
Abstract
Background:
Evidence suggests that selenium (Se) supplementation could be useful as an adjunctive therapy to levothyroxine (LT4) in the treatment of Hashimoto's thyroiditis (HT). To summarize evidence regarding its effect on thyroid autoantibodies' titers, demands in LT4 replacement therapy, ultrasonographic thyroid morphology, and mood in patients with HT under LT4 treatment, a systematic review and meta-analysis of relevant literature were performed.
Methods:
Systematic review of prospective studies involving patients with HT under LT4 treatment and meta-analysis of studies on randomized, placebo-controlled, blinded trials were performed.
Results:
Patients with HT assigned to Se supplementation for 3 months demonstrated significantly lower thyroid peroxidase autoantibodies (TPOab) titers (four studies, random effects weighted mean difference: −271.09, 95% confidence interval: −421.98 to −120.19, p < 10−4) and a significantly higher chance of reporting an improvement in well-being and/or mood (three studies, random effects risk ratio: 2.79, 95% confidence interval: 1.21–6.47, p = 0.016) when compared with controls. Demands in LT4 replacement therapy and ultrasonographic thyroid morphology were found either unaltered or underreported.
Conclusions:
On the basis of the best available evidence, Se supplementation is associated with a significant decrease in TPOab titers at 3 months and with improvement in mood and/or general well-being. Evidence suggests a different pattern of response to Se supplementation in HT relative to baseline TPOab titers, and this, if confirmed, could be used to identify which patients would benefit most from treatment. An improvement in thyroid function and morphology should be demonstrated before Se routine supplementation can be recommended in the treatment of HT.
Introduction
Chronic autoimmune (Hashimoto's) thyroiditis (HT) is the most common thyroid disorder in iodine-sufficient areas. HT is characterized by the presence of complement-fixing autoantibodies to thyroid peroxidase autoantibodies (TPOab) (8), which are closely associated with overt thyroid dysfunction and tend to correlate with progressive thyroidal damage and lymphocytic inflammation (9). Along with several genetic and environmental factors, Se deficiency has been implicated in its pathogenesis (9 –12). In animal models, impaired GPx, as in states of Se deficiency, may contribute to oxidative (free radical) damage of the thyroid cell, initiation of fibrosis, and impaired tissue repair (13,14). In addition, Se deficiency may be associated with an impairment in both T-cell- and B-cell-mediated immunity (15), given its significant role in the immune system (16). However, it remains unclear if Se deficiency can induce HT in humans (15). Evaluating this possible association or causation is further complicated given that serum Se concentrations do not reflect tissue concentrations (17), normal basal serum Se concentrations do not exclude low intrathyroidal Se concentrations (18), and higher than previously thought Se intake is required to obtain full expression of at least one selenoprotein, namely selenoprotein P (7).
Because of its structural and functional role in the thyroid microenvironment and its possible implication into HT pathogenesis, the aim of several studies has been to investigate the potential therapeutic effect of Se supplementation (i.e., Se administration as an adjunctive therapeutic modality to levo-T4 [LT4]) in HT in patients with different baseline Se statuses. The findings have been equivocal. In a recent randomized trial (19), no benefit was detected after Se supplementation in a cohort of Se-sufficient HT patients. This contrasts with previous studies, in which a decrease in TPOab titers and/or an improvement in thyroid echogenicity was noted in patients with various degrees of Se sufficiency (15,18,20 –22). It is notable that different forms of Se preparations (selenomethionine and sodium selenite) were used in these studies. Further, no definitive information about the duration of Se supplementation, the time of maximum response to treatment, and the patient subgroups were readily available.
In an attempt to summarize available data and provide an evidence-based recommendation regarding Se supplementation in the treatment of HT, a systematic review and a meta-analysis were performed.
