
Abstract
Background:
The association between autoimmune thyroiditis (AIT) and thyroid cancer is still not clear despite many previous reports. This study investigated whether serologic thyroid antibodies are predictive of thyroid cancer in patients with thyroid nodules.
Method:
We retrospectively reviewed records of patients with thyroid nodules evaluated by ultrasonography-guided fine-needle aspiration cytology at our institution between January 2006 and December 2008. Thyroid autoimmunity was assessed by measuring thyroglobulin antibody (TgAb) and thyroid peroxidase antibody (TPOAb). The final outcome deciding a benign or malignant status involved a combination of cytology and histology.
Results:
Of the 1638 patients, malignant nodules had a higher rate of positive TgAb (30.8% vs. 19.6%; p < 0.001) and elevated thyrotropin (TSH) levels (2.5 ± 2.8 mIU/L vs. 2.1 ± 2.0 mIU/L; p = 0.021) than benign nodules. The rate of positive TPOAb was not higher in malignant nodules, although both TPOAb and TgAb were well correlated with TSH levels and histological AIT. In the multivariate analysis, a positive TgAb was significantly associated with thyroid cancer (odds ratio [OR] = 1.61, 95% confidence interval [CI] 1.12–2.33) with upper tertile of normal range of TSH levels (OR = 1.72, 95% CI 1.12–2.63) and above normal range of TSH levels (OR = 1.98, 95% CI 1.06–3.70).
Conclusion:
We report for the first time that a positive serum TgAb test was an independent predictor for thyroid malignancy in thyroid nodules along with serum TSH levels regardless of the presence of AIT. Our results suggest that TgAb measurement could give additional information for predicting malignancy in cytologically indeterminate thyroid nodules in conjunction with clinical risk factors and TSH levels.
Introduction
The gold standard of diagnosis for thyroid nodules is fine-needle aspiration (FNA). However, FNA alone is insufficient to detect cancer not only because of inadequate cytology (5–15%) but also because of cases of follicular neoplasm (15–25%) in which only surgery is diagnostically conclusive (8). Therefore, other factors in addition to FNA should be considered to predict malignancy preoperatively. Traditionally, clinical factors such as age, gender, nodule size, and radiation history are considered meaningful for predicting thyroid malignancy (9).
Another proposed risk factor is autoimmune thyroiditis (AIT), and many reports have indicated the relationship between AIT and thyroid cancer (10 –15). However, this relationship remains controversial, because the results of subsequent reports did not support this association (16 –18). Although the relationship was first noted from surgical findings, there may have been a selection bias because the cases were confined to highly malignant cases requiring operation, and there was some difficulty in discriminating thyroiditis conjoined with malignant tissue and true AIT (19). Also, the results from a few large clinical cohorts opposed the association (16,17).
Recently, a few reports presented serum thyrotropin (TSH) as a possible reliable predictor of thyroid malignancy (20,21) and also suggested that AIT could be a risk factor for thyroid cancer as it is the most common cause of elevated TSH (21,22). Although thyroid peroxidase antibody (TPOAb) is reported to be dependently associated with thyroid cancer (20), little attention has been paid to whether measuring other thyroid autoantibodies, in addition to TSH, could help predict malignancy in subjects with thyroid nodules. Therefore, this study was undertaken to determine if there is an association of malignancy in thyroid nodules with thyroid autoantibodies, or serum TSH, or Hashimoto's thyroiditis as diagnosed by histopathology.
Subjects and Methods
A total of 2088 patients with thyroid nodules who received US-guided FNA at our institution between January 2006 and December 2008 were reviewed retrospectively. After excluding patients taking thyroid hormone or antithyroid drugs, and with inadequate cytology, only those with normal free thyroxine (FT4) levels were included (Fig. 1). In total, 1725 patients with thyroid nodules were investigated.

The flow for final diagnostic outcome.
