
Abstract
Background:
Spinal metastases secondary to thyroid cancer of follicular and parafollicular cell origin are uncommon but may require stabilization of the compromised vertebrae to prevent fracture with spinal cord injury. Such treatment may also relieve pain and improve survival and quality of life.
Summary:
Percutaneous vertebroplasty (PV) is a minimally invasive, radiologically guided procedure whereby bone cement is injected into a structurally weakened vertebra to provide immediate stability. The authors present two cases of thyroid cancer with spinal metastases. Both patients successfully underwent PV. Following PV, the patients experienced significant pain relief with immediate reduction in analgesic requirements and improvement in other symptoms. Both were able to return to their daily activities.
Conclusion:
PV is a minimally invasive spinal procedure and should be considered for patients with metastatic thyroid cancer with spinal metastases.
Introduction
Bone metastases from DTC occur in 2%–13% of patients (3) and in about 23% of patients with medullary thyroid cancer (MTC) (4). Patients with MTC often have multiple and simultaneous metastases to liver, lungs, and bones (5). Coleman reported that spinal cord compression occurs more frequently in patients with metastatic DTC (28%) when compared with other cancers such as prostate (10%) or breast cancers (8%) (6).
Patients with poorly differentiated papillary thyroid cancer, invasive follicular, or Hurthle cell cancers are more likely to have distant metastases than the patients with well-differentiated cancers. The predicted 10-year survival of patients with bone metastases ranges from 13% to 21% (3). Eighty percent of bone metastases from all tumors including thyroid cancer occur in the axial skeleton where blood flow is high (spine, ribs, and hips). The body of vertebrae (29%) is the most common site, followed by the pelvis (22%), femur (15%), and skull (13%) (7).
Most thyroid bone metastases are osteolytic (8) and reduce the quality of life by causing pain and fractures, sometimes with spinal cord compression (3). Symptoms may be the consequence of a pathologic fracture secondary to vertebral destruction, with development of spinal instability and compression of adjacent neurological structures. The survival rate of patients with pathological fractures is lower than that found in patients without fractures (9,10).
Radioiodine is the initial treatment of choice for patients with bone metastases from DTC in patients whose metastatic tumors take up I131. Unfortunately, only about 55% of patients with metastases of DTC are effectively treated with radioiodine (11).
Focused radiation therapy and chemotherapy may relieve pain and tumor growth but are associated with side effects and a delayed response. These treatments also fail to stabilize the fracture (12). In contrast, surgical treatment usually restores spinal stability and decreases the risk of vertebral collapse. The main indications for surgery are real or anticipated spinal instability with or without neural compression, persistent pain refractory to medical therapy, and poor uptake of radioiodine (3).
Bone stabilization with tumor resection is indicated in selected individuals such as those with single or adjacent level disease with neurological symptoms from tumor compression or vertebral collapse, who are otherwise in relatively good health and have a life expectancy of 6 months or greater (13). Some patients, however, may not be surgical candidates because of rapidly progressing systemic disease or other medical problems.
Percutaneous vertebroplasty (PV) is a minimally invasive, radiologically guided procedure in which bone cement (polymethylmethacrylate [PMMA]) is injected into structurally weakened vertebrae. PV was introduced in 1984 by Deramond and Galibert for the treatment of a painful vertebral hemangioma and adopted to treat spinal tumoral osteolysis. This procedure provides biomechanical stability and pain relief (14). After injection the cement morphology stays unchanged, providing long-term stabilization and pain relief (15). The recurrence of pain is most likely due to the development of new or progressive tumor rather than failure of the initial procedure (12).
We report two patients treated with PV for palliative care who had advanced thyroid cancer with severe movement-related back pain and document that following PV, the patients experienced significant pain relief, reduction in analgesic requirements, and improvement in other symptoms. Within 2 weeks after their respective operations, both patients were able to return to their normal activities of daily living with an improved quality of life until death.
Case 1: PV for Follicular Thyroid Carcinoma Spinal Metastasis
History
A 63-year-old Caucasian man had a total thyroidectomy for a T3N0M0 (5th ed.) (16) follicular thyroid cancer. Postoperatively he was treated with I131 and thyroid hormone suppressive therapy. Eight years following his operation he developed low-back pain. His thyrotropin at this time was appropriately suppressed at 0.01 mME/mL. A magnetic resonance imaging scan revealed 1-cm L5 vertebral metastasis without fracture. His blood thyroglobulin level was 483 ng/mL (normal, less than 42 ng/mL). He was treated with I131 (total dose, 8389.7 MBq/226.75 mCi) but no uptake was observed anywhere or at the site of spinal metastasis on posttreatment imaging. He was therefore treated with external radiation (44 Grey to L5 level). His focal back pain became progressively more severe and was aggravated by motion, thus restricting his activity. He required oral narcotics.
