
Abstract
Background:
Familial nonmedullary thyroid cancer (FNMTC) is a disease defined by clustering of thyroid cancers of follicular cell origin, and it is estimated to account for 5% of all thyroid cancers. Several studies found FNMTC to be more aggressive than sporadic disease, whereas others found them to have a similar course and outcome. The purpose of this study was to determine whether FNMTC is more aggressive than sporadic thyroid cancer.
Methods:
A retrospective controlled study of FNMTC versus sporadic nonmedullary thyroid cancers was conducted using a registry of patients with thyroid cancer. Data on disease severity at presentation, treatment modalities, and outcome were collected.
Results:
Sixty-seven patients with FNMTC and 375 controls with sporadic disease were included. Follow-up period was 8.6 ± 10 years for patients with FNMTC and 8.4 ± 9.1 years for sporadic cases. Patients with FNMTC had comparable disease severity at diagnosis as sporadic patients, underwent similar surgical and radioiodine treatments, and had similar long-term disease-free survival. Long-term outcome in families with three or more affected relatives was similar to families with only two affected relatives.
Conclusions:
Our results suggest that FNMTC is not more aggressive than sporadic thyroid cancer within our studied population. After a similar therapeutic strategy, FNMTC and sporadic cases had comparable prognosis, including in families with three or more affected members.
Introduction
Given the high prevalence of thyroid cancer, clustering of sporadic thyroid cancer in one family may not be rare. It has been estimated that 62%–69% of families with two affected relatives are sporadic occurrences, whereas the chance of a sporadic case in families of three or more affected members is less than 6% (5).
Whether FNMTC is more aggressive than sporadic disease is controversial. Several studies found patients with FNMTC to have increased risk of multifocal disease, local invasion, and lymph node metastases, leading to higher recurrence rate and decreased disease-free survival (3,6 –12). However, several other studies did not find FNMTC to be more aggressive than sporadic disease (13 –15).
To evaluate the clinical characteristics and outcome of FNMTC as compared with sporadic thyroid cancer, we performed a retrospective controlled study using the Beilinson hospital registry of differentiated thyroid cancer.
Patients and Methods
Patients
A total of 67 patients with FNMTC were included, representing 46 families. Fifty-four patients were from the Rabin Medical Center Thyroid Cancer Registry (5.3% of all registered patients) and 13 from other endocrinology clinics. Patients were included if data were available regarding staging at diagnosis, pathology, type of surgery, radioiodine treatment, and follow-up visits after surgery. Of 118 known patients in the included families (1 family with six patients, 1 family with five patients, 3 families with four patients, 11 families with three patients, and 31 families with two patients), sufficient information was available for 67 patients. The control group was 375 consecutive patients with sporadic nonmedullary thyroid cancer (SNMTC) from our registry.
The Rabin Medical Center Thyroid Cancer Registry includes all patients with nonmedullary thyroid carcinoma followed in our institute. To date, there are 1200 patients registered. The data was retrospectively collected for the period 1973–2004 and prospectively thereafter. These data include demographic information, medical and family history, age at diagnosis, type of surgeries, histopathology, treatment modalities, and outcome. The registry includes patients over the age of 18—either patients who were diagnosed during adulthood or patients who were diagnosed at a younger age who continued follow up in our institute after the age of 18.
Cases of thyroid cancer were defined as familial if two or more first-degree relatives were affected by histopathologically confirmed thyroid cancer of follicular cell origin. Patients were excluded if they had other known familial syndromes or exposure to factors that might cause thyroid cancer. In our registry, the diagnosis of familial syndromes causing thyroid cancer is based on clinical evaluation, with genetic testing performed at the discretion of the treating physician.
Study protocol
The following clinical variables were collected: age, sex, histopathology, Tumor, Node, Metastasis (TNM) staging, type of surgery, 131I treatment, local persistence or recurrence, distant metastasis, disease-free and overall survival at the end of follow up. Multifocality was defined as more than one tumor in one lobe or in both lobes in the thyroidectomy specimen. Persistent and/or recurrent disease was defined as disease within 1 year from primary treatment (surgery with/without radioiodine treatment), based on sonographic and cytologic findings, serum thyroglobulin levels, and iodine uptake beyond the thyroid bed. Due to the difficulty in differentiating persistent from recurrent disease, we grouped all cases with any evidence of tumor after initial treatment as recurrence/persistence. Intrathyroidal extension refers to vascular invasion or extension within the thyroid gland; extrathyroidal extension refers to any extension beyond the thyroid gland.
