
Abstract
Background:
Iodine deficiency is a major public health problem throughout Africa. Although salt for human consumption is said to contain adequate amounts of iodine in Uganda, iodine intake may not be optimal. We undertook a field study to assess the adequacy of iodine nutrition in western Uganda using on-site measurement methods of neonatal thyroid stimulating hormone (TSH) levels as recommended by the World Health Organization (WHO) for monitoring the degree of iodine deficiency during pregnancy.
Methods:
The study design consisted of a prevalence study using the percentage of newborns between the ages of 3 and 7 days with TSH >5 mIU/L, measured with a point-of-care immunochromatographic TSH assay, as a surrogate marker of iodine deficiency. Five districts in western Uganda were selected for study on the basis of a past history of iodine deficiency. One thousand seventy-eight newborns from the five districts were sequentially enrolled in each separate district and tested between July 2007 and January 2008.
Results:
The prevalence of TSH levels >5 mlU/L ranged from 20% to 32%. Neonates tested on or before the age of 3 days were more likely to have a TSH level >5 mlU/L than those tested beyond the age of three days (28.2% vs. 18.7%, p < 0.001).
Conclusions:
Assessing neonatal TSH levels in developing countries with a TSH assay method suitable for field use can be successfully used to screen for congenital hypothyroidism and to indirectly assess a population's iodine status. Based on the percentage of neonates with TSH values >5 mIU/L, presumptive iodine deficiency persists in western Uganda. This finding suggests that continued monitoring of iodine nutrition in the area surrounding the Rwenzori Mountains in Uganda and Congo is needed. Due to the progressive fall in the percent of TSH values >5 mIU/L from day three to day five of life, we conclude that TSH measurement earlier than day five of life in newborns at risk for iodine deficiency may be misleading. Guidelines for the use of neonatal TSH to monitor iodine nutrition should specify that TSH measurement take place no earlier than day five of life.
Introduction
Methods currently used to assess iodine nutrition include determining community prevalence of goiter in children older than age 5, measuring iodine excretion among school-aged children (9), and determining the percent of neonatal TSH values between 5 and 20 mIU/L (10). The accurate determination of goiter prevalence requires ultrasonography, with its attendant need for expensive electrical equipment and trained personnel. Additionally, normative data for thyroid size in Ugandan school children require ultrasonic examinations of a substantial number of subjects across a broad range of socioeconomic and demographic strata (11). Iodine excretion for national surveys in sub-Saharan Africa is measured by a central WHO laboratory in South Africa using random urine samples collected by designated individuals in multiple countries. The results are expressed as the ratio of iodine to creatinine. In areas where there is malnutrition, creatinine levels are artefactually low, resulting in falsely elevated values for iodine to creatinine ratios (12). Additionally, urine specimen collection is susceptible to tampering, as collection methods do not require documentation of urine sample integrity. The use of neonatal TSH samples has generally not been regarded as practical for rural and remote regions of sub-Saharan Africa.
Recently introduced methods for point-of-care measurement of TSH, however, provide an alternative method to the use of centralized laboratories for newborn TSH determination. The present study was undertaken to assess the adequacy of iodine nutrition in western Uganda using an on-site method for measuring neonatal TSH levels and to evaluate in the field the use of point-of-care TSH measurement for identifying neonatal TSH values >5 and 20 mIU/L.
Methods
Procedures
Five districts in western Uganda were selected for study on the basis of a past history of iodine deficiency (Fig. 1). One thousand seventy-eight newborns were sequentially enrolled by district and tested between July 2007 and January 2008. Mothers of infants, ages 2–7 days, were contacted immediately after delivery or at the time of first immunization, provided with a detailed explanation of the nature of the study procedures and the importance of iodine for normal childhood growth and development, and invited to provide consent to collect a small quantity of blood from their infant by means of a heel stick. Mothers provided either a signature or thumb print to indicate consent to participate in the study. The research protocol was approved by the Uganda Council for Science and Technology and by the Institutional Review Board of the International Hospital, Kampala, Uganda. For each infant tested, name, place of birth, birth date, recorded birth weight, mother's name, age, and significant details associated with the pregnancy or birth (e.g., delivery by cesarean section, twinning, medical complications, infection with malaria or HIV during pregnancy, recent immigration from the eastern region of the Democratic Republic of Congo or residence in a refugee camp in Uganda due to civil war in Eastern Congo at the time of delivery) were recorded.