FT4 and TSH were measured by commercial immunoradiometric assays (FT4 RIA kit and TSH IRMA kit; Immunotech, Vaudreuil-Dorion, Canada). Thyroglobulin antibody (TgAb) and TPOAb were measured by radioimmunoassay (RIAZENco TgAb and TPOAb kits; ZenTech S.A., Liège, Belgium), with a negative range of <30 IU/mL and a positive range of >50 IU/mL in both assays. The analytical sensitivity (minimal detective concentrations based on calibrated curve) of TgAb was 6 IU/mL and of TPOAb was 1.3 IU/mL, whereas the functional sensitivity (maximum 20% interassay variance) of TgAb was 15 IU/mL and of TPOAb was 20 IU/mL.
After the thyroid gland was assessed by high-resolution US, FNA was done under US guidance using a 23-gauge needle for the detected nodules except for complete cysts. Cytological findings were classified as nondiagnostic (class I), benign (class II), indeterminate (class III), and suspicious or frank malignant (class IV) according to the standard criteria (21).
Among 1307 patients diagnosed as class II in FNA cytology (FNAC), only three patients underwent surgery (because of cosmetic problems) and all three were confirmed as benign (Fig. 1). FNAC results of 142 patients showed class III and 55 underwent surgery; of these, histology results confirmed 29 cases as benign and 26 as malignant. The remaining 87 patients without definite cytological results in class III were excluded from the study because of no confirmed data (Fig. 1). Among the 276 patients diagnosed as class IV in FNAC, 184 patients underwent surgery, which demonstrated 178 malignant cases and 6 benign cases. The other 92 patients within class IV did not undergo surgery because of patient refusal, request for second opinion, and loss to follow-up.
The final diagnosis of benign or malignant nodules was determined using combined results of FNAC and postoperative histology. Finally, after the exclusion of 87 subjects with no confirmed results in class III, 1638 patients (1342 with benign and 296 with malignant results) were investigated (Fig. 1).
We evaluated and compared the clinical parameters such as age, sex, nodule size, singularity, thyroid autoimmunity, and TSH in both benign and malignant groups. In addition, we investigated whether thyroid autoantibody could predict malignancy and was associated with TSH. Pathological Hashimoto's thyroiditis was defined when specimens showed panthyroiditis with diffuse lymphocyte infiltration. The study was approved by our institutional review board.
Statistical analysis
Data were expressed as mean ± standard deviation. The comparison of two continuous variables was done by unpaired t-test and categorized ones by χ 2 test or Fisher's exact test. Univariate and multivariate logistic regression analyses were performed to evaluate the association between malignancy and risk factors such as age, sex, solitary nodule, nodule size, and TSH as a categorized variable. A p-value of <0.05 was considered statistically significant. All analyses were performed using SAS (version 8.2; SAS Institute, Cary, NC).
Results
Clinical characteristics
Among the 1638 patients, thyroid cancer was histologically confirmed by surgery in 204 patients (Fig. 1). The results included 201 papillary thyroid cancer (PTC; 177 classic variant, 22 follicular variant, and 2 combined), 1 lymphoma, and 2 mixed carcinoma (1 papillary carcinoma with medullary thyroid cancer and 1 papillary carcinoma with poorly differentiated carcinoma). Regarding diagnosis by FNA in the study population, sensitivity was 100%, specificity was 33.3%, positive predictive value was 96.7%, and negative predictive value was 100%.
As shown in Table 1, there was no difference in sex ratio between patients with benign and malignant nodules. However, patients with malignancies were relatively younger (48.4 ± 12.6 years vs. 51.4 ± 12.4 years; p < 0.001), had smaller nodules (1.2 ± 0.8 cm vs. 1.5 ± 1.0 cm; p < 0.001), and had positive TgAb more frequently (30.8% vs. 19.6%; p < 0.001). There was no difference in the rate of positive TPOAb (16.2% vs. 17.7%; p = 0.279). And the rate of Hashimoto's thyroiditis presented in histology was not different between malignant and benign nodules (16.2% vs. 21.1%; p = 0.470).
Data represent mean ± standard deviation or number (percentage).
Benign was composed of 1304 cytology and 38 histology results and malignancy was composed of 92 cytology and 204 histology results.
Measured in 1046 subjects.
Measured in 1536 subjects.
Measured in 38 benign and 204 malignant specimens.