Three years earlier both his magnetic resonance imaging and computed tomography (CT) scans demonstrated a mix osteolitic–osteoblastic metastatic tumor with compression fracture of L5 vertebral body (Fig. 1). His low-back pain was 7/10 (numerical rating scale 0–10/10). He had no neurological urinary or bowel dysfunction or any sensory or motor deficits and had tenderness to percussion at L5 vertebrae. The patient refused an open operation because of risk of possible complications. However, he accepted PV because of increasing uncontrollable pain.
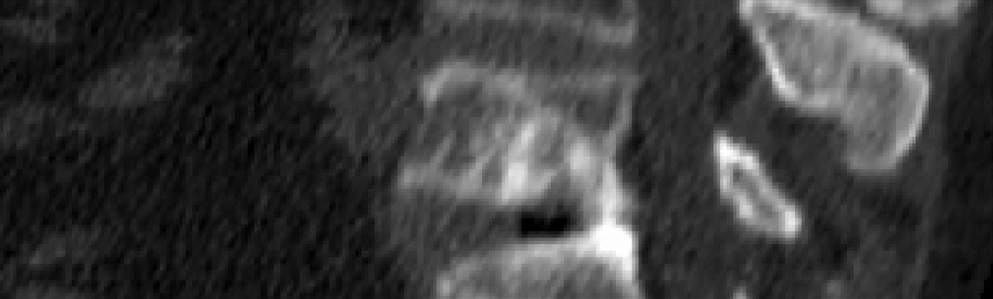
Case 1. Preoperative imaging: CT reconstruction L5 vertebrae demonstrating metastatic lesion with compression fracture. CT, computed tomography.
The patient was taken to the operation room and PV was done under local anesthesia with fluoroscopic guidance. After the infiltration of soft tissues with marcaine, a unilateral puncture of the vertebral body was done with a 11G needle. The procedure was more difficult because of severe osteosclerosis of the posterior elements of L5. Six milliliters of PMMA bone cement (Simplex; Stryker) was then injected into the collapsed vertebral body.
The patient did well following this procedure. A CT scan was done (Fig. 2) and he was discharged at 3 hours after the procedure with dramatic relief of his back pain, which declined from 7/10 to 2/10. Two months after PV, his pain level remained at 2/10, for which he occasionally took nonnarcotic pain medications. The patient died at 2 years after PV because of unrelated problems. At that time he had no signs of cancer progression despite not removing his metastatic tumor.

Case 1. Postoperative imaging: Sagittal CT reconstruction demonstrating bone cement into L5 vertebral body.
Case 2: PV for MTC Spinal Metastases
History and examination
A 60-year-old Caucasian man complained of severe low-back pain of 4 months duration. On examination, the patient reported low-back pain as 8/10 (numerical rating scale 0–10/10). Neurological examination revealed no motor deficit, but with slight hypesthesia of L1 on the right. Five years earlier the patient underwent a total thyroidectomy and central and bilateral neck dissections for MTC T4N1aM0 (5th ed.) (16). After his operation he was treated with external radiation to his neck. His blood basal calcitonin level at this time was 11.4 pg/mL (normal range, below 20.0 pg/mL; and less than 1 after total thyroidectomy). He had no familial history of MTC or other endocrine pathology and RET testing was not done. Lung metastases were unfortunately detected by CT and Technetium-99 m dimercaptosuccinic acid (Tc99m-DMSA) scan at 2 years after his thyroidectomy and his basal calcitonin level increased to 135 pg/mL. Regional lymph node metastases were removed at 5 years after initial treatment. During CT examination, distant liver and spinal metastases (L2 and L4) were identified (Fig. 3).