Map of Western Uganda showing location of districts studied.
U.S. Food and Drug Administration approved, self-performing, semi-quantitative, disposable immunochromatographic TSH assays (OneStep Whole Blood Neonatal TSH) were purchased from Syntron Bioresearch, Carlsbad, California. Tests were performed by local medical personnel, including licensed medical laboratory technicians, clinical officers, nurse midwives, and district medical and surgical officers, following manufacturer's instructions. All personnel who performed TSH tests had previous experience conducting immunochromatographic tests for HIV antibody detection, which are identical in format, performance, and interpretation to the TSH assays used in this study. Control tests, using TSH of known concentration in phosphate-buffered saline provided by the test manufacturer, were performed at least once a day or after completion of 10 tests to ensure appropriate test calibration.
Each newborn was initially screened for TSH >5 mIU/L. To minimize the effects of the neonatal surge in TSH secretion, screening was conducted on day 2–7 of life. Infants found to have TSH >5 mIU/L were then screened for TSH >20 mIU/L. If the initial test indicated TSH >20 mIU/L, a second test was performed at least 24 hours later. The diagnosis of primary hypothyroidism was based on the finding of two TSH values >20 mIU/L. Neither mothers nor infants were exposed to iodine-containing antiseptic solutions during delivery or in the postpartum period.
Statistical analysis
A minimum of 200 infants were tested in each district. This number of subjects was based upon previous studies in Thailand which showed that 200 individual neonatal TSH values obtained sequentially from defined geographic areas were sufficient to detect effects with relative odds of disease 2.0 or greater (13). Data analyses were conducted using SPSS (Version 16.0 for Windows, Chicago, IL). Standard descriptive statistics were used to describe maternal and infant demographics by site. Pearson χ2 tests and one-way analysis of variance were used to compare demographic characteristics across the five sites. Multiple logistic regression was used to identify factors associated with TSH >5 mIU/L.
Results
