (12).
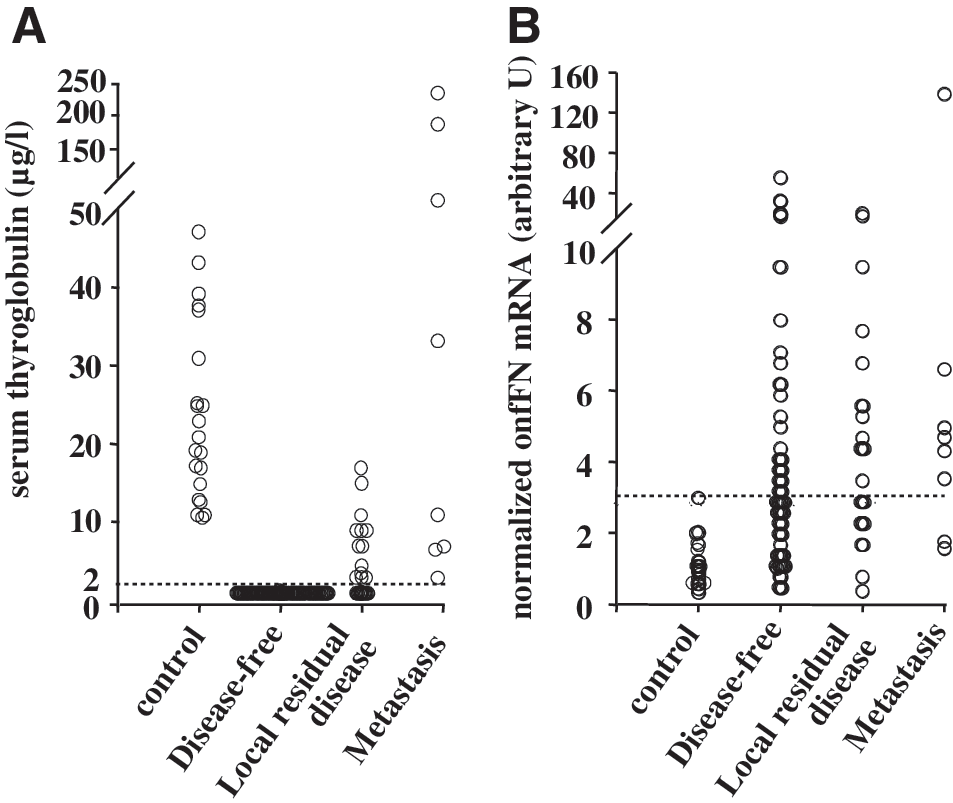
To distinguish a PTC-dependent elevated amount of onfFN mRNA from a nonspecific background signal, we quantified onfFN transcripts in the peripheral blood of 25 healthy control subjects and determined a diagnostic cutoff. The healthy subjects therefore served as a zero baseline controls (hereafter referred to as controls). The onfFN mRNA expression in controls was calculated as 1.0 (arbitrary U) and demonstrated a standard deviation of 0.6 (Table 1). The cutoff was then calculated to be 3.1 (arbitrary U), which equals mean +(3 × standard deviation). Only values above this cutoff were counted as positive (Fig. 1B). To analyze the abundance of onfFN transcripts in patients with PTC and to determine a correlation with the status of the disease, onfFN transcripts were quantified in each patient.
(
Statistical analysis
Differences in the abundance of onfFN mRNA transcripts between groups were evaluated by the Mann–Whitney U-test using SPSS® (SPSS, version 11.0, Chicago, IL). p < 0.01 was considered to be statistically significant.
Results
Subject characteristics
This study included 95 patients. More than two-third (64 of 95, ∼67%) of the patients were disease free, less than a quarter (23 of 95, ∼24%) suffered from residual disease, and only ∼9% (8 of 95) were found to have metastasis. About two-third (64 of 95, ∼67%) of our patients were women and about one-third (31 of 95, ∼33%) were men. Patients with distant or local metastases were approximately 15 years older (67.4 ± 17.4 years) than patients who were free of disease (52.3 ± 12.2) or who were found to have local residual disease (53.1 ± 11.6) (Table 1).