Patients with undetectable stimulated serum thyroglobulin levels (during hypothyroid phase or after recombinant human TSH [rhTSH] stimulation), normal findings on ultrasound examination of the neck, and negative findings on whole-body scan were considered disease free. The sixth edition of the TNM classification was used for staging (16).
Quality control of the registry input was performed by data verification on several occasions. Levels of thyrotropin, free thyroxine, thyroglobulin, and antithyroglobulin antibodies were measured by chemiluminescence assay (Immulite, 2000; Diagnostic Products Corporation, Los Angeles, CA) (for thyroglobulin, functional sensitivity, 0.9 ng/mL; analytical sensitivity, 0.2 ng/mL).
Statistical analysis
Baseline patient's characteristics and disease outcome were compared between the FNMTC group and the SNMTC group. Subgroup analysis was performed for thyroid cancer variants and for disease severity in the first generation compared with those in later generations. Proportions were compared using Fisher's exact test or Chi-square test, and continuous variables were compared using Student's t-test or Mann Whitney U-test, as appropriate. p-values less than or equal to 0.05 were considered statistically significant.
Results
Of the 442 included patients, 25 had three or more first-degree relatives with differentiated thyroid carcinoma, 42 patients had two affected relatives, and 375 had sporadic thyroid cancer. There was no difference in baseline characteristics between the familial and sporadic groups, except for a trend for a younger age in the familial group (mean 42.8 ± 16.8 vs. 47.2 ± 16.1, p = 0.06) (Table 1). There was no difference in the presence of antithyroid antibodies, histopathologic type of thyroid cancer, or mean tumor size at presentation. There was no significant difference in multifocality (56% vs. 44%, NS), extra-capsular invation (27.6% vs. 22%, NS), lymph node involvement (29.3% vs. 24.6%, NS), or prevalence of distant metastases (8.2% vs. 5%, NS) in the FNMTC and SNMTC groups, respectively. TNM staging was similar with 84% low-risk patients (stage 1 or 2) in the familial group and 77.5% in the sporadic group (Fig. 1).
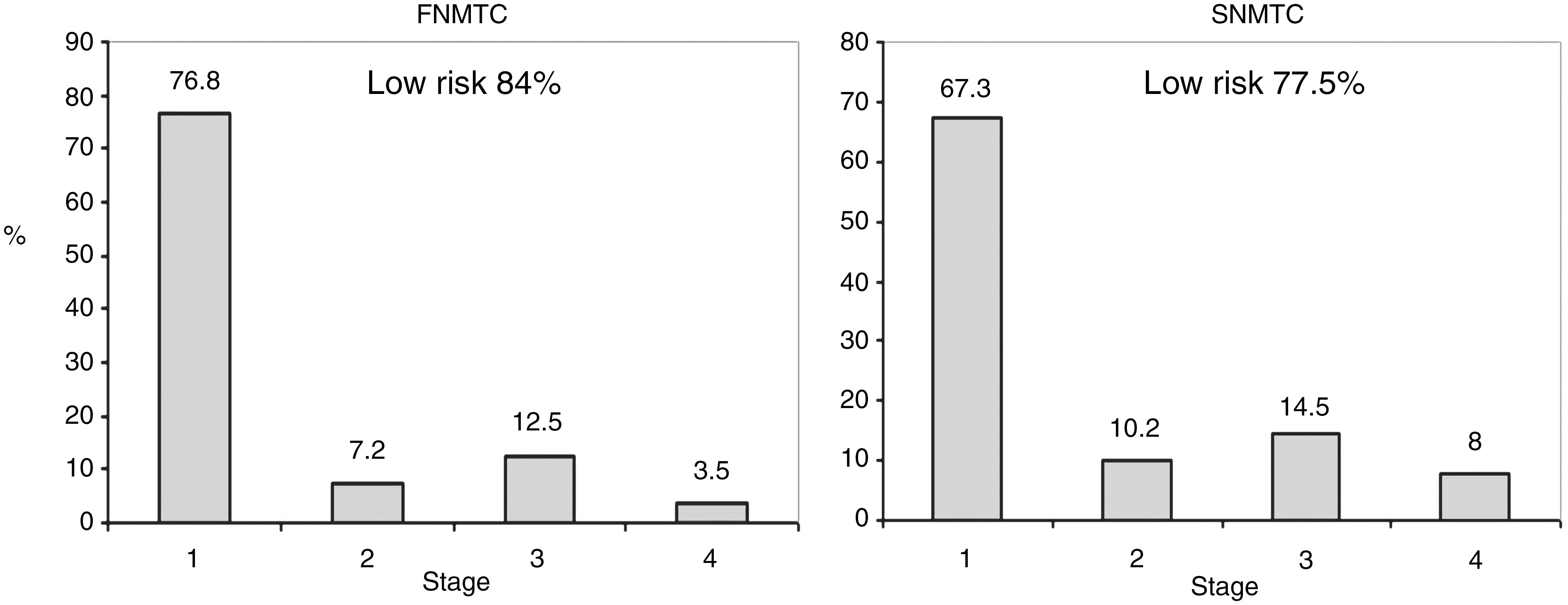
TNM staging in familial and SNMTC. Low risk refers to stages 1 and 2. FNMTC, familial nonmedullary thyroid cancer; SNMTC, sporadic nonmedullary thyroid cancer.