Demographic characteristics of infants and their mothers by district are displayed in Table 1. No significant differences on these characteristics were detected for sex of neonate, mother's age, parity, or birth weight. Sample sizes per district were roughly equal, ranging from 200 to 232.
The prevalence of TSH levels >5 mlU/L ranged from 20% in Bundibugyo to 32% in Kasese (Fig. 2). Presumptive evidence for iodine deficiency, defined as 20%–40% of infants between 3–7 days of age with TSH >5 mIU/L, was present in each of the five districts studied. No cases of congenital hypothyroidism were detected. The prevalence across districts did not differ significantly except for Kasese (p = 0.011), where local non-iodinated salt is produced.
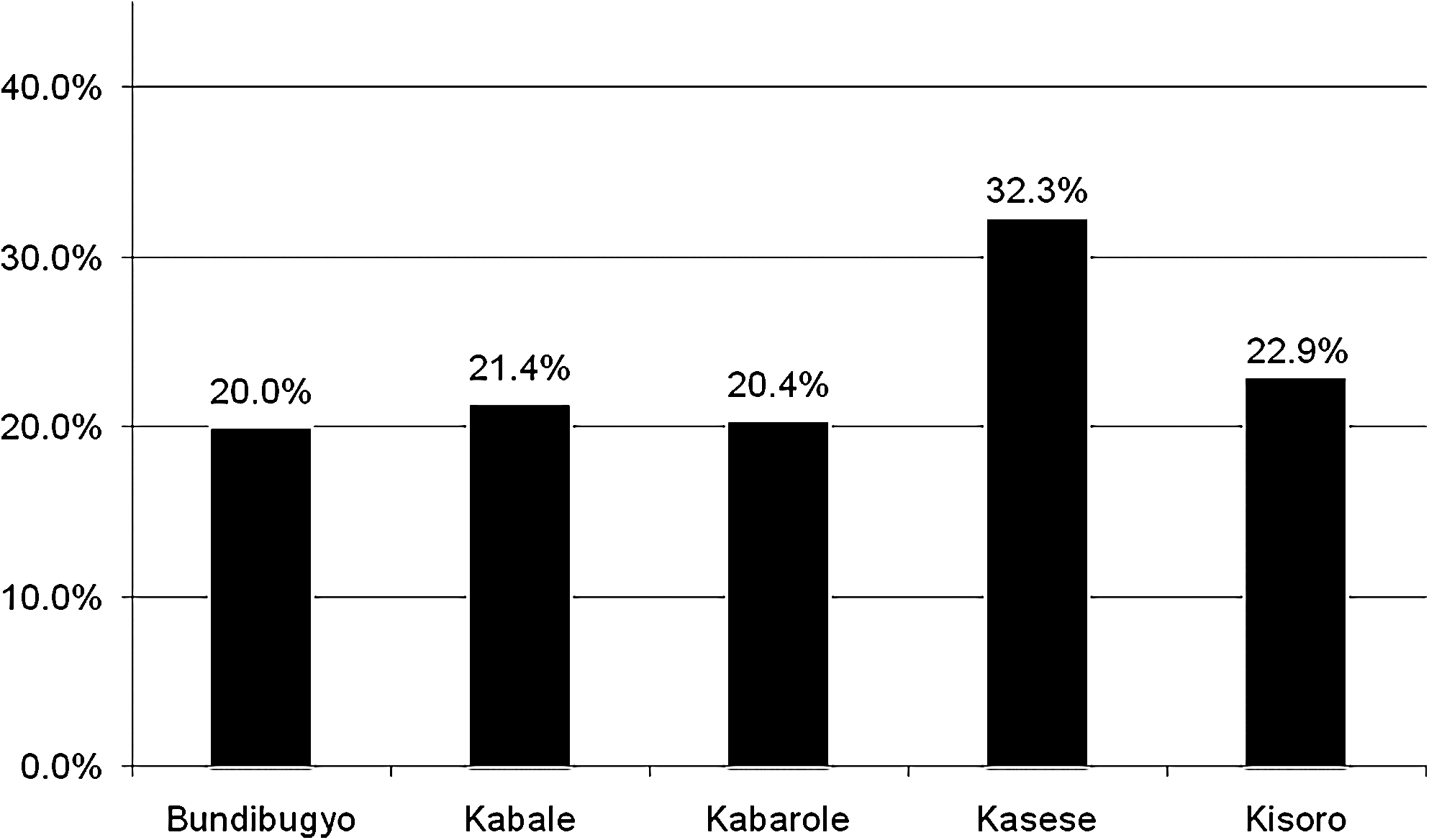
Prevalence of presumptive iodine deficiency by district: % TSH >5 mlU/L.
A multiple logistic regression analysis was conducted, with TSH >5 mlU/L modeled as a dichotomous outcome and delivery by C-section, maternal age, parity, birth weight, district of residence, birth in hospital, and age at TSH testing as predictor variables (results are shown in Table 2). In addition, a series of age-stratified secondary analyses were conducted (with individual models for TSH testing at 3, 4, 5, 6, and 7 days of life plus one that aggregated days 5 through 7 of life) using the same predictor variables except for age. The stratified analyses did not yield significant associations among included predictor variables and TSH >5 mIU/L, potentially due to limited statistical power associated with the smaller sample sizes. Using the aggregate data set, residence in the Kasese district remained a predictor of increased risk of presumptive iodine deficiency whereas birth in a hospital and age at TSH testing were associated with reduced risk of iodine deficiency. All other variables in included in the logistic model failed to demonstrate a significant association with a TSH level >5 mlU/L.
Figure 3 depicts the percent of TSH >5 mIU/L by the age of the neonate in days at the time of testing. Rates decline by date, from a high of 27% on day three to a low of 9% on day 6. To assess the differences in the percent of TSH >5 mIU/L by day, results were collapsed into those collected on or before age 3 days versus those collected on day 4 or later. Neonates tested on or before the age of 3 days were significantly more likely to have a TSH level >5 mlU/L than those tested beyond age 3 days (28.2% vs. 18.7%, p < 0001).