The second follow-up evaluation after patients were put back on L-T4 included 25 patients. The group of disease-free patients was again the largest group (17 of 25, ∼68%) and contained nine female (∼53%) and eight male (∼47%) patients. The groups of local residual or metastatic disease each consisted of four patients, four female (100%) and no male (0%) patients in the former group and three female (75%) and one male (25%) patients in the latter group. Again patients with metastasis were older (67.3 ± 13.9 years) than disease-free patients (54.5 ± 14.5 years) or patients with local residual disease (45.8 ± 11.1) (Table 2).
Tumor characteristics
At the time of diagnosis, several tumor characteristics, including the pathological tumor classification, affected lymph nodes and metastasis, and the grading of the PTCs, were determined. Consistent with the clinical course of the disease, patients who remained disease free after therapy had PTCs of a low tumor classification and grading (Table 1). The majority of these patients had no affected lymph nodes or metastasis. In contrast, patients who presented with metastasis after treatment had PTCs of a higher tumor classification and grading. Lymph nodes were more frequently affected and more metastases were found at the time of diagnosis compared to patients who remained disease free. Patients with local residual disease had tumors of intermediate classification and grading. The involvement of lymph nodes and the presence of metastases were in between the group's disease free and metastasis (Table 1).
Tumor imaging
Cervical sonography and WBS were used for tumor imaging. Negative sonography and WBS were a prerequisite for patients to be classified as disease free. Local residual disease was detected by cervical sonography in 86% of the cases and in 91% by WBS in the respective group. In patients with metastatic disease, cervical sonography revealed local metastases in 25% and WBS detected local or distant metastases in half of the cases (Table 1). Without the stimulation by TSH during the second follow-up examination, the sensitivity of cervical sonography to detect local tumor growth was greatly diminished and revealed a positive result in only 25% of the cases in the groups of patients with either local residual disease or metastasis (Table 2). WBS was not performed during the second clinical evaluation.
Serum TSH and Tg
Withdrawal of oral T4 supplementation during the first follow-up examination resulted in highly elevated serum TSH levels in all patients of the three groups. An elevated serum TSH level was found in all disease-free patients with a mean value of 77.5 ± 40.6 mIU/L (physiological range: 0.27–4.2 mIU/L); patients with local residual disease and patients with metastasis had a mean TSH level of 64.1 ± 40.8 mIU/L and 64.2 ± 43.5 mIU/L, respectively (Table 1). The highly elevated serum TSH levels most likely stimulated PTC cells, a well-known prerequisite for measurements of serum Tg to be a sensitive indicator of residual or recurrent disease. More than half (57%) of the patients with local residual disease had a positive serum Tg level, and all patients with metastases were positive. Due to a healthy thyroid gland, control subjects always had a serum Tg level >2.0 μg/L even without any hormonal manipulation (Table 1). In the second follow-up examination after resumption of L-T4 treatment serum TSH concentrations were suppressed in all groups, and about half of the patients with local residual disease and about half of the patients with metastatic disease had positive serum Tg values (Table 2).
onfFN mRNA, disease status, and serum TSH
The expression of onfFN mRNA was significantly greater in patients that were free of disease or that were diagnosed with local residual disease at time that they were not on L-T4 replacement than in the control subjects (Fig. 1B). There was also a strong trend to higher expression rates of onfFN-mRNA in patients that had evidence of local or distant metastases. The disease-free patients had a median onfFN mRNA value of 3.0 (range, 0.4–55.1; p = 0.005) (arbitrary U). Patients with local residual disease had a median onfFN mRNA value of 4.3 (range, 0.5–16.9; p = 0.004) (arbitrary U), and patients with metastatic disease had a median onfFN mRNA value of 4.5 (range, 1.6–138.7; p = 0.223) (arbitrary U) (Table 1). Although there was a trend toward a higher concentration of onfFN mRNA in patients with metastasis compared to the other DTC groups, this was not significant.