Methods
Search strategy
A preliminary search was conducted in MEDLINE using the terms “selenium” (MeSH) and “autoimmune thyroiditis” (MeSH) to evaluate the size of the relevant bibliography and choose keywords for the main search. To identify eligible studies, the main search was conducted in the electronic databases MEDLINE, EMBASE, PubMed, Web of Science, and Cochrane Central Register of Controlled Trials (CENTRAL) from inception through September 2009, using the terms “selenium” (MeSH) or “
Eligibility of relevant studies
Studies eligible for the systematic review were those in which the effects of Se supplementation in patients with HT had been prospectively investigated. Studies were excluded from the systematic review if they involved participants (i) with a thyroid disease other than HT, (ii) under medication that could affect thyroid hormones, autoantibodies, or Se concentrations, and (iii) in pregnancy. Further, (iv) reviews or letters to the editors and (v) studies for which assessment of their accordance with the predefined inclusion criteria was not possible were excluded. To ensure synthesis of the best available evidence, only studies that were blinded, randomized, placebo-controlled in design were considered eligible for the meta-analysis. Open-label and/or uncontrolled studies were excluded from the meta-analysis.
Data extraction
Information from each study was extracted independently by two reviewers (K.A.T. and T.G.T.), using a standardized data extraction form. Study characteristics (author, year of publication, country, study design and duration, recruitment period, sample size) as well as the characteristics of the study groups were recorded. These included their comparability on baseline characteristics (age, sex, body mass index, thyroid function tests, years from first diagnosis, Se status before treatment), methodology (inclusion criteria, HT definition, thyroid autoantibodies measurement method, threshold and time of measurement), and outcomes (TPOab and antithyroglobulin autoantibodies [TGab] titers, thyroid ultrasonography [U/S], quality of life at baseline and at endpoint). Other outcomes were recorded, where available, and double checked.
Outcomes of the meta-analysis
The main outcome of the meta-analysis was weighted mean difference (WMD) in TPOab titers between Se supplementation and placebo groups at 3 months. This analysis was feasible, because TPOab titers were comparable at baseline between groups. To gain a more thorough perception of the effects of Se supplementation in HT, the probability of a reported improvement in mood status and/or well-being served as a secondary outcome measure.
Statistical analysis
TPOab titers after a 3-month period of Se supplementation were extracted in each trial as mean difference ± standard deviation. WMDs were calculated and combined using random effects model. The probability of a reported improvement in well-being and/or mood was treated as a dichotomous outcome, expressed as risk ratio with 95% confidence interval (CI) and combined using a random effects model. Random effects model was preferred over fixed effects, because evidence of significant heterogeneity was present. Heterogeneity between the results of different studies was examined by I 2 test for inconsistency (I 2 > 50%: significant heterogeneity; I 2 = 25%–50%: moderate heterogeneity; I 2 < 25%: insignificant heterogeneity), which can be interpreted as the percentage of total variation across several studies due to heterogeneity (23). To assess the extent of publication bias, tests for rank correlation and regression asymmetry (Egger test) were used (24). Meta-analysis was conducted using Stata/SE 10.0 for Windows (StataCorp LP, College Station, TX).
Results
Search results
A flow chart summarizing search results is provided in Figure 1. The main search strategy identified 31 potentially relevant publications. Eighteen of them were excluded because they were reviews (n = 8), case series, case reports or letters to the editor (n = 8), preclinical experimental study in rats (n = 1), or duplicate (n = 1). The remaining 13 publications were read in full independently by two reviewers to assess their accordance with the selection criteria. Three of them were excluded because no intervention had been undertaken, although serum Se concentrations in HT were evaluated (25 –27). One study was excluded because it was retrospective in design and had involved patients with Graves' disease (28). A prospective, blinded, randomized, placebo-controlled study investigating the effect of Se supplementation on postpartum thyroiditis in pregnant women was also excluded (29). Finally, two studies were excluded because their accordance with the predefined inclusion criteria was not possible, despite efforts to communicate with the primary investigators (30,31). In total, six studies were included into the systematic review. Two of them were excluded from the meta-analysis, because they were not placebo controlled and/or blinded in design (20,22).

Flow chart for the systematic review and the meta-analysis.
Systematic review
The six studies included in the systematic review were published between 2002 and 2007 and reported data on 339 patients with HT (330 women). Main data are summarized in Tables 1 and 2. All trials were held in Europe, with the exception of one that was held in Asia (Turkey). Four of them were prospective, blinded, randomized, and placebo controlled in design (15,18,19,21), whereas one was open labeled (20) and another uncontrolled (22). None of them was double blind in design.