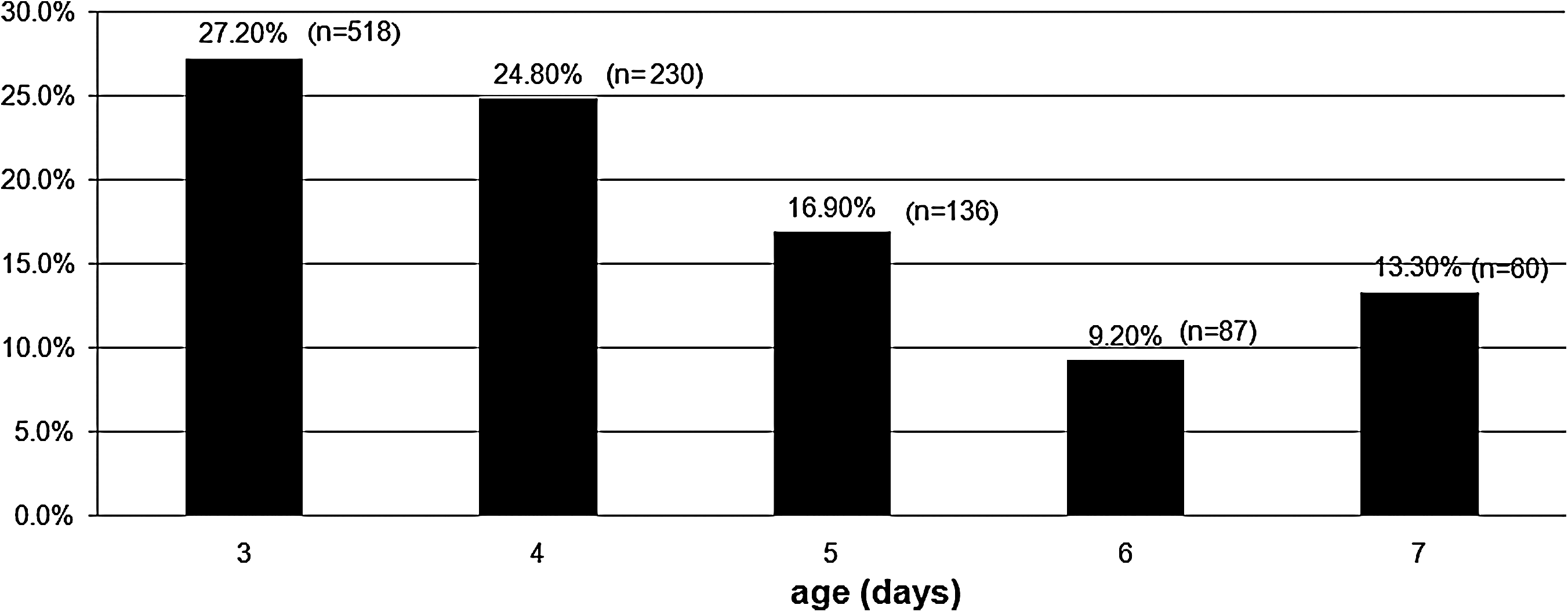
Prevalence of presumptive iodine deficiency by age: % TSH >5 mlU/L.
Discussion
At the time of birth, there is a surge in TSH secretion as a result of changes in the ambient temperature to which the neonate is exposed as well as other stressors associated with delivery. By 72 hours of life, the transient TSH elevation has resolved; accordingly, elevations in TSH found after day 3 of life have an increased positive predictive value for the diagnosis of congenital hypothyroidism (14). Current recommendations from the American Pediatrics Society, American Thyroid Association, and the Lawson Wilkins Pediatric Endocrine Society recommend TSH testing between 48 and four days of age to screen for congenital hypothyroidism in iodine sufficient populations (15). According to WHO/United Nations Children's Fund/International Commission for the Control of Iodine Deficiency Disorders criteria, presumptive evidence for iodine deficiency is present in the five districts we studied in western Uganda (9). Our data show, however, that a neonate's age at TSH testing has a significant effect on the likelihood of the result being >5 mIU/L before the fourth day of life. This finding occurs after the physiologic TSH surge at birth has resolved (16). If TSH were measured between days 5 and 7 of life in this population, 1 of the 5 districts and not 4 of the 5 districts studied would have shown a percentage of TSH elevations that are associated with long-term adverse development effects due to iodine deficiency. Previous studies have shown that iodine deficiency in populations with 20.0%–39.9% neonatal TSH values >5 mIU/L is associated with impaired growth and development, including a decrease of 10–15 intelligence quotient points, whereas populations with 3.0%–19.9% of neonatal TSH values >5 mIU/L do not show evidence of iodine deficiency (17). Consequently, the date on which neonatal TSH measurement takes place can have significant public health and health resource allocation implications.