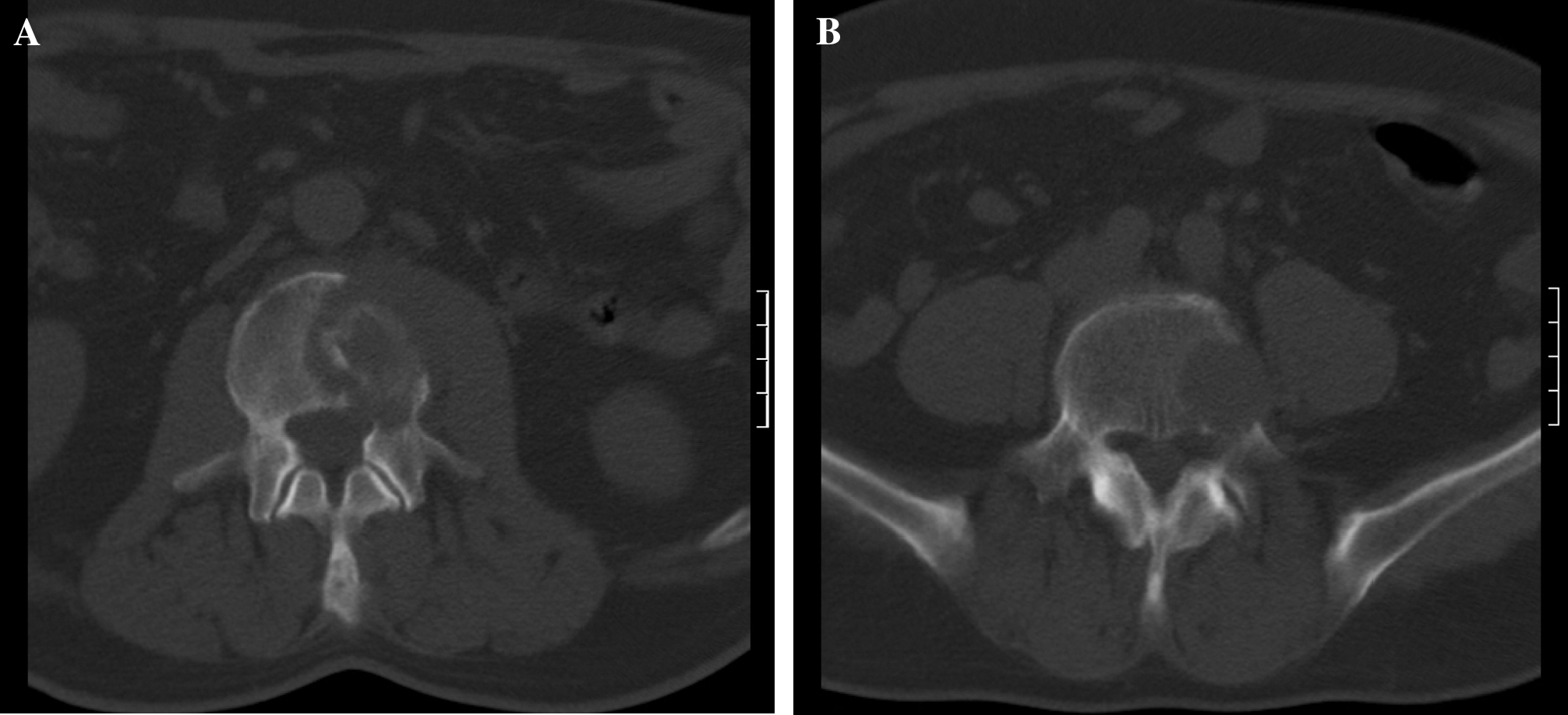
Case 2. Preoperative imaging studies: Sagittal CT demonstrating metastatic lesions in L2 (
Because of extensive lesions of L2 and L4 vertebral bodies, a two-staged operation was performed after biopsy at L2 revealed metastatic MTC into vertebrae. First, a unipedicular left-sided PV L2 and L4 was done under local anesthesia. Bone cement (Simplex; Stryker) was injected into the bodies of L2 and L4 (Fig. 4A). After this procedure, his low-back pain and use of analgesics decreased from 8/10 to 3/10. Two days later, a transpedicular fixation of L1–L3 was carried out under general anesthesia (Fig. 4B).
