
Abstract
Background:
Vascular endothelial growth factor (VEGF-A) expression is upregulated in the majority of human tumors, where it stimulates proliferation, migration, and survival of endothelial cells. Studies have suggested that VEGF inhibitors can be used as an alternative therapy in medullary thyroid carcinoma (MTC), but data about expression of VEGF-A and its receptor in this tumor are scarce. The aims of this study were to evaluate VEGF-A, VEGF receptor (VEGFR)-1, VEGFR-2, and microvessel density (MVD) expression in MTC samples and correlate it with clinical parameters.
Methods:
Paraffin-embedded samples from 38 MTC patients were evaluated for VEGF-A, VEGFR-1, VEGFR-2, and MVD expression by immunohistochemistry. Clinical data were retrospectively reviewed in medical records.
Results:
Thirty-eight patients aged 31.8 ± 17.1 years were enrolled. Twenty-seven patients had hereditary disease (71.1%). Twenty-five of them were found to have multiple endocrine neoplasia (MEN) 2A and two were found to have MEN 2B. VEGF-A immunohistochemical staining was detected in 95% (36/38), VEGFR-1 in 96% (36/37), and VEGFR-2 in 91% (31/34) of MTC samples. Age at surgery was positively correlated with VEGFR-2 (p = 0.003). There was no correlation between VEGF-A, VEGFR-2, and tumor stage (tumor node metastasis). Nevertheless, VEGFR-1 was found to be inversely correlated with tumor node metastasis (p = 0.034). We also observed a trend toward an association between VEGFR-1 signal intensity and cure of disease, although this did not reach statistical significance (p = 0.054). Neither VEGF-A nor VEGFR-2 was associated with disease outcome after a median follow-up period of 5 years (p = 0.882 and p = 0.236, respectively). As expected, MVD was correlated with age at surgery (p = 0.005) and tumor size (p = 0.03). Patients with the hereditary form of the disease had a stronger intensity for VEGFR-1 (p = 0.039), whereas patients with sporadic disease displayed higher MVD counts (44 [27–63] vs. 21 [9–49], p = 0.018).
Conclusion:
The VEGF-A, VEGFR-1, and VEGFR-2 immunoreactive proteins are overexpressed in MTC lesions and might be implicated in tumor progression. It is not clear, however, if expression of these molecules provides prognostic information regarding the spread or outcome of MTC.
Introduction
Thyroid malignancies encompass many different histotypes with varying phenotypic characteristics that display unique clinical behaviors (5). Most thyroid tumors arise from follicular thyroid cells. They comprise a wide spectrum of neoplastic phenotypes, including benign adenomas, well-differentiated papillary and follicular thyroid carcinomas, as well as aggressive poorly differentiated or undifferentiated thyroid carcinomas (1,6). Medullary thyroid carcinoma (MTC) arises from parafollicular or C cells that produce calcitonin (CT) and accounts for 5%–10% of all thyroid cancers (7,8). MTC may occur sporadically (75%) or on a hereditary basis caused by germline mutations in the RET proto-oncogene (9). The RET proto-oncogene is expressed in cells of neuronal and neuroepithelial origin and encodes a receptor tyrosine kinase (10). In patients with familial MTC only the thyroid is affected. Patients with MEN 2A develop MTC, pheochromocytoma, and/or primary hyperparathyroidism. In addition, MEN 2B patients have MTC, pheochromocytoma, ganglioneuromas of the digestive tract, mucosal neuromas, and/or skeletal abnormalities (9). MTC tends to metastasize early via angioinvasion and hematogenous spread (6,9). The 10-year disease-specific survival of patients with MTC is about 75% (11).
It was only in the past two decades that VEGF-A was first positively associated with the tumorigenic potential of thyroid cancer cell lines (12 –18). In fact, several studies have demonstrated correlations between microvessel formation, increasing size of the primary tumor (19), intrathyroidal tumor spread (20), and disease-free survival in differentiated thyroid cancer (21). In these tumors, VEGF-A expression appears to be correlated with higher risk of recurrence and metastasis (22). In vitro studies have showed that VEGF-A secretion in thyroid cancer cell lines could be stimulated by thyroid-stimulating hormone (23).