Analysis of thyroid autoantibodies
Both positive TPOAb and TgAb were closely correlated with chronic lymphocytic thyroiditis as noted by histopathology (χ 2, p < 0.001; χ 2, p < 0.001, respectively). Also, there were linear correlations of both TgAb (r = 0.27, p < 0.001) and TPOAb titers (r = 0.27, p < 0.001) with TSH levels when antibody titers were categorized into absent, normal, and elevated titers (defined positive) (to < 30, 30–50, and > 50 IU/mL).
We also evaluated the rate of malignancy according to the presence or absence of TgAb or TPO antibodies and for three category levels of TgAb or TPOAb titers (Fig. 2). The prevalence of malignancy was significantly higher in the TgAb-positive group than either the undetectable (26.4% vs. 17.1%, p = 0.007) or normal group (26.4% vs. 11.1%, p = 0.002). When we evaluated TgAb by dividing the positive (N = 227) and negative (N = 819) (which includes absent and normal TgAb titer) groups, the TgAb-positive group had a higher cancer rate than the TgAb-negative group (26.4% vs. 16.5%, p = 0.001). In contrast, there was no association or trend between positive TPOAb tests or titers and the prevalence of thyroid cancer.
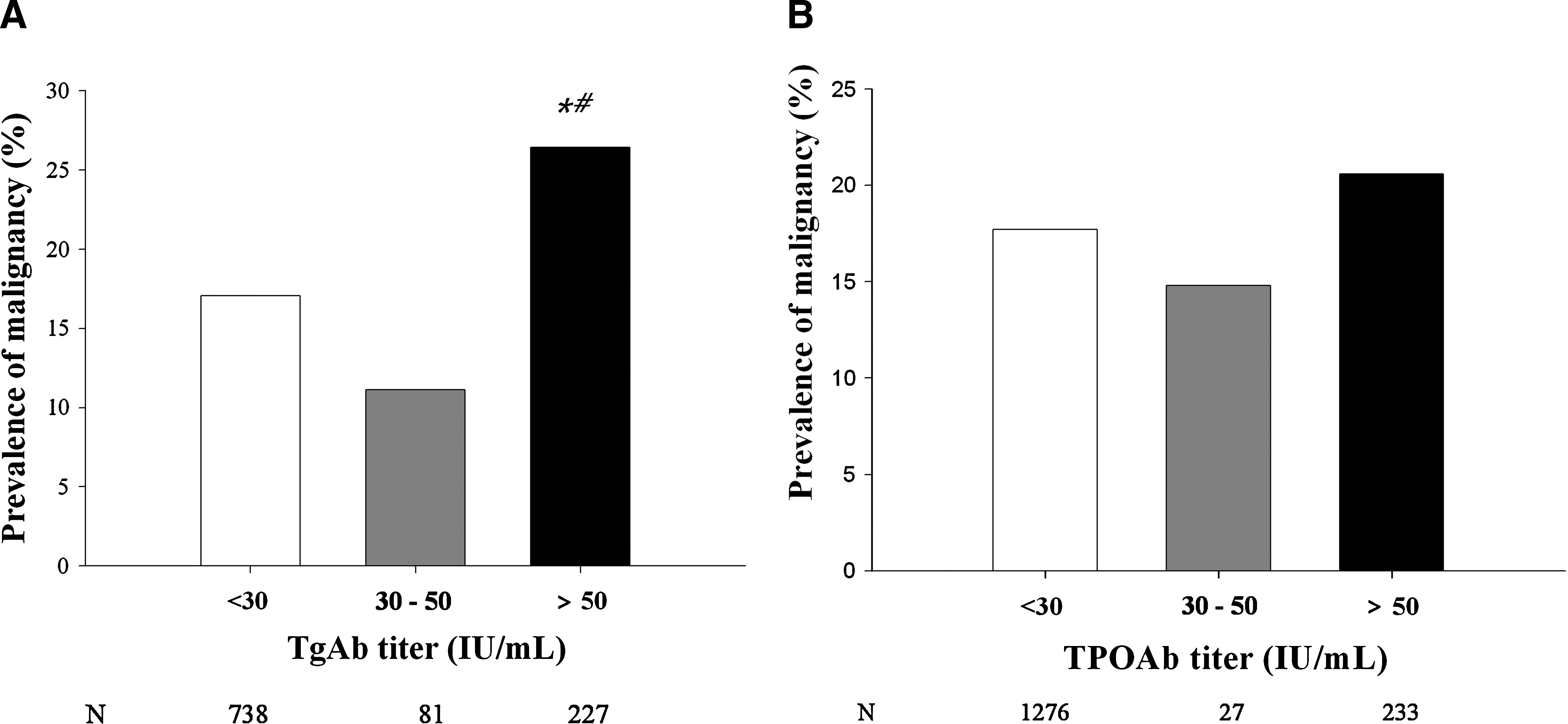
Prevalence of malignancy according to thyroglobulin antibody (TgAb) (
Univariate and multivariate analyses with thyroid malignancy
In univariate analysis, related factors with thyroid cancer were age (OR = 0.98, 95% CI 0.97–0.99), size (OR = 0.72, CI 0.61–0.85), and TgAb (OR = 1.80, CI 1.29–2.58).