Data on histopathology was missing in four and two cases of FNMTC and SNMTC respectively.
FNMTC, familial nonmedullary thyroid cancer; SNMTC, sporadic nonmedullary thyroid cancer; NS, non-significant; PTC, papillary thyroid carcinoma; FV, follicular variant; FTC, follicular thyroid carcinoma; HCC, Hurthle cell carcinoma.
Total thyroidectomy was performed in the vast majority of patients, with 86.2% in the familial group and 89.1% in the sporadic group (NS). Other operations included subtotal thyroidectomy (6.9% vs. 0.6%) and hemithyroidectomy (6.9% vs. 10.3%). Lymph node neck dissection was performed in 22.4% of patients with FNMTC and in 15% of patients with sporadic disease.
Complete data regarding postoperative radioiodine therapy were available for 54 of the 67 patients with FNMTC and for 330 of 375 patients in the sporadic group. The rates of postoperative radioiodine treatment were comparable, with 79.6% in the FNMTC and 82.2% in the sporadic group. The groups did not differ in the mean first dose of I131 (114 ± 42 in the FNMTC group vs. 106 ± 51 mCi in the SNMTC group) or in the cumulative dose (375 ± 145 in the FNMTC group vs. 345 ± 145 mCi in the SNMTC group). A higher proportion of patients with FNMTC received more than one dose compared with the sporadic group (39.5% vs. 25.8%, p = 0.07). There was no difference in the use of external neck radiation (8.8% vs. 5.3%, NS).
Follow-up period was 8.6 ± 10 years for patients with FNMTC and 8.4 ± 9.1 years for patients with SNMTC. Outcome measures are presented in Figure 2. There was no difference in the prevalence of persistent/recurrent disease or of new distant metastases (diagnosed after initial treatment). There was also no difference in disease-free survival at the end of follow up (80% in the FNMTC group vs. 79.9% in the SNMTC group).