Probably because of the higher prevalence, most of the data on the role of VEGF-A in thyroid carcinogenesis are derived from differentiated thyroid tumors. Little is known about the role of VEGF-A in the pathogenesis or clinical course of MTC. Considering the potential action of VEGF-A and its receptors in thyroid tumor growth and metastatic spread, as well as the fact that these small molecules have been considered targets for a new class of anticarcinogenic drugs (24), this study aimed to evaluate expression of VEGF-A, VEGFR-1, and VEGFR-2, and microvessel density (MVD) in a cohort of MTC patients followed at our institution. In addition, we have examined the possible associations between clinical features and the expression levels of these angiogenic factors.
Materials and Methods
Thyroid tissue
Our sample comprised 38 specimens with histopathological/immunohistochemistry (IHC) findings of MTC obtained from patients attending the Endocrine or Head Neck Divisions at Hospital de Clínicas de Porto Alegre, Porto Alegre, RS, Brazil, from 1997 to 2008. Twenty-seven patients had the hereditary form of the disease. Identification of RET germline mutations was performed by standard procedures, described previously (25). The diagnosis of sporadic MTC was established based on the absence of family history and known germline RET point mutations in exons 8, 10, 11, or 13–16. Clinical data were retrospectively reviewed in medical records. The ethics committee at the hospital approved the study protocol.
For patients with clinical or biochemical evidence of MTC, the surgical procedure consisted of total thyroidectomy and at least the resection of lymph nodes in the central zone of the neck combined with lymph node dissection of both cervicolateral compartments. For asymptomatic gene carriers with no abnormalities at cervical ultrasonography examination and normal serum CT levels, we recommended prophylactic thyroidectomy. Tumor staging was performed according to the International Union Against Cancer tumor node metastasis (TNM) classification (26).
Following our standard protocol, patients underwent a complete clinical examination and laboratory tests (levels of basal CT [until December 2003, Calcitonin IRMA-DSL7700; Diagnostic Systems Laboratories, Webster, TX; reference range <10 pg/mL; and after January 2004, Immulite 2000, Diagnostic Products Corporation; Los Angeles, CA; reference range: male <12.0 pg/mL and female <6.0 pg/mL]) and carcinoembryonic antigen (CEA; measured with chemiluminescence immunoassay; Immulite 2000, Diagnostic Products Corporation; reference range <3.4 μg/L).
The standard follow-up of MTC in our division consists of determining basal plasma CT and CEA (every 6 months). Serum calcium and 24-hour urinary metanephrines are measured in those patients with hereditary disease. Individuals with undetectable CT and CEA levels and normal physical examinations were felt to be in a complete biochemical remission and were monitored annually without additional imaging unless a change in examination, symptoms, or laboratory values was noted (27).
IHC analysis
IHC was performed on thin sections (3 μm) of previously formalin-fixed and paraffin-embedded tissues. The antibodies used were polyclonal rabbit antihuman VEGF-A (clone VG1; M7273 Dako Cytomation, Carpinteria, CA), monoclonal rabbit anti-human VEGFR-1 (VEGFR-1: #1303-1; Epitomics, Burlingame, CA), and monoclonal mouse anti-human VEGFR-2 (A-3: SC-6251; Santa Cruz Biotechnology, Santa Cruz, CA). Sections representing MTC were submitted to routine immunohistochemical technique, which comprises deparaffination and rehydration, antigenic recovery, inactivation of endogenous peroxidase, and blockage of unspecific reactions. Primary antibodies were incubated overnight at a temperature of 4°C, at dilutions of 1:400 (VEGF-A), 1:100 (VEGFR-1), and 1:200 (VEGFR-2), followed by application of streptavidin horseradish peroxidase conjugate (LSAB; Dako Cytomation), and diaminobenzidine tetrahydrochloride (Kit DAB; Dako Cytomation). Positive controls were human tissues, skeletal muscle tissue for VEGF-A, human placenta for VEGFR-1, and intestinal tumor for VEGFR-2; negative control was obtained by omission of the primary antibody.
The intensity of VEGF-A, VEGFR-1, and VEGFR-2 staining in each lesion was determined and quantified as grade 0 (absent, −), grade 1 (weak, +), grade 2 (moderate, ++), and grade 3 (strong, +++) based on the staining characteristics of most of the tumor. The slides were read independently by two blinded and experienced pathologists (L.M. and B.A.B.) who were not aware of the respective clinicopathological data. When the two experts differed in their interpretations, they consulted together and reached a consensus.