Thirty-three of 64 disease-free patients (52%) were positive for circulating onfFN mRNA. This was the case in 15 of 23 patients (65%) with local residual disease and in 6 of 8 cases (75%) of patients with local or distant metastases (Table 1). Although the values for circulating onfFN mRNA were significantly different in disease-free patients and patients with local residual disease compared to control individuals (Table 1), no significant difference was found between the groups of patients. The fraction of patients having circulating onfFN mRNA was considerably lower when they were tested at a time that they were on L-T4 treatment with its associated with suppressed serum TSH concentrations. None of 17 disease-free patients were positive for circulating onfFN mRNA. Only one of four (25%) patients with local residual disease and two of four patients (50%) with metastases were positive for onfFN mRNA (Table 2; Fig. 2A–C). The latter two groups were too small for satisfactory statistical analysis.
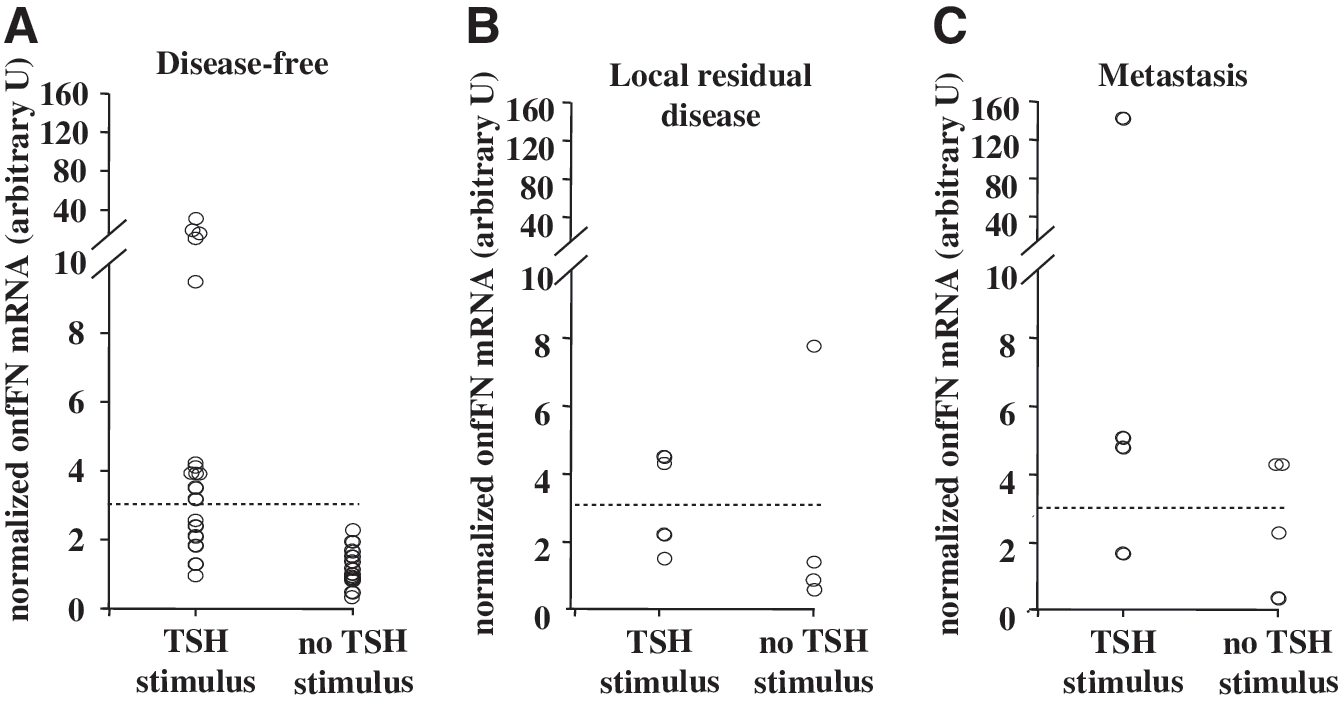
Quantification of onfFN mRNA expression (onfFN mRNA, ordinate) in the peripheral blood of patients with and without TSH stimulus (TSH stimulus, abscissa) at different disease status after treatment of a PTC. TSH stimulus, not on L-T4; no TSH stimulus, on TSH suppressive doses of L-T4. Examined were (
Discussion
The aim of this study was to determine the fraction of patients with various stages of DTC having circulating onfFN mRNA, the concentrations of this substance in these groups, and the relationship of this to situations where circulating TSH was either suppressed or elevated. We hypothesize that in the setting of our patients, circulating onfFN mRNA originated from circulating DTC cells. Evidence in support of this hypothesis is that onfFN mRNA is undetectable in healthy individuals but highly abundant in the peripheral blood in patients with a history of DTC. Further, our group reported previously that onfFN mRNA is not detectable in different groups of nucleated blood cells, but it is highly expressed by DTCs (12).