Continuation of Gärtner et al. (15) trial.
Only phase 1 is described in this table.
Ab, antibody(ies); AE, adverse effects; fT3, free triiodothyronine; fT4, free thyroxine; HT, Hashimoto's thyroiditis; IU/mL, international units per milliliter; LT4, levo-thyroxine; Se, selenium; Seme, selenomethionine; TGab, thyroglobulin autoantibodies; TPOab, thyroid peroxidase autoantibodies; TSH, thyroid-stimulating hormone; Con, control group; Se–Se, received selenium in previous trial and continued with selenium; Se–0, received selenium in previous trial and continued with placebo; 0–Se, received placebo in previous trial and continued with selenium; 0–0, received placebo in previous trial and continued with placebo; U/S, ultrasonography.
First phase.
In Karanikas et al., plasma Se concentrations were reported in (μg/L), in contrast to previous studies.
NR, not reported; pts, patients; SF 12, standardized short form 12 protocol for subjective well-being; T/S, tolerability/safety; mos, months; ↓, decrease; ↑, increase.
In general, researchers attempted to evaluate the effects of Se supplementation on TPOab (15,18 –22) and TGab titers (15,18,20 –22), on thyroid echogenicity on ultrasound (15,20), on general well-being (15,18,19), and on estimates of immunological pattern (19) in patients with HT, by administering identical doses of Se in the form of either sodium selenite (200 μg) (15,19,20) or selenomethionine (200 μg) (18,21,22), both orally, once per day. The duration of supplementation ranged from 3 (15,19) to 12 months (22). A clear definition of HT was not stated in two studies (21,22), whereas the typical hypoechoic appearance of the thyroid on ultrasound was not prerequisite for HT diagnosis in another one (18). Plasma Se concentrations, at baseline and the end of the study, were determined only in two studies (15,19), whereas in another one (18) they were determined in a subset of participants. Immunoradiometric assays for the measurement of thyroid autoantibodies were applied in three studies (18,21,22), whereas in another three, chemiluminescence assays were used. All methodologies, thresholds, and/or coefficients of variations related to the determination of thyroid autoantibodies were validated and standardized. In two studies, mood and well-being before and after treatment was assessed using SF-12, a standardized 12-item short form, to survey health status (15,19). In individual randomized studies, groups, assigned to either Se or placebo, were comparable in age and TPOab titers, which were used as the primary randomization factors, resulting in a significant difference in TGab concentrations between groups. Time (years) from diagnosis of HT, which could serve as an indirect marker of the thyroidal damage and/or the reversibility of the disease, were not used either in the randomization process or in the presentation of results in any of the studies.
Except from one (19), all trials documented a significant decrease in TPOab titers after Se supplementation, evident from the first trimester of treatment. Those extended beyond this period reported a further decrease at 6, 9, or 12 months (18,20 –22), with either lower (21) or higher (22) rate of titers suppression compared with the first 3 months. Patterns of responders and nonresponders to treatment were documented in three trials (15,18,21), two of which reported greater decrease in those subjects with higher baseline TPOab titers (possibly reflecting highly active HT) (15,21). In one study (22), smoking was also identified as a predictor of unresponsiveness to Se supplementation. No correlation of Se concentrations with the response to treatment was documented in any of the trials. Indications of an improved U/S appearance of the thyroid was provided in one trial (15); however, this improvement was limited to those patients with a TPOab decrease below 50 IU/mL. This observation was not replicated in subsequent studies. Finally, the dose of 100 μg selenomethionine was only tested in a late phase of one trial, without evidence of efficacy in decreasing TPOab concentrations (21).
The majority of trials reported no significant change in TGab concentrations after Se supplementation (15,18,20,22), in contrast to one that reported a significant decrease (21). In general, baseline TGab concentrations were not comparable between groups and were considered by researchers as a less-specific marker of HT. No significant difference in T4, triiodothyronine, TSH concentrations, or LT4 replacement dosage was reported in any of the trials. Evidence of an improvement in mood and/or general well-being after Se supplementation was provided in three trials (15,18,19), yet using different and/or subjective methodology for assessment. The only study that investigated intracellular cytokine production in CD4+ and CD8+ reported no difference after Se supplementation. None of the studies reported calculation of GPx activity.