MVD assessment
Samples were prepared for IHC, as described above, using primary anti-CD31 antibody (clone JC7OA, M0823; Dako Cytomation). The Chalkley point technique was used for assessment of vascular density. The densest vascular areas (known as hot spots) were determined at low magnification (× 40 and × 100). The mean of the counts for the most angiogenic areas (hot spot) was recorded at × 400 magnification, and lung carcinoma was used as positive control.
Statistical analysis
Data were presented as median and interquartile interval. Spearman's coefficient test was used to assess the correlation between expression of the angiogenic markers (VEGF-A, VEGFR-1, or VEGFR-2) and MVD with age at surgery, tumor size, TNM stage, and disease outcome. Mann–Whitney's U-test was used to compare the number of MVD between patients considered free of disease or with persistent disease and between sporadic or hereditary disease. p < 0.05 was considered statistically significant. The Statistical Package for Social Science 15.0 professional software (SPSS, Chicago, IL) was used for statistical analysis.
Results
Patients
The clinical and oncological features of the 38 patients with MTC included in this study are shown in Table 1. Twenty-seven patients had a hereditary tumor (71.1%). Twenty-five individuals were found to have MEN 2A and two were found to have MEN 2B syndrome (Table 1). The identified RET mutations in MEN 2A patients were as follows: C634Y (20 individuals), C634R (2 individuals), and C618R (3 individuals). The two patients with MEN 2B presented the characteristic phenotype and mutation in codon 918.
RET mutations: C634R (Cys→Arg), C634Y (Cys→Tyr), C618R (Cys→Arg), and M918T (Met→Thr).
Age at surgery.
Dominant nodule size (cm).
International Union Against Cancer classification for TNM.
MEN, multiple endocrine neoplasia; NA, not available; NE, not evaluated; TNM, tumor node metastasis; VEGF-A, vascular endothelial growth factor A; VEGFR-1, vascular endothelial growth factor receptor 1; VEGFR-2, vascular endothelial growth factor receptor 2.
The patients had a mean age of 31.8 ± 17.1 years at the time of surgery and 24 (63.2%) were women. Patients with sporadic MTC were older at diagnosis than those with hereditary disease (41.7 ± 15.2 vs. 27.8 ± 16.4 years, respectively, p = 0.02). CT median value was 284.5 pg/mL (37.8–994.3) and CEA median value was 14.6 ng/mL (1.7–44.3). Ten (26.3%) patients had stage I, 12 (31.6%) were classified as stage II, 12 (31.6%) as stage III, and 4 (10.5%) patients had stage IV disease. Twenty-nine (76.3%) patients are considered free of disease after a follow-up period of 5.6 ± 2.6 years.
Expression of VEGF-A and VEGFRs in MTC
VEGF-A immunohistochemical staining was detected in 36 of the 38 (95%) MTC samples; VEGFR-1 immunoreactivity was detected in 36 of 37 (96%) and VEGFR-2 in 31 of 34 (91%). As expected, positive immunoreactions of VEGF-A, VEGFR-1, and VEGFR-2 were detectable in the cytoplasm of the thyroid cancer cells, but rarely in stromal cells or surrounding healthy thyroid tissue (Fig. 1A–C).