We noted that circulating onfFN mRNA was much more likely to be detected in our DTC patients after they stopped L-T4 than when they were taking suppressive doses of L-T4, and we hypothesize that this difference was caused by an ability of TSH, whose levels differed markedly in these two settings, to stimulate the production of onfFN mRNA and/or to facilitate the invasion of DTC tumor cells into the blood stream, regardless of what stage their DTC was in.
The current management and follow-up of patients with DTC regimen consists of cervical sonography, WBS, and serum Tg measurements. Unfortunately, some of these techniques are most sensitive when serum TSH concentrations are elevated (3,7,14). This is not an ideal situation, however, since TSH is a thyroid growth hormone and high TSH serum concentrations likely promote the malignant behavior of DTC (15). TSH is postulated to stimulate occult thyroid cancer cells, causing them to proliferate at a higher rate and/or enter the bloodstream to eventually give rise to distant metastases (14). The ability to quantify circulating tumor cells (CTCs) should be useful in managing PTC and in developing and improving treatments. The ability to do so, however, is a challenge because of technical and biological limitations (11) and a reliable method is currently not available.
A limiting factor in detecting CTCs is the kinetics by which tumor cells enter the circulation and remain in the blood. Cancer cells are intermittently shed into the bloodstream and persist only for a relatively short period (16). Thus, patients with a negative result may still have CTCs that might be detected at another time point or under different circumstances. Although cancer cells do circulate in the blood even at early stages of thyroid cancer, the total cell number per volume varies greatly (17). Thus, the time, frequency, and sample volume are all critical factors that may influence the results and their interpretation. Data interpretation is also complicated by the fact that CTCs do not necessarily cause metastases because only very few cancer cells survive the attacks by the immune defense system or other events that prevent the establishment of metastatic disease (16).
During the last decade, numerous groups have tested many candidate gene products in an attempt to find a suitable marker of CTCs, but there has been considerable variability in the studies (9,11). Putative thyrocyte-specific markers such as mRNAs for Tg (12,18 –20), TSHR (5,12), or thyroid peroxidase (17) turned out not to be nearly as useful as initially anticipated due to interfering effects such as ectopic transcription or pseudogene expression (2,5,11,12). Our group and others reported the detection of circulating PTC cells by quantifying onfFN mRNA, a pathologically occurring isoform of fibronectin (12,21,22). Physiologically, alternative splicing of the fibronectin transcript leads to 20 distinct isoforms that differ in the number of internal repeats and give rise to plasma and cellular forms of fibronectin. Posttranscriptional modification of fibronectin occurs in a cell-specific, tissue-specific, and developmentally specific manner and is deregulated under pathologic conditions (23). Fibronectin isoforms that arise in malignant cells such as onfFN are distinct from physiological plasma and cellular isoforms in terms of molecular size, glycosylation pattern, and the composition of different internal repeats (24,25). Isoforms containing repeats of the III connecting segment, and the extracellular domains A and B are expressed to a greater extent in tumor tissues and in transformed human cell lines (26). The III connecting segment domain is characteristic for onfFN and was therefore used for amplification in this study. Oncofetal fibronectin mRNA is expressed in 98% of PTC (12,27) and other types of cancer (24,25,28), but it is not ectopically transcribed in the peripheral blood of healthy subjects (12). These characteristics strongly support onfFN as a candidate target sequence for detecting CTCs.