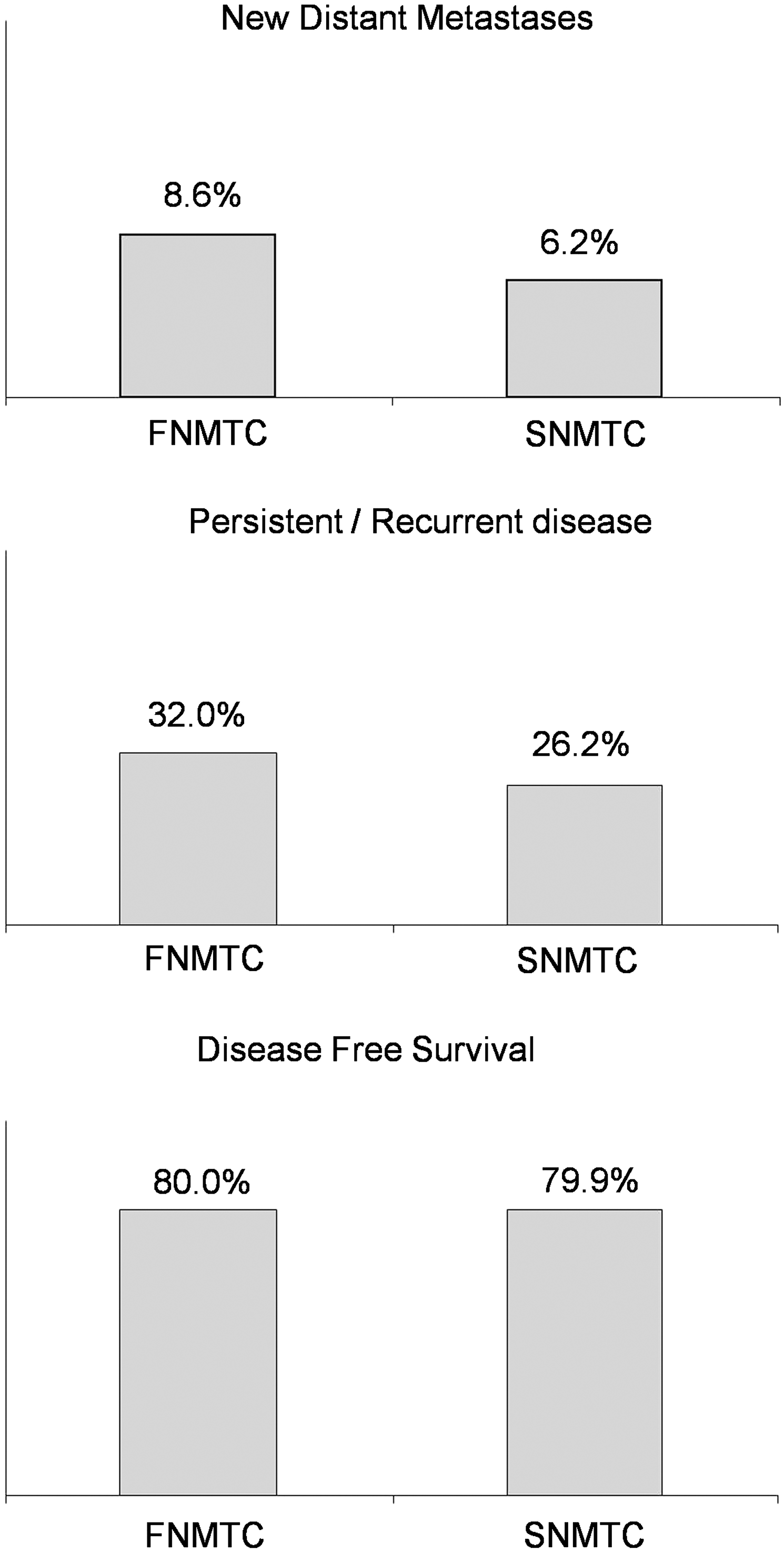
Long-term outcome of patients with familial and SNMTC. Disease free is depicted as the percentage of patients with no evidence of disease at their last follow-up visit: 8.6 ± 10 years for patients with FNMTC and 8.4 ± 9.1 years for patients with SNMTC.
Subgroup analyses were performed for number of affected relatives, for thyroid cancer variants, and for generation of affected patients. Comparison of patients with three or more affected relatives versus patients with only two affected relatives showed no significant difference in presentation and clinical course. Disease-free survival at the end of follow up was higher in the group of three or more affected relatives (90.9% vs. 77.7%, p = 0.16) (Table 2). Next, subgroup analysis for thyroid cancer variant was performed. There was no difference in distribution of variants between groups (Table 1), with most patients diagnosed with papillary thyroid carcinoma and small number of patients diagnosed with other variants. There was no difference in outcome measures when stratified according to disease variants, including disease recurrence/persistence rates and disease-free survival at the end of follow up (data not shown). For the presence of the anticipation phenomenon, family members in the first generation and those in later generations were compared, showing no significant difference in presentation, clinical course, or outcome (Table 2). This analysis was limited by incomplete inclusion of affected members within each family, as this is an intrafamilial phenomenon.
Discussion
FNMTCs have been recognized as a distinct clinical entity in the last decade (11). Though FNMTC may represent an array of genetically distinct syndromes, pending identification of involved gene(s), it is referred to as a single clinical entity. The ongoing debate regarding the aggressiveness of the disease led us to perform a study comparing patients with FNMTC with sporadic cases within our thyroid cancer registry.