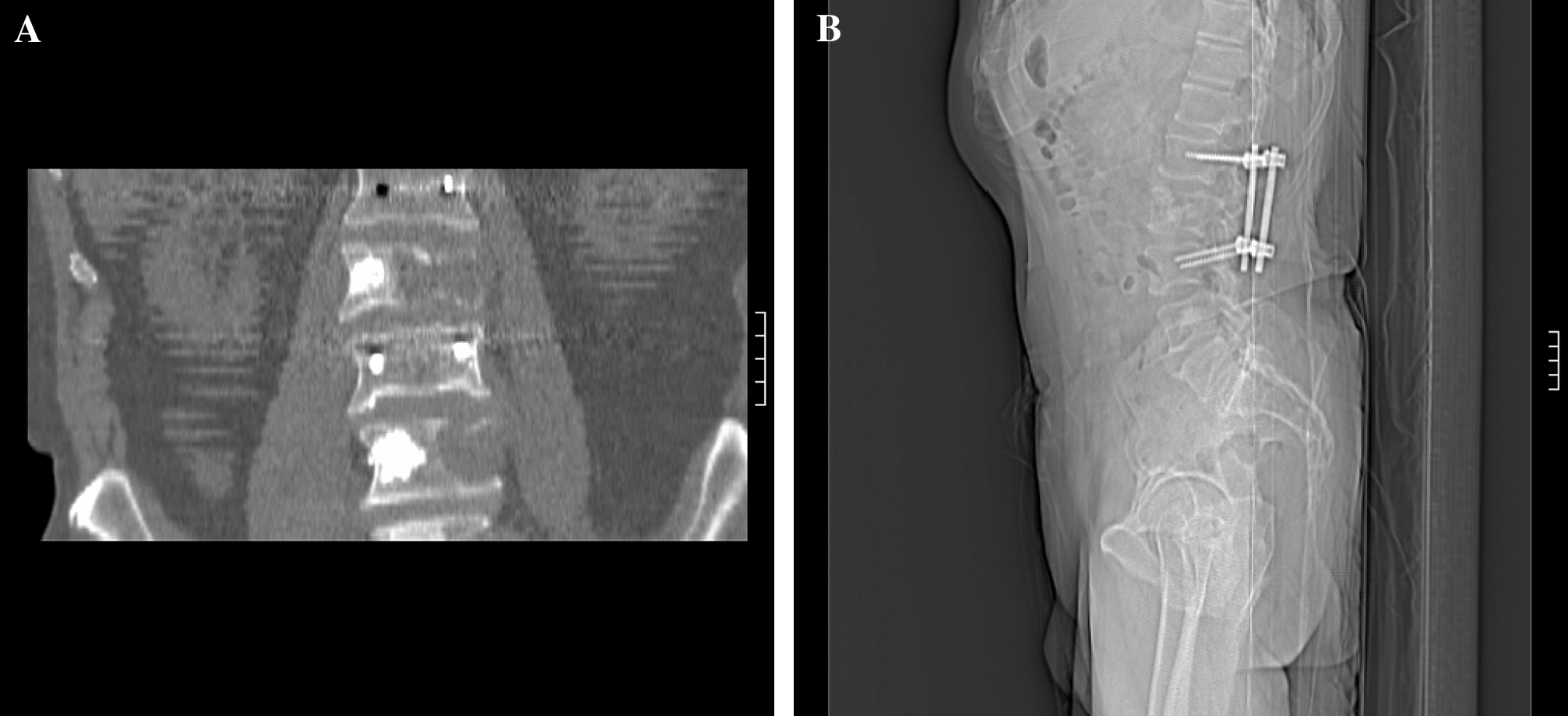
Case 2. Radiological studies obtained in a 60-year-old man after operation: A coronal CT reconstruction (
At discharge, 3 days after these procedures, he noticed that his movement-related spinal pain had decreased from 8/10 to 2/10. He was now taking nonnarcotic pain killers. Because of L1 pain, which radiated to the right and required local anesthetics, he was treated with radiofrequency destruction of this L1 root. The patient subsequently underwent 131I-metaiodobenzyl—guanidine (131I-MIBG) therapy at 4 months after these procedures. Unfortunately, the size and number of liver and lung metastases progressed during the next 6 months but without recurrence of low-back pain. The patient died at 8 months following his spine operation because of progressive lung and liver metastases.
Discussion
In 1967, Halnan and Roberts wrote, “Even when the site of the primary tumor is known, treatment is too often symptomatic only, and when the primary is not known it is sometimes thought that energetic pursuit of the diagnosis is academic,” and that the patient is better left to “die in peace.” (17).
