
Abstract

Brain metastases from differentiated thyroid carcinoma (DTC) occur in 1% of cases, worsening the prognosis to a median survival of about 1 year (1). Data on the optimal treatment in this situation are limited. Neurosurgery, radiosurgery, stereotactic radiotherapy, and whole-brain radiotherapy are common treatments. Chemotherapy and radioactive iodine have also been employed, but the last is not likely to be effective because radioactive iodine uptake by brain metastases is uncommon (1,2). We report a patient with DTC who was successfully treated for recurrent brain metastases.
A 42-year-old man was found to have in 1991 a minimally invasive 6 cm follicular thyroid cancer (FTC) (T3N0M0), in the dominant nodule of a chronic multinodular goiter. After total thyroidectomy he received a cumulative doses of 33 GBq (900 mCi) iodine-131 for persistent uptake in the neck. Thyroglobulin (Tg) (solid-phase two-site immunoradiometric assay with sensitivity of 1.5 ng/mL) and Tg antibodies were undetectable after total thyroidectomy. For the next 10 years he remained free of apparent disease at which time he presented with seizures and was found to have brain metastases in the left frontal and the occipital lobes (Fig. 1). The left frontal lobe metastasis was resected and diagnosed on histopathology as FTC. The left occipital metastasis was treated with linac-based stereotactic radiotherapy (3 × 8 Gy at the 80% isodose). Tg ranged between 2.3 and 5.5 ng/mL. Posttreatment the patient remained on anticonvulsive therapy and seizures occurred sporadically, but otherwise there were no overt complications. No tumor activity was detected on magnetic resonance imaging (MRI) and 18F-fluoro-deoxy glucose (18FDG)–positron emission tomography (PET) scans.
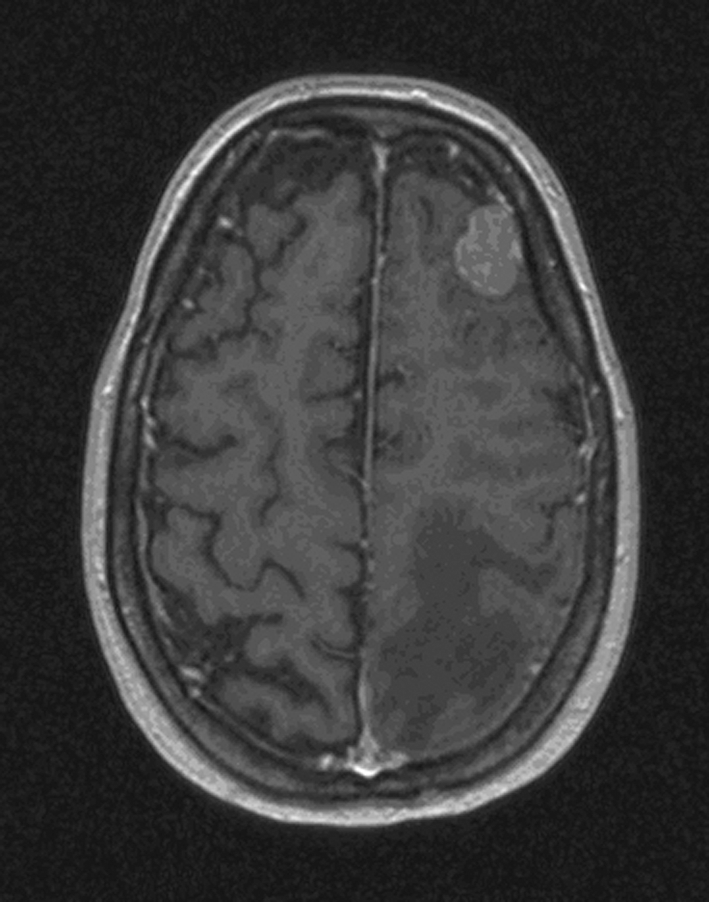
Axial T1-weighted image with gadolinium shows a left frontal, homogeneously enhancing metastases. Also, the edema of a second metastasis in the left occipital lobe (not shown) is noted. Scan made 10 years after primary diagnosis of differentiated thyroid carcinoma.
Five years later the left occipital metastasis was apparent on MRI. This was resected but a postoperative brain abscess occurred. He recovered after surgical drainage and long-term antibiotics. Two years later MRI showed a new 6.6 mm brain metastasis in the frontobasal area of the right hemisphere. This was treated with linac-based radiosurgery (20 Gy at the 80% isodose). On a follow-up MRI scan growth of the frontobasal lesion was observed, but a 11C methionine PET showed no uptake, so this was probably caused by radionecrosis. More than 18 months after the last treatment, his clinical situation is stable.
This patient's history and course are remarkable. He was in good condition 8 years after FTC brain metastases presentation, a very long survival compared to other reports. Chiu et al. noted a median survival after diagnosis of 12 months (1). In the seven patients of Salvati et al. (3), median survival was 26 months and the longest was 5 years. The median survival in McWilliams et al. (2) was 8 months with a range of 0 to 61. Chiu et al. (1) noted survival tended to be longer with a solitary as compared to multiple brain metastases (12 vs. 4 months, respectively).
Our patient's course indicates that some brain metastases are likely to be treated effectively with surgery and radiosurgery or stereotactic radiotherapy. Several studies suggest that surgical treatment is the currently most effective treatment of brain metastases from DTC. Chiu et al. (1) noted a median survival of 22 after surgery compared to 4 months with no surgery (p < 0.01). McWilliams et al. (2) noted similar respective results, 20 months versus 3 months median survival. That study, however, included patients with anaplastic and medullary thyroid cancer. These results, however, must be interpreted with caution as it is likely that one of the reasons that patients with multiple metastases were not selected for surgery is that they were more severely ill.
Radiosurgery is less invasive than a craniotomy and should be considered for treating brain metastases from DTC based on McWilliams et al. (2). However, this series is small with regard to this and two of the four patients initially treated with gamma knife had surgical resection later. In the nine patients of Kim et al. (4), five had a solitary brain metastasis and four had multiple metastases. They had gamma knife radiosurgery and the progression free period after this ranged from 4 to 53 months (median 12 months) and survival from 5 to 54 months (median 33 months). Tumor control (tumor disappearance, or reduction or no change in volume) was achieved in 25 of 26 tumors. There were no procedure-related complications.
In conclusion, the prolonged and continued survival of our patient with multiple brain metastases from DTC provides apparent support to treating such patients with combined aggressive treatment of neurosurgery and radiotherapy.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.