A clear description of the methodology applied to record and assess adverse outcomes and/or side effects was not provided in any of the studies. In general, all studies concluded that Se supplementation was safe and well tolerated. Gastric discomfort was recorded in a total of four patients [three in the trial by Mazokopakis et al. (22) and one in that by Turker et al. (21), all of them under selenomethionine supplementation. No correlation with treatment duration was possible.
Meta-analysis
The four randomized, controlled trials that were included in the meta-analysis reported data on 259 patients with HT who had been randomized to either Se supplementation (n = 136) or placebo (n = 123), along with LT4 treatment. T4 substitution was titrated to maintain TSH concentrations within normal limits in all randomized, controlled trials (Table 1). Study size varied from 36 to 88 participants (median = 67.5). Sodium selenite was used in two studies, in contrast to the other two, in which selenomethionine was used. The vast majority of the participants (96.5%) were women, and thus, special consideration on sex was neither feasible nor undertaken. The main results of the meta-analysis are summarized below.
TPOab titers after 3 months of Se supplementation
Participants who received Se supplementation demonstrated significantly lower TPOab titers compared with controls (four studies, random effects WMD: −271.09, 95% CI: −421.98 to −120.19, p < 10−4; Fig. 2). Substantial heterogeneity among studies was detected (I 2 = 62.6%, p = 0.046). No sign of publication bias was detected (Egger's test, p = 0.235). On the basis of the actual pharmacological substance used, participants taking selenomethionine demonstrated significantly lower TPOab titers compared with controls (two studies, random effects WMD: −277.22, 95% CI: −447.17 to −107.27, p = 0.001, I 2 = 27.9%; Fig. 2). In contrast, no significant difference in TPOab titers following sodium selenite was detected (two studies, random effects WMD: −225.42, 95% CI: −577.44 to 126.6, p = 0.209, I 2 = 83.5%; Fig. 2).
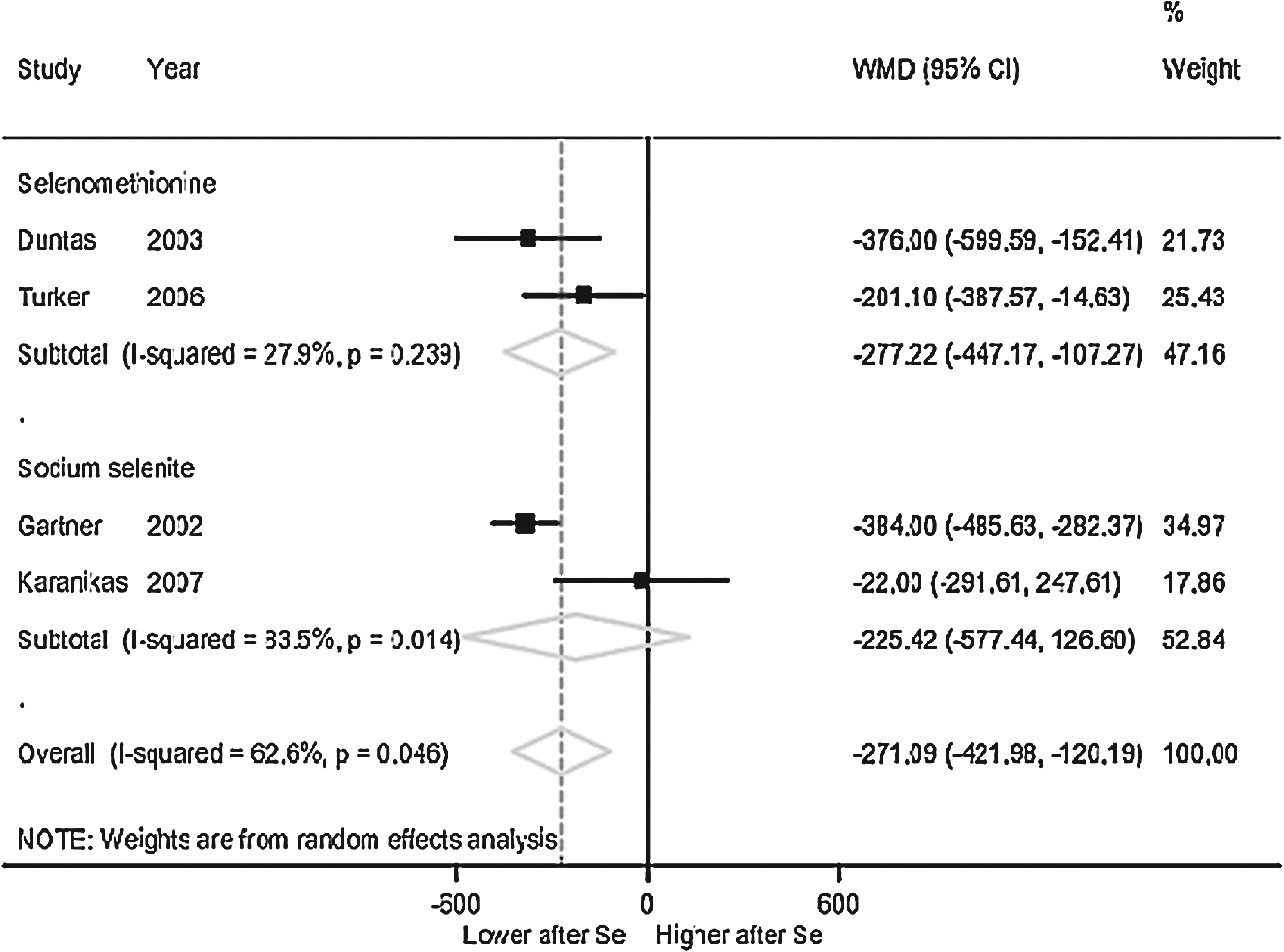
Weighted mean difference (WMD) in thyroid peroxidase autoantibodies titers after a 3-month period of selenium (Se) supplementation or placebo. Dotted line indicates combined WMD. Squares represent mean values of outcomes in a study, and their size is proportionate to the weight assigned to the study. Diamonds represent the pooled estimates of the outcome, and their horizontal dimension represents the relevant confidence interval.
Probability of an improvement in well-being and/or mood after Se supplementation
Participants assigned to Se supplementation had a significantly higher chance of reporting an improvement in well-being and/or mood compared with controls (three studies, random effects risk ratio: 2.79, 95% CI: 1.21–6.47, p = 0.016; Fig. 3). Substantial heterogeneity among trials was detected (I 2 = 75.6%, p = 0.017).
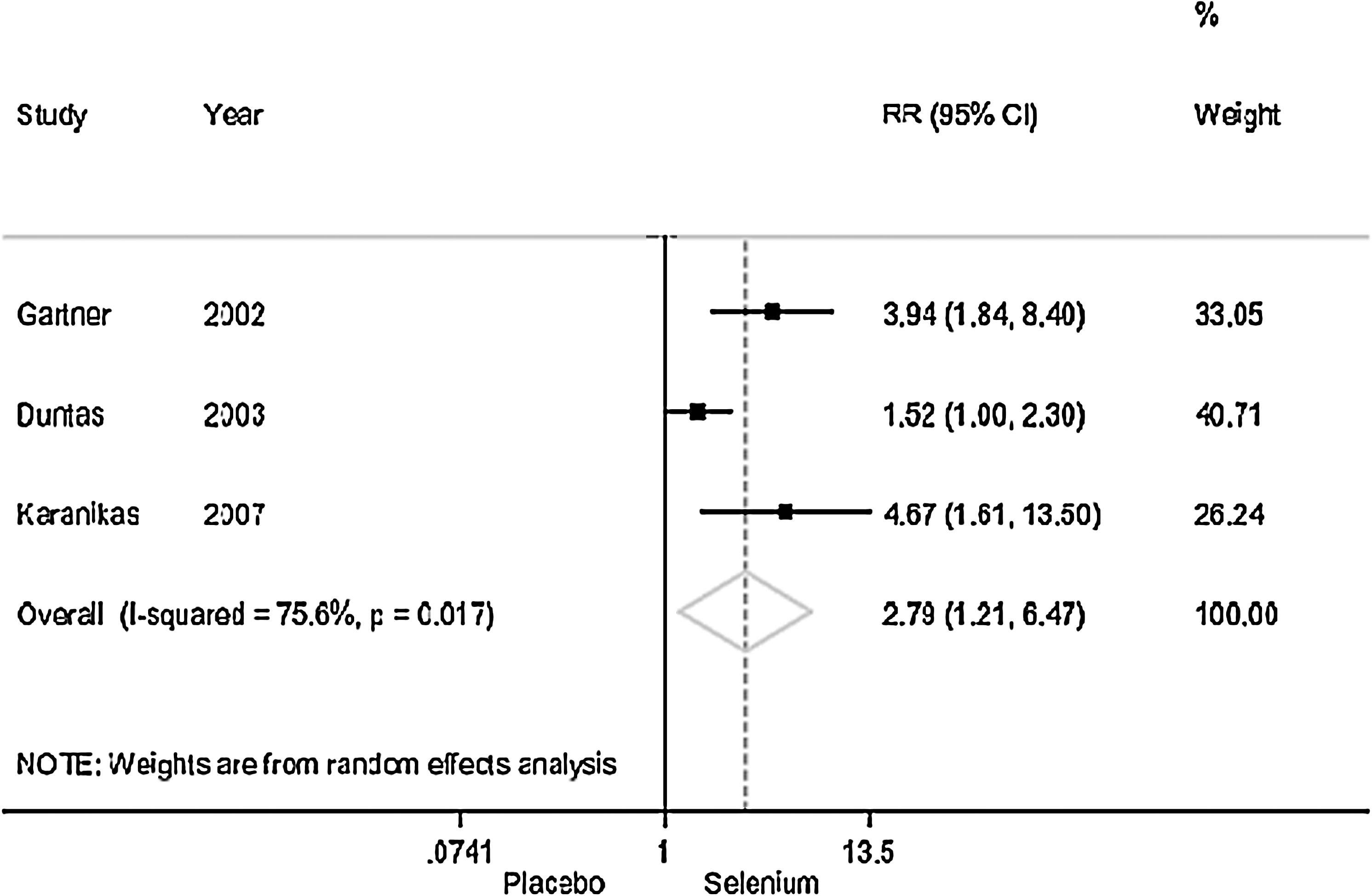
Probability of reporting an improvement in well-being and/or mood after a 3-month period of selenium supplementation or placebo. Dotted line indicates combined risk ratios. Squares represent mean values of outcomes in a study, and their size is proportionate to the weight assigned to the study. Diamonds represent the pooled estimates of the outcome, and their horizontal dimension represents the relevant confidence interval.
Analysis on TPOab titers after a 6-month supplementation as well as on U/S thyroid morphology was not undertaken, because of scarcity of evidence. Analysis on TGab titers was not undertaken, because groups were not comparable in them at baseline.
Discussion
The present systematic review and meta-analysis provided evidence that selenomethionine at a dose of 200 μg once per day is effective in reducing TPOab titers in patients with HT after a 3-month period, compared with placebo. In absolute numbers, this reduction equals ∼300 IU/mL. Efficacy of Se supplementation for >3 months could not be supported, because of lack of evidence from randomized, placebo-controlled trials. Patients assigned to Se supplementation had also a threefold higher chance of reporting an improvement in well-being and/or mood, compared with controls. No serious adverse effects were recorded after Se supplementation, with the exception of a limited number of gastric discomfort complaints associated with selenomethionine use. In general, there are no data demonstrating that Se treatment had any impact on the natural course of the disease.