The use of neonatal TSH values as an index of iodine nutrition is based on observations from neonatal screening programs for congenital hypothyroidism. These screening programs have been established in industrialized countries where significant degrees of iodine deficiency do not exist. As a result, the effect of age of TSH testing in an iodine-deficient region and the use of neonatal TSH values to assess iodine nutrition have not been systematically previously evaluated. Previous observations in Ethiopia (18) Sicily (19), Argentina (12), Kuwait (20), Turkey (21), Nepal (22), and Thailand (23), all of which have populations that experience iodine deficiency, are consistent with the findings reported here. A recent report on iodine intake and neonatal TSH values in Ireland, an iodine sufficient region, concluded that the trend in the mean TSH value of a population that has adequate iodine intake is a more sensitive indicator of changes in iodine intake than the % of TSH values >5 mIU/L (24).
These study findings illustrate the limitations of using the commercial availability of iodized salt to supplement iodine intake as an exclusive method to ensure adequate iodine nutrition. Kasese District, which has the highest prevalence of TSH >5 mIU/L of the five districts studied in western Uganda, is a site of local noniodized salt production, and locally produced salt is preferred to store-bought salt for a number of cultural and economic reasons. Previous attempts to add iodine have not been successful due to chemical instability of iodine in the sodium salts contained in Kasese salt. Another factor that affects salt and iodine consumption is Ugandan public health policy, which recommends that people limit their salt intake to decrease the risk of hypertension. Thus, although almost all commercial salt available in Uganda is iodized, there are a number of socioeconomic and public health reasons as to why this iodized salt is not always used. These findings underscore the importance of using a variety of iodine delivery systems, such as iodized oil delivered orally or parenterally, in addition to iodized salt for culinary use to ensure adequate iodine intake.
Although birth in hospital was associated with a decreased risk of TSH >5 mIU/L, the effect of age on likelihood of TSH >5 mIU/L was independent of birth site. The most likely explanation to account for the decreased risk of TSH >5 mIU/L for births in hospital is that women with access to a hospital had an increased intake of iodine during their pregnancy. In contrast to findings reported from Australia, where percentages of TSH >5 mIU/L was 7.1% for babies born by cesarean compared with 4.3% for babies born vaginally (25), we found that mode of delivery was not a significant risk factor for TSH >5 mIU/L.
A recently published comprehensive review of neonatal TSH screening for monitoring iodine status in populations identified mode of delivery, anatomic site and neonatal age, specimen type, exposure to iodine-containing antiseptics, and TSH assay methodology as potential independent variables that can affect TSH measurement (26). An additional factor that can affect neonatal TSH concentration is concomitant illness. The present study did control for blood collection site, specimen type, TSH assay method, and iodine exposure and did assess the potential effect of mode of delivery on TSH, but did not evaluate the effect of undercurrent illness on neonatal TSH results. Prematurity and neonatal illnesses are known to affect newborn TSH secretion (27). The effects of other illnesses commonly encountered in western Uganda, such as maternal HIV infection or malaria, on neonatal TSH is unknown. It is possible that these may result in elevations in TSH during the neonatal period. Another potential limitation of the present study is infant age as reported at the time of testing. For neonates born at home, the infant's age was provided by the mother. The reliability of this information was not independently validated, and it is possible that an incorrect day of birth could have been reported or recorded. Selection basis in the infants tested may also represent a potential source of error. Infants born at home were tested at weekly immunization clinics. It is possible that attendance at these clinics during the first week of life may have introduced a bias into the subject selection process. Since consistent results were obtained independently among the five districts studied, we believe that the possibility of these potential sources of error substantially altering our findings is unlikely.
This study demonstrates that point-of-care TSH measurement is a practical method for use in developing countries to both screen for congenital hypothyroidism and assess a population's iodine status. Based on the percentage of neonates with TSH values >5 mIU/L, presumptive iodine deficiency continues to exist in western Uganda. Due to the increased frequency of TSH >5 mIU/L in infants born in iodine-deficient regions and the progressive fall in the percent of TSH values >5 mIU/L from day 3 to day 5 of life, we conclude that TSH measurement earlier than day 5 of life in newborns at risk for iodine deficiency may be misleading. Consequently, International Commission for the Control of Iodine Deficiency Disorders/United Nations Children's Fund/WHO Guidelines for the use of neonatal TSH to monitor iodine nutrition should specify that TSH measurement take place no earlier than day 5 of life.
Disclosure Statement
J.E. has developed a point-of-care immunochromatographic TSH assay. The TSH assay used in this study is not the assay developed by the author. The author has no financial or commercial relationship with the company that manufactures the TSH assay used in this study.
J.F., A.N., I.C., and S.A. declare that no competing financial interests exist.