Subsequently, TSH levels were divided into quintiles such as below normal (Q1, < 0.17 mIU/L; subclinical hypothyroidism), above normal (Q5, ≥ 4.06 mIU/L; subclinical hyperthyroidism), and within normal ranges divided into tertiles of similar size (Q2, 0.17–1.17 mIU/L; Q3, 1.18–2.01 mIU/L; Q4, 2.02–4.05 mIU/L). The prevalence of malignancy was increased according to TSH levels categorized into quintiles; 11.4%, 14.7%, 18.0%, 20.0%, and 24.7% (p-value for trend = 0.002; Fig. 3).

Prevalence of thyroid malignancy according to serum thyrotropin (TSH) concentration. The dashed vertical lines represent the normal reference range of TSH levels. Subjects with normal range of TSH concentrations were divided into three groups of similar size. The total number of patients (N) in each group is given beneath the graph. *p = 0.032, **p = 0.005 compared with lower normal TSH (Q2; 0.17–1.17 mIU/L); p-value for trend = 0.002.
In multivariate logistic regression analysis, the prevalence of thyroid cancer was significantly associated with positive TgAb (OR = 1.61, 95% CI 1.12–2.33) in addition to elevated TSH levels (TSH: 2.02–4.05 mIU/L, OR = 1.72, 95% CI 1.12–2.63; TSH: ≥ 4.06 mIU/L, OR = 1.98, 95% CI 1.06–3.70), decreased age (OR = 0.98; 95% CI 0.96–0.99), and decreased nodule size (OR = 0.74, 95% CI 0.61–0.91) (Table 2).
The adjusted odds ratio, 95% confidence interval, and p-value for each variable are displayed.
Discussion
Our study showed that positive TgAb in thyroid nodules could predict thyroid cancer independent of TSH levels. This study is remarkable because it is the first study that reports TgAb as a predictive marker for thyroid cancer.
Although several studies reported there was no relationship between thyroid autoantibodies and thyroid cancer, they were not focused on TgAb. Boelaert et al. evaluated the relationship by analyzing only TPOAb and not TgAb (20). Other studies (18,23) evaluated the association with malignancy by considering positive thyroid autoantibodies as a whole, including TPOAb and TgAb, but associations with individual antibodies were not considered.
Historically, the relationship of AIT with thyroid cancer has long been speculated. Since Dailey et al. (10) reported that there was more lymphocytic thyroiditis in malignant nodules than benign nodules by a retrospective study based on surgical specimens, there has been many subsequent reports supporting the association (10 –15). The proposed oncogenic effect of AIT, especially on PTC, is supported by the observation that immunohistological markers of PTC, such as cytokeratin 19 (24), p63 (25), and rearranged during transfection/papillary thyroid carcinoma (RET/PTC) rearrangements (26), are also found in tissues with AIT, although there are disputes about the role of RET/PTC rearrangements in the tumorigenesis of thyroiditis (27). Meanwhile, many studies have opposed the association of AIT with malignancy. Especially, two large prospective studies with a follow-up over 10 years failed to reveal higher incidence of thyroid cancer in goiters with AIT compared with goiters without AIT (16,17,28). Moreover, Rago et al. also reported that there was no association between thyroid autoimmunity and malignancy in a study conducted on indeterminate cytology (18).