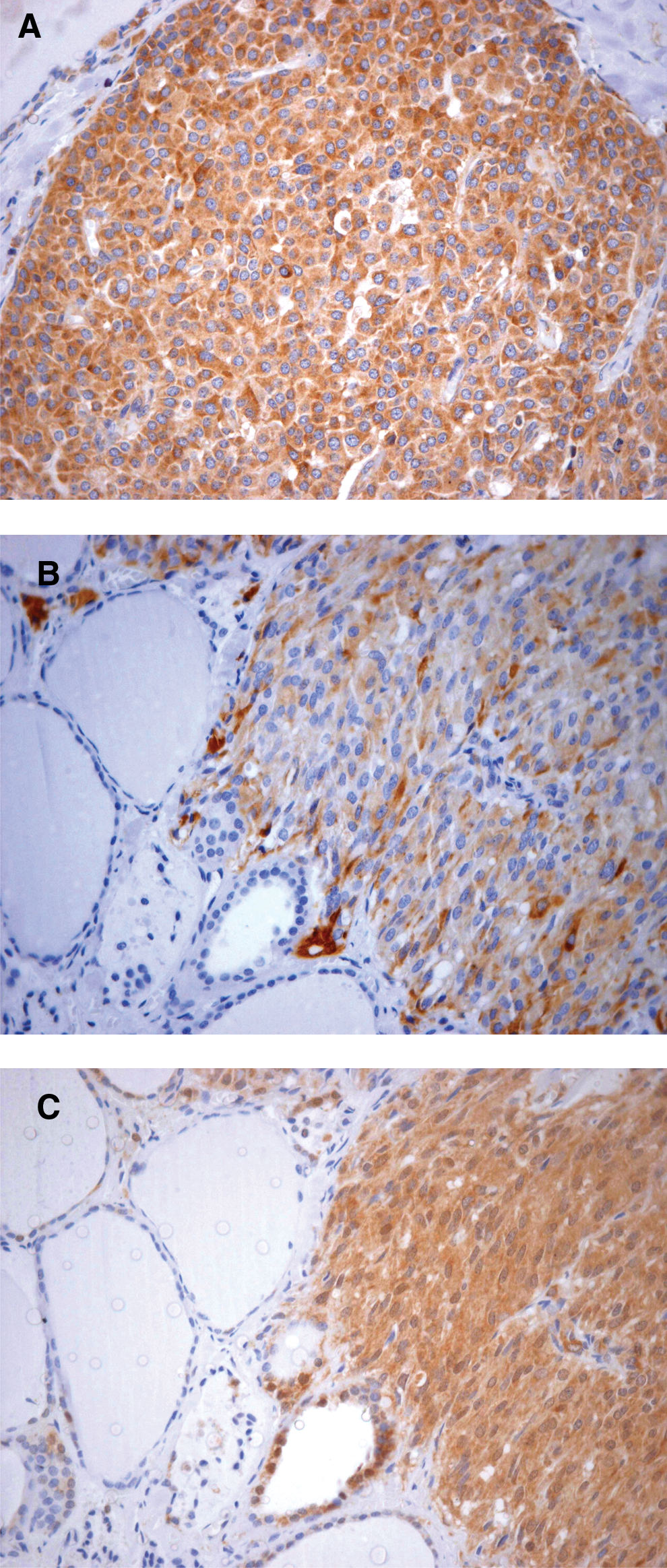
Immunohistochemical detection of VEGF-A (
When we evaluated expression of the angiogenic molecules with clinical parameters, we observed that VEGFR-2 expression was positively correlated with age at surgery (r = 0.490, p = 0.003), whereas no correlation was found to VEGF-A and VEGFR-1 (Fig. 2A–C). Expression of VEGF-A, VEGFR-1, or VEGFR-2 was not associated with tumor size (p = 0.425, p = 0.080, and p = 0.183, respectively). Sixteen patients had lymphatic or distant metastases at the time of surgery. There was no correlation between tumor stage (TNM) and VEGF-A or VEGFR-2, but VEGFR-1 was found to be inversely correlated with the stage of the disease (r = −0.34, p = 0.034, respectively; Table 2). We also observed a trend toward an association between VEGFR-1 signal intensity and cure of disease, although this did not reach statistical significance (p = 0.054). Neither VEGF-A nor VEGFR-2 was associated with disease outcome after a median follow-up period of 5 years (p = 0.882, p = 0.236, respectively).