The care of patients with advanced metastatic cancer presents many challenges. For patients with bone metastases, treatment is primarily palliative. The aim of the therapy is primarily to relieve pain with improvement in the quality of life and to prevent pathological vertebral fractures with possible neurological dysfunction.
Pain is often the main symptom of metastatic bone involvement and unfortunately often becomes progressively more severe and resistant to nonopioid analgesics (3). The three types of pain encountered are local, mechanical, and radicular. Local pain is thought to arise from irritation and inflammation of the periosteum due to invasion by tumor (18). Mechanical pain seems to be the main component in metastatic spinal pain and appears to be related to the destruction of bone with reduced load-bearing capabilities, resulting initially from trabecular disruption and microfractures and subsequently from loss of bony integrity (Fig. 5). Radicular pain is a sharp, shooting pain that follows the sensory distribution of a particular nerve root or roots. Radicular pain is caused by epidural and neuroforaminal compression of nerves by tumor growth (18). PV provides mechanical stabilization of the involved vertebral body and often provides improvement in mechanical pain as occurred in our two patients. These observations have also been observed by other authors (19,20).

Illustration mechanism of mechanical pain in spinal metastases: 1, lateral deformity of the vertebral body and periosteal irritation; 2, subperiostal fractures; 3, subperiostal hematomas; 4, deformity of end plates of vertebral body.
We believe that patients suffering from significant, focal, mechanical pain unresponsive to analgesia due to osteolytic metastases are potential candidates for vertebroplasty. Blastic metastases with an osteolytic component may also be considered for vertebroplasty. Extensive bone destruction with significant vertebral collapse leading to height loss of 70% or more may be a contraindication (13). Severely compressed vertebrae are technically difficult to treat and compression of the cord or nerve roots by displaced fracture fragments may be made worse with the injection of bone cement (13). Significant epidural tumor is a relative contraindication for similar reasons. Metastatic involvement of the posterior elements of the vertebrae should not be treated with PV because of high risk of epidural leakage (13).
Between 50% and 97% benefit from PV, with pain reduction in selected patients with vertebral metastasis (12). Clear improvement is usually defined as complete pain relief with no requirement for analgesic medication (complete relief ) or enough of a decrease in pain that the dose of analgesic drugs can be reduced by at least 50% (partial relief ). The replacement of narcotic drugs with nonnarcotic drugs is also considered clinical improvement (12).
Immediate postprocedural pain relief is the best predictor of successful vertebroplasty (21). Our two patients underwent PV without complications and both patients reported excellent pain relief. Before the surgery the patients required constant narcotics for pain relief. Following PV, spinal pain decreased from 7/10 to 2/10 in the first patient and from 8/10 to 2/10 in the second. For treatment of the coexisting radicular pain, radiofrequency ablation of the L1 nerve root was done in the second patient. PV provided rapid and sustainable pain relief with improvement in performance status until the death of both patients. Although the tumor was not resected in these patients, PMMA bone cement might have had an antitumor activity as a result of cytotoxicity, thermal effects, and/or ischemia (22).
Mechanical weakness with vertebral collapse may result in severe neurological complications. Cement injection restores vertebral stability apparently with little risk as reported in our two patients and in previous publications (23,24). To obtain the best stabilization of the injured vertebral body, one should both fill the vertebral body with cement and anchor it to uninvolved bone (Fig. 6). Cement injected into vertebral bone can “preserve” bone tissue from further metastatic destruction. We injected the bone cement into the vertebral body bone from the unaffected side and tried to fill it completely. Higgins et al. have calculated the cement volume required to restore vertebral stability (25). They reported that filling about 17% of the vertebral body was required for the posterolateral and anterolateral PMMA deposition, whereas stabilization of the axial displacement required up to 32% of the metastatically involved vertebrae. Cotten et al. reported partial or complete pain relief in 36 of 37 patients within 6–72 hours of PMMA injection (26). These good results did not depend upon the percentage of cement. Unfortunately, two of their patients had foraminal leaks with nerve root compression that required decompressive surgery.