Our study also showed that AIT was not predictive of malignancy. It is because TPOAb, a more specific serum marker of AIT (29), showed no association with malignancy and because histological AIT was not common in malignant specimens. Therefore, our study results could be interpreted that TgAb itself is a predictor of thyroid cancer, not a reflecting marker of AIT.
In thyroid cancer, the importance of TgAb measurement was stressed because it could interfere with measurement of thyroglobulin levels (30). In thyroid malignancy, the prevalence of TgAb, 10–30% (31,32), is much higher than that of normal population and decreases subsequently after cancer treatment in 3 years (33). So, some studies suggest that persistent increases in TgAb titers could be an early relapse marker as a thyroglobulin surrogate (34,35). These findings imply that TgAb elevation is present before surgery in malignant nodules.
In humans, thyroglobulin has only four to six epitopes that are recognized by B cells among the 40 known epitopes (36). Recently, thyroglobulin produced by thyroid cancer was demonstrated to have epitopes different from those involved with AIT autoantibodies (37). Therefore, it is possible that occult thyroid cancer that develops in normal thyroid or AIT stimulates chronic immunologic responses and produces new or more TgAb against thyroglobulin released by increased tumor cell mass in proportion to TSH levels. This could explain the mechanism of association between positive TgAb and malignancy.
Concerning TSH, its role of prediction for malignancy was also apparent in our study (20,21,23,38). However, unlike Haymart et al. (21,39), TSH level was not related to higher stages of cancer or extrathyroidal tumor extension (not described in Results section). Malignancy rate was increased with elevated TSH levels and the relationship remained significant even with normal TSH levels. The reason why TSH acts as a predictive factor for malignancy is not ascertained, but it has been proposed that TSH might cause tumor growth through the TSH receptor in well-differentiated thyroid carcinoma as in normal thyroid tissue (40,41), which results in occult cancer progression into overt cancer.
The baseline characteristics of our study showed a slightly higher prevalence of malignancy (18.1%) than other studies conducted in patients with ordinary thyroid nodules (42 –44). This might have resulted from the fact that our institution is a tertiary referral hospital. The proportion of PTC among thyroid cancer diagnosed in our study, 98.5%, was higher than 80% noted in other studies (45,46), but it is concordant with previous studies conducted in Korea showing a prevalence exceeding 90% (47).
When we investigated clinical variables as risk factors for cancer, association with decreased age was in agreement with previous studies (21). However, our results were different with respect to that no sex difference was observed, which was reported in several studies (48 –50), and smaller nodules showed positive association with thyroid cancer, which might be caused by selection bias resulting from detection of a lot of tiny nodules through high-resolution US; this explanation agrees with other studies (40,51).
This study is limited in that the final diagnostic outcome was not solely based on surgical histology, and moreover, benign nature of thyroid nodules was mostly decided only by a single FNA. However, when considering that benign nodules are less likely to be operated and that the negative predictive value of FNA is quite high, this study design is acceptable and efficient to evaluate malignancy and its risk factors in thyroid nodules, because it minimizes selection bias, which might be a limitation in histology-based studies. Another limitation is the small portion of patients who received surgery among those with indeterminate nodules. For this, we could not fully evaluate TgAb positivity in indeterminate nodules, although there was a slight increase of prevalence of malignancy in TgAb-positive group than the TgAb-negative group (44.8% vs. 50.0%; p = 0.763).
In conclusion, in addition to TSH, thyroid nodules with positive TgAb were independently associated with the presence of thyroid cancer. Our observations suggest that evaluation of TgAb in patients with indeterminate FNAC might give additional information to predict malignancy in conjunction with clinical risk factors and TSH levels. Therefore, we could reduce unnecessary surgery, although TgAb alone does not give clear information. Prospective studies are needed to validate the potential role of positive serum TgAb in predicting thyroid cancer in subjects presenting with indeterminate FNAC.
Footnotes
Acknowledgments
The authors thank Hyeon-Woo Yim, M.D., Ph.D., and Seung-Hee Jeong, M.P.H. (Catholic Medical Center Clinical Research Coordinating Center), for their invaluable advice on statistics.
Disclosure Statement
The authors declare that no competing financial interests exist.