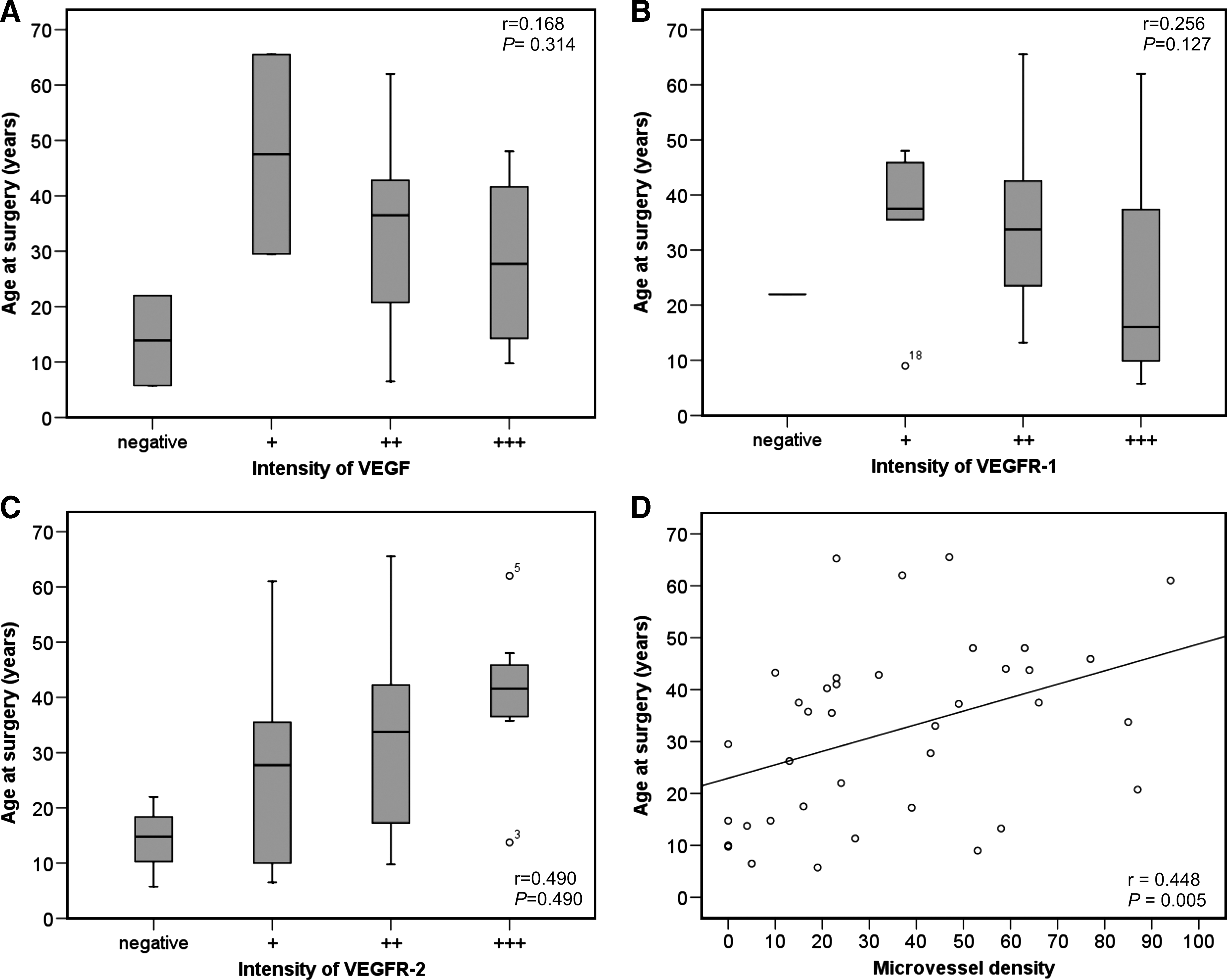
Association between age at surgery and immunohistochemical intensity of VEGF-A (
Spearman's test.
n, number of patients.
MVD assessment
For evaluation of MVD as a measure of angiogenesis, we used CD31 staining. The pattern of CD31 antibody expression in MTC is shown in Figure 3. The median MVD for all samples was 26 microvessels/mm2 (15–54). Age at surgery and tumor size (cm) were correlated with MVD (r = 0.448, p = 0.005, and r = 0.367, p = 0.03, respectively; Fig. 2D). However, there was no correlation between MVD and TNM stages. The median microvessel count was as follows: stage I, 7; stage II, 30; stage III, 40; and stage IV, 23 microvessels/mm2 (r = 0.266, p = 0.107). The number of MVD was similar between patients considered free of disease or with persistent disease: 23 (10–61) versus 27 (23–41) (p = 0.770). There was no correlation between VEGF-A, VEGFR-1, or VEGFR-2 and MVD in MTC samples (r = 0.260, r = 0.241, and r = 0.215, respectively, p > 0.05).