We found a significant difference in both the number of onfFN-positive subjects and the mean expression rate of onfFN mRNA between healthy controls and patients who had been treated for PTC and were then evaluated during a follow-up examination after L-T4 withdrawal. However, the level of onfFN mRNA did not vary between patients who were free of disease, or who had local residual disease or metastases, and therefore did not correlate with the clinical status of the disease. Interestingly, these results also demonstrate that disease-free patients had higher onfFN mRNA levels than the control group but a distribution similar to the residual disease group. These data therefore suggest an occult disease, which would imply a higher sensitivity of measuring onfFN mRNA levels compared to stimulated serum Tg. There was also no association between the amount of onfFN mRNA and the results of the tumor imaging or the level of serum Tg. Similar observations have been described in a study published by Ishikawa et al., who found no significant correlation between the level of circulating thyroid peroxidase mRNA in peripheral blood and the clinical characteristics, including serum Tg levels and the size or stage of PTC (17). In another study Sato et al. investigated the prevalence of patients who were positive for carcinoembryonic antigen mRNA and found no significant association between carcinoembryonic antigen mRNA expression and features like age, tumor size, nodal metastasis, and histologic differentiation (16). Although the absolute amount of a particular molecular marker seems to be irrelevant, the percentage of patients with an onfFN mRNA value above the cutoff was, compared to disease-free patients, increased in the group of patients with local residual disease and was even further increased in patients with metastatic disease. This suggests that the amount of onfFN mRNA could be related with the total tumor burden and/or the differentiation stage of the tumor cells. This can at least in part be explained by the kinetics of tumor cell circulation. If tumor cells are indeed circulating in the peripheral blood due to an advanced status of the disease or distant metastases, tumor cells will be detected in a stochastic manner; that is, the more frequent cells circulate, the more patients will be tested positive. The absolute amount of the signal depends, however, on the absolute number of tumor cells that were present in the blood sample and may therefore vary from time to time due to heterogeneous tumor cell aggregates.
The follow-up evaluation of patients who have been treated for PTC is generally performed at a time that serum concentrations of TSH are high, either due to the administration of rhTSH or due to withdrawal of their L-T4 supplement (3,7,14). Because TSH is a very potent stimulating growth hormone for thyrocytes that has been linked with the pathogenesis of thyroid cancer (15) and because thyroid cancer cells are known to express functional TSHRs (5), we hypothesized that TSH may have a positive effect on CTCs. To test this hypothesis, we repeated the quantification of onfFN mRNA but without withdrawal of L-T4 and therefore with nonelevated TSH serum levels in subpopulations of all three previously examined groups of patients. We found that the rate of positive patients and therefore also the mean amount of onfFN mRNA greatly decreased in all three groups of patients. Since the decrease in onfFN mRNA was even among all groups, the positive rate still correlated with the status of the disease, indicating that this method of quantification does not necessarily depend on a TSH stimulus to be sensitive. This observation supports the hypothesis that TSH increases the abundance of circulating thyroid cancer cells in the peripheral blood either by increasing the proliferation of tumor cells that circulate already or by facilitating the entry of tumor cells into the bloodstream or by a combination of both and maybe other mechanisms. The resulting increased abundance of CTCs is detectable by quantifying onfFN mRNA, which is not thyrocyte specific but fulfills the most important criteria for a molecular marker.
This study demonstrates that onfFN transcripts are highly abundant in the peripheral blood of patients with PTC. High levels of serum TSH correlated with high rates of onfFN mRNA-positive patients at all stages of the disease. At the moment, serum Tg is still the most sensitive and specific marker of residual or recurrent thyroid cancer disease. As the Tg assay sensitivity depends on the stimulation by TSH, we believe that the quantification of onfFN mRNA could become a useful supplemental tool to monitor patients after treatment of a PTC for circulating thyroid cancer cells, especially while they are on L-T4 treatment.
Footnotes
Acknowledgments
The authors thank Bernadette Luens, Frank Dsiosa, and Klaus Burfeind for their outstanding help in sample processing and data collection. The authors are indebted to Zekiye Korkmaz for assisting in obtaining patient information.
Disclosure Statement
The authors declare that no competing financial interests exist.