Our analysis showed FNMTC to have similar staging at presentation, treatment regimens, and long-term outcome as compared with sporadic disease. There was a trend for younger age at presentation in the FNMTC group with a mean difference of 5 years. Patients with FNMTC underwent surgical and radioiodine treatment similar to patients with sporadic disease, with most cases undergoing total thyroidectomy and radioiodine ablation. At the end of follow up, there was no difference in disease-free survival, including in subgroup analyses for patients with three or more affected relatives and for disease variants. Papillary thyroid cancer was the most common type of cancer in both groups, comprising nearly 90% of cases.
Several previous studies have raised concern about FNMTC being more aggressive than sporadic NMTC in terms of local invasiveness, multifocality, lymph node involvement, and distant metastases (3,7 –11). This has led some investigators to recommend more aggressive therapy for FNMTC (2,3,8,11). However, other studies contradict this assertion. A meta-review of case series published in 1997 did not find FNMTC to be more aggressive than sporadic cases (14). A case control study from Toronto consisting of 24 cases of FNMTC found no difference in terms of invasiveness, risk for distant metastases, or disease-free survival between familial and sporadic NMTC (15). Uchino et al. (12) studied 258 cases of FNMTC from Japan, which were found to have more aggressive local disease, but similar rates of distal recurrence and survival compared with sporadic cases. Another recently published study evaluated 273 patients with FNMTC and found similar overall and cause-specific survival as patients with sporadic disease (13). A comparison table of our data with other published cohorts demonstrates significant variability in baseline characteristics and outcome (Table 3).
The discrepancy between our results and previous studies regarding the aggressiveness of FNMTC may have several explanations. First, the genes responsible for FNMTC have not been identified to date, and they may include several foci. Studies till date have been on small family groups, with contradictory results (17). Six potential regions have been identified: MNG1 (14q32), TCO (19p13.2), fPTC/PRN (1q21), NMTC1 (2q21), FTEN (8p23.1–p22), and the telomere-telomerase complex. An advantage of our work is the relative homogenous genetic background of included patients (97% Jewish). A possible explanation for the comparable outcome of FNMTC and sporadic cases in our cohort is a genetic defect different than described in other series. Second, patients with relatives affected by thyroid cancer may undergo more careful thyroid examination, more imaging studies, and may be diagnosed earlier. In this case, outcomes may appear comparable to sporadic cases due to earlier diagnosis and treatment and not due to similar biological behavior. However, several characteristics of our cohort may point against this argument. The FNMTC and the sporadic groups had similar tumor size and staging at presentation, underwent similar surgeries, and received similar radioiodine dosages. As opposed to several published series, the comparable baseline characteristics in our study enabled a more valid comparison regarding disease course between the two groups. Third, subgroup analysis for patients with three or more affected relatives was not reported in all studies, which may have led to missed subtle differences between groups. In our study, subgroup analysis of patients with more than three affected relatives did not reveal more aggressive features compared with patients with two affected relatives.
Our study was limited by several factors. The study was retrospective, which may have limited the accuracy and completeness of the collected data. Due to the nature of the clinical problem and its low prevalence, prospective studies (following offspings of affected families) have not been done to date. The use of our thyroid cancer registry and the common therapeutic approach in participating centers may have helped minimize bias resulting from the retrospective design. We did not have complete information regarding radioiodine treatment in a minority of included patients. However, the protocol for I131 treatment is homogenous in participating centers (18). We estimate the probability that differences in I131 treatment led to bias in our cohort being low. Finally, as in most previous studies on the subject, the sample size for patients with FNMTC was small, and we did not have full medical record of all known patients within the included families. This may have limited our power to detect minor differences between the study groups, between thyroid cancer variants, and to evaluate for the anticipation phenomenon. However, we believe that the incomplete inclusion of all known patients would not affect our primary outcome, comparing the aggressiveness of FNMTC with sporadic disease. If FNMTC is truly more aggressive than sporadic disease, we would expect a more aggressive course in most, if not all patients, or at least in families with three or more affected relatives.
In conclusion, our results suggest that FNMTC is not more aggressive than sporadic thyroid cancer within our studied population. After similar therapeutic strategy, both groups had comparable prognosis, including in families with three and more affected members.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.