Immunohistochemical detection for MVD in medullary thyroid carcinoma at 400 × magnification. The brown-dark represents blood vessels stained by CD31 antibody in medullary carcinoma sample. Color images available online at
Sporadic and hereditary MTC tumors
Since there are both a hereditary and a sporadic form of thyroid medullary tumors, we also analyzed both groups separately. We found no difference in the intensity of VEGF-A or VEGFR-2 among hereditary and sporadic patients (p = 0.295 and p = 0.488, respectively), whereas patients found to have the hereditary form of MTC had higher expression of VEGFR-1 than sporadic patients (p = 0.039). Higher MVD was found in patients with sporadic MTC than in patients with hereditary MTC (44 [27–63] vs. 21 [9–49], p = 0.018, respectively; Table 3).
Mann–Whitney U-test.
Median (percentile 25%–75%).
MVD, microvessel density.
Discussion
This study examined expression of angiogenic factors in MTC samples. We observed VEGF-A, VEGFR-1, and VEGFR-2 overexpression in more than 90% of tumor specimens. Although VEGF-A staining was not associated with clinical presentation or tumor aggressiveness, VEGFR-2 was associated with age at surgery, whereas VEGFR-1 was found to be inversely correlated with tumor stage. None of these molecules were associated with outcome (free of disease or persistent disease).
Increased expression of VEGF-A indicates that an angiogenic switch in carcinogenesis occurs with subsequent upregulation of pro-angiogenic growth factors to produce de novo vascularization to supply the growing tissue (18). VEGF-A, an important stimulator of angiogenesis, has been implicated in proliferation and spread of different malignant tumors. Our findings showed a moderate to strong staining of VEGF-A in MTC. VEGF-A expression upregulation has been previously reported in differentiated thyroid tumors by in vivo and in vitro studies (12 –16,18,22,28 –30), but very few reports focused on MTC. Bunone et al. (5) and de la Torre et al. (18) evaluated six and eight MTC samples, respectively, and showed positive immunostaining in all samples analyzed. Higher expression of VEGF-A on MTC samples is corroborated by in vitro study using MTC cell lines that showed higher expression of VEGF-A mRNA and protein than normal thyroid tissues (31).
Studies focusing on the prognostic value of VEGF-A expression in differentiated thyroid carcinomas have shown conflicting results. Several studies have demonstrated increased VEGF-A expression associated with metastatic spread in thyroid papillary cancer samples (5,22,30,32). A study with a 5-year follow-up also demonstrated that immunohistochemical expression of VEGF-A correlates with local and distant recurrence of papillary thyroid carcinoma and demonstrated that VEGF-A staining is strongly associated with more frequent local and distant recurrence (33). In addition, elevated VEGF-A mRNA expression was associated with high tumorigenic potential and has been suggested as an important event in the transition from low to high-grade tumors (12). In contrast, other immunohistochemical studies have described an absence of correlation between VEGF-A expression and TNM staging or tumor size and extent of invasion in papillary carcinomas (32,34). Moreover, a recent study comparing serum VEGF-A in 48 consecutive papillary thyroid carcinoma patients categorized by TNM staging with 20 healthy control subjects identified a negative correlation between TNM classification staging and serum VEGF-A levels (35). However, these apparently conflicting results could be due to the different techniques to quantify VEGF-A expression, using different antibodies reactive to VEGF-A. On the other hand, based on the observations described above, it could be hypothesized that the potential implications of VEGF-A in the progression of thyroid neoplasms is distinct for histologic subtype.
There are few data available about VEGF-A expression and clinical features in MTC. The two previously referred to studies, those that evaluated six and eight MTC patients, reported that VEGF-A expression at diagnosis was associated with lymph node metastasis (5,18). In this report we observed no correlation between VEGF-A staining and age at surgery, tumor size, or TNM staging in our 38 patients with MTC. Of these patients, 22 had localized disease (TNM I–II) and 16 had metastatic disease (TNM III–IV), but the staining signal of VEGF-A did not differ between them. These findings are consistent with a recent study that did not observe a correlation between serum VEGF levels and the extent of disease in MTC patients (36).