Several observations should be taken into consideration when interpreting the results of the meta-analysis. First, the combined estimate of Se efficacy on reducing the TPOab titers was based on limited primary data, because only four randomized, placebo-controlled trials were identified and the final numbers of patients included in the meta-analysis was modest. Thus, the analysis could be underpowered or vulnerable to the distorting effect of a single biased estimate and further studies are needed to consolidate the findings. Second, the possibility of publication bias, namely the underreporting of studies with nonsignificant findings, should be taken into consideration, despite the negative result of the test for publication bias. Further, substantial heterogeneity was detected across trials. To explain this, the primary investigators attributed the differences to the nutritional supply of Se and iodine, patients' and regional characteristics, and TPOAb titers (32,33). Placing an alternative context for interpretation, Karanikas et al. suggested that different TPOAb titers reflect different immunological states, because they correlate with T-lymphocyte cytokine production patterns (34). Selenoprotein transport network and its defects have also been proposed to account for the difference in the efficacy of Se supplementation (35). Additionally, evidence from two trials (15,21) indicates a difference in response relative to TPOab baseline titers, suggesting that the higher the TPOab titers, the maximum response is to be expected. Finally, no firm conclusions could be drawn as to whether differences in serum Se concentrations could account for the observed inconsistency of the response across trials. Baseline Se concentrations were found to be similar between treatment and control groups across trials (15,18,19). Although the only study on subjects clearly sufficient for Se (19) showed no response in TPOAb titers, in contrast to those on subjects with mild insufficiency (15) or borderline sufficiency (18), many other reasons may have been implicated, such as difference in baseline TPOAb titers or iodine status. Moreover, serum Se concentrations do not reflect tissue concentrations (36). This observation, along with reported immunomodulatory effects of Se on cellular immune response (15,18,19), might explain the observed effect of Se even in a state of Se sufficiency, in accordance with the statement by Turker et al. (21) that “Se acts on Se-sufficient HT patients.” However, it should be taken into consideration the fact that iodine status was not determined in any of the studies. As for the effect of Se supplementation on mood status, this might be due to a possible Se effect on the degree of hypothyroidism. However, the latter could not be properly investigated, because LT4 dosage was not stable in any of the studies. Alternative explanations of this finding could be based on reports linking Se status and brain function. In fact, cognitive dysfunction has been recorded in subjects with low serum Se concentrations (37,38), whereas Se deficiency was shown to alter the turnover rate of brain monoamine neurotransmitters (39).
Regarding the differences between sodium selenite and selenomethionine supplementation, it has been suggested that the latter might be favored over the former (40); however, no firm conclusions from randomized, controlled trials in HT could be drawn yet.
Although this study demonstrated a decrease in TPOAb titers, the lack of outcomes with direct clinical implications should be underlined. Thyroid function was generally found unaltered after Se supplementation, no data on the demands in LT4 replacement therapy were recorded, and thyroid morphology, assessed by ultrasound, was investigated in only one study (15). TPOab titers are considered as a surrogate marker, an intermediate outcome of limited clinical importance in the course of HT, with the exception of pregnancy (29). Thus, although Se holds a satisfactory safety/tolerability profile, meaningful clinical outcomes should be demonstrated before Se supplementation can be routinely recommended in HT.
Thus, future studies investigating the efficacy of Se supplementation in HT could address the following issues: (i) response to treatment on the basis of the years from diagnosis (new-onset HT) and baseline TPOAb titers (highly active HT), which could potentially identify “ideal” patients who would benefit most from Se supplementation; (ii) inclusion of direct clinical outcomes, such as thyroid morphology on ultrasound, histomorphology assessed by fine-needle aspiration, and LT4 treatment demands, to gain further insight on Se mechanism of action or the reversibility of thyroidal damage after Se supplementation; (iii) assessment of Se efficacy in preventing or delaying progression to later stages of HT (from euthyroid HT to subclinical and clinical HT); (iv) standardized approaches to assess mood improvement; and (v) extension of follow-up in a double-blinded, randomized setting, to secure validity of the findings.
Footnotes
Acknowledgments
The authors are very grateful to Prof. Leonidas Duntas (University of Athens) for his thoughtful suggestions during preparation of the manuscript. The authors thank Dr. Georgios Karanikas (Departments of Nuclear Medicine and Pathophysiology, Medical University of Vienna, Austria) and Dr. Elias E. Mazokopakis (Department of Internal Medicine, University Hospital of Heraklion, Greece), who both kindly provided requested information on their publications. Funding: none.
Disclosure Statement
The authors declare that they have nothing to disclose.