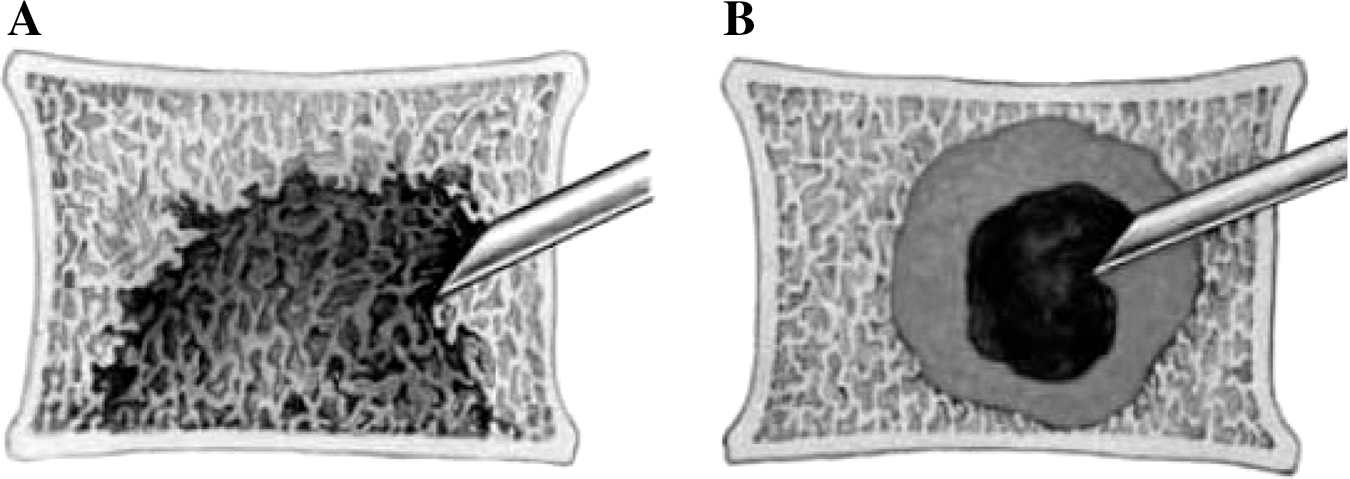
Illustration of vertebral body augmentation in case of metastatic lesion: for performing its function, injected bone cement should anchor in vertebral bone tissue (
The principal concern when vertebroplasty is used is related to cement extravasations, both local and pulmonary. Direct neurologic injury, cerebrospinal fluid fistula, and adjacent level fractures have been described (26). Local cement leakage is usually asymptomatic but sometimes can cause transient or chronic radiculopathy. Cement extruded into the spinal canal can also compress the spinal cord and cause long tract signs and myelopathy (18). This happens more frequently when vertebroplasty is used to treat patients with an angioma or osteoporosis (2%–5% and 1%–3%, respectively) and may be a result of increased PV destruction and/or poor general condition of the cancer patient (22). In general, PV is safe, with a complication rate of 1.7% to 10% when performed appropriately by an experienced surgeon (12). Meanwhile, open surgery complication rate is reported at a level of 20% (27). PV does not compete with open surgery; it complements current approaches for treatment of spinal metastases.
We have found several publications of successful cases of treatment of spinal metastases secondary to thyroid cancer with PV in the radiological and neurosurgical literature (28 –31). Nowadays, the surgical aspects of PV have been discussed meticulously and the problem of patient selection for the procedure is raised.
According to recently published final recommendations of Spine Oncology Study Group, using percutaneous techniques (PV and embolization) in the treatment of metastatic spinal tumors is considered as “strongly recommended.” A “strong recommendation” means that most, if not all, clinicians would want to use the intervention, patients would almost all want it, and policy makers should consider it being policy in most situations (32).
PV can also be successfully combined with chemotherapy, radiotherapy, radiofrequency ablation, neurodecompression, and instrumentation (30,33). It does not interfere with radiation therapy protocols and can be performed either before or after treatment (18).
In our two patients, standard treatment with PV for metastatic thyroid carcinoma was used. In our second patient, with advanced MTC, we also used transpedicular fixation for additional stability of the weakened segment. Although PV may be associated with severe complications, it appears to be well worth the risk in selected patients and instantly improves the quality of life (33).
Conclusion
PV is a minimally invasive spinal procedure and should be considered for patients with metastatic thyroid cancer with spinal metastases. PV when used for palliative treatment provides immediate and long-term pain relief and spinal stabilization that helps to prevent possible neurological complications. PV is a treatment option for the palliation of severe pain associated with some vertebral body metastasis, especially with often slow-growing metastatic thyroid cancer. It can be successfully combined with other therapies.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.