An interesting finding of this study was the positive association between VEGFR-2 staining and age at surgery, since age-dependent progression is a characteristic feature of MTC (37,38). The VEGFR-2 signaling pathway is crucial in bringing about the effects of VEGF-A, including vasodilatation, endothelial cell migration, and proliferation, and it has been considered as the key mediator of VEGF-induced angiogenesis (39,40). Of note, VEGFR-1 has a 10-fold higher binding affinity to VEGF-A, but exerts less activation of intracellular signaling intermediates than VEGFR-2. In fact, VEGFR-1 is thought to be a negative regulator of VEGF-A activity either by acting as a decoy receptor for VEGF-A or by downregulating VEGFR-2-mediated signaling. Indeed, the VEGF-A-mediated stimulation of VEGFR-1 autophosphorylation and signaling in endothelial cells is weaker than signaling through VEGFR-2 (6,41). Our findings support these premises, since we have observed a positive correlation of VEGFR-2, whereas VEGFR-1 expression presented a negative correlation with tumor stage. In line with these observations, one would expect to find a positive correlation between the grade of VEGFR-2 staining and TNM stages, but this could not be demonstrated (Table 2).
Tumor angiogenesis has been considered a prerequisite for tumor growth, progression, invasion, and metastatization (42). A significant association between vascular density, quantified by microvessel counting, and tumor metastasis has been reported for several solid tumors, including breast carcinoma (43), gastric carcinoma (44), and colon carcinoma (45). Regarding differentiated thyroid tumors, MVD counts seem to be higher compared with normal tissue (19 –21). Increased MVD in differentiated thyroid carcinomas tended to be associated with improved survival, whereas a lower MVD in undifferentiated thyroid tumors is associated with worse prognosis (46,47). The scarce data available seem to point to the idea that MTC samples have the highest MVD compared with other types of thyroid cancers (46). One study examined 157 primary thyroid cancers, including 82 well-differentiated epithelial cell thyroid carcinomas, 52 medullary carcinomas, and 23 undifferentiated thyroid carcinomas and demonstrated that MVD was associated with poor prognosis only in medullary carcinoma. In that study, all of the patients who died of MTC had a microvessel count >30. This was significantly different from those patients with MTC who were alive at the time of study. In contrast, in patients with well-differentiated carcinoma and undifferentiated carcinoma there were no such differences (48). We also noted positive correlations between age at surgery with MVD counts and tumor size with MVD counts, but no association between tumor stage or the presence of persistent disease with MVD counts. The reasons for this are not clear. The divergence may be related to differences in characteristics of the sample populations or to different techniques to quantify MVD expression.
Sporadic MTC is more common (75%–80%) than hereditary MTC (20%–25%). In the sample population studied here, however, most patients (70%) had hereditary MTC due to the selection bias of our institution being a referral center for molecular diagnosis. Because this could influence our results, we compared expression of angiogenic markers in the sporadic and MTC groups. No differences were observed in the intensity of VEGF-A or VEGFR-2, but patients with the hereditary form of MTC had higher expression of VEGFR-1 than sporadic patients (Table 3). When comparing MVD counts between the two groups of patients, we observed a higher count in patients with the sporadic form. These results might be attributed to a long time course of the disease in the sporadic group, since patients with hereditary MTC were younger at the time of surgery.
Conclusions
This study supports the idea that VEGF-A and its receptors are implicated in the development and maintenance of sporadic and hereditary MTC. Consequently, these findings demonstrate a biological basis for VEGF-related tyrosine-kinase therapy in sporadic MTC tumor and might indicate a potential advantage for compounds that inhibit both RET and VEGF tyrosine kinase activities for hereditary disease. Nevertheless, the determination of the angiogenic phenotype may have limited prognostic value for patients with this type of tumor.
Footnotes
Acknowledgments
The authors are grateful to the physicians who sent patients for molecular analysis and the surgeons at our hospital, Dr. Alceu Migliavacca and Dr. José Ricardo Guimarães, for surgical management of their patients. Grant support: Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Fundacão de Amparo Pesquisa do Estado do Rio Grande do Sul (FAPERGS), and Fundo de Incentivo à Pesquisa do Hospital de Clínicas de Porto Alegre (FIPE), Brazil.
Disclosure Statement
The authors declare that there are no competing financial interests.