
Abstract
Background:
The ability of sialagogues to increase or decrease radiation induced-sialoadenitis and/or xerostomia after therapeutic administration of 131I is controversial. To evaluate this we measured the radiopharmacokinetics of 123I in the parotid glands (PGs) after its administration of lemon juice (LJ).
Methods:
A retrospective review was performed on all patients who had a salivary gland scan performed before 131I therapy between July 2008 and April 2009 at the Washington Hospital Center. Two hours after 123I was given orally, dynamic scintigraphy was initiated. Five milliliters of LJ was given 5 minutes later. Then, the patient was imaged for 1 hour (phase 1) at which point the sequence was repeated (phase 2). Twenty-three patients were studied. For each PG, the presence or absence of uptake was assessed, and based on background corrected counts, the mean, range, and standard deviation were determined for multiple radiopharmacokinetic parameters such as (i) percent radioiodine washout, (ii) time from LJ administration to re-accumulation of radioiodine to pre-LJ activity, and (iii) percent reduction in radiation absorbed dose to the PGs if LJ had been re-administered at the time the radioiodine activity re-accumulated to the pre-LJ activity.
Results:
The mean ± one standard deviation and range for percent washout were 84% ± 18% (35%–100%) and 83% ± 21% (37%–100%) in phase 1 and 2, respectively. The times from LJ to re-accumulation of the radioiodine to the pre-LJ activity were 21 ± 10 minutes (4–45 minutes) and 40 ± 14 minutes (12–62 minutes) for phase 1 and 2, respectively. The estimated percent reduction in radiation absorbed dose to the PGs following the first and second administration of LJ was 37% ± 14% (13%–93%) and 47% ± 16% (21%–97%), respectively.
Conclusions:
The washout of radioiodine from the PGs is rapid but transient. Early repeat administration may result in continued and cumulative reduction of radiation absorbed dose in the PGs.
Introduction
131
The objective of this study was to characterize the radiopharmacokinetics of radioiodine in the parotid glands (PGs) after LJ.
Methods
A retrospective review was performed on all patients who had a clinical salivary gland scan performed before 131I therapy for differentiated thyroid cancer between July 2008 and April 2009 at the Washington Hospital Center. Patients fasted for 4 hours before the start of the scan. Two hours after the oral administration of a capsule of 15–37 MBq (0.4–1 mCi) of 123I, a dynamic imaging sequence was initiated on a Siemens gamma camera using the protocol outlined in Table 1. Without moving the patient, 5 mL of Real Lemon Juice® (LJ) was given orally 5 minutes after the start of the acquisition. The patient was then imaged for another 60 minutes (phase 1). At 65 minutes after the initiation of the images, the patient was given a second bolus of 5 mL of LJ orally with imaging continuing for an additional 60 minutes (phase 2). Regions of interest were placed over each observed PG along with a background region (see Fig. 1). Background corrected time activity curves were obtained for each PG in each phase. Decay correction was not performed. For each PG and each phase, the mean, range, standard deviation, and confidence intervals were determined for (i) maximum percent washout relative to pre-LJ 123I activity, (ii) time from administration of LJ to nadir of washout of 123I, (iii) time from nadir to re-accumulation of 123I activity to pre-LJ 123I activity, (iv) time from administration of LJ to re-accumulation of 123I to pre-LJ 123I activity, and (v) ratio of 123I activity at 1 hour relative to pre-LJ 123I activity (see Fig. 2).
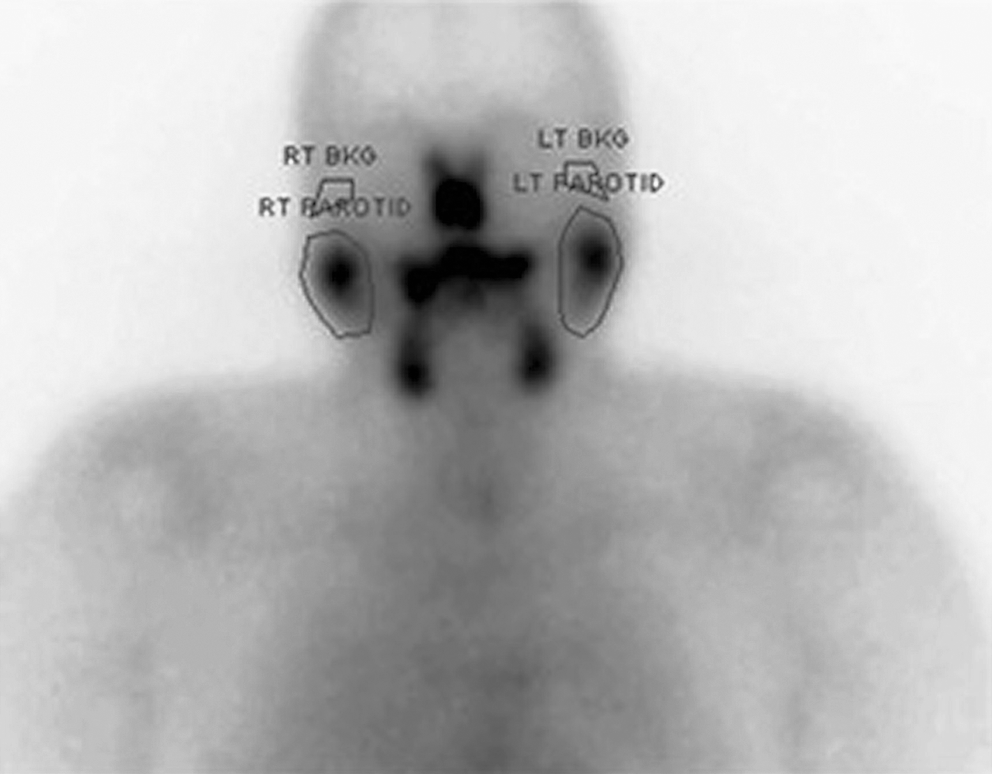
The regions of interest positioned over each parotid gland and the background regions placed superior to the respective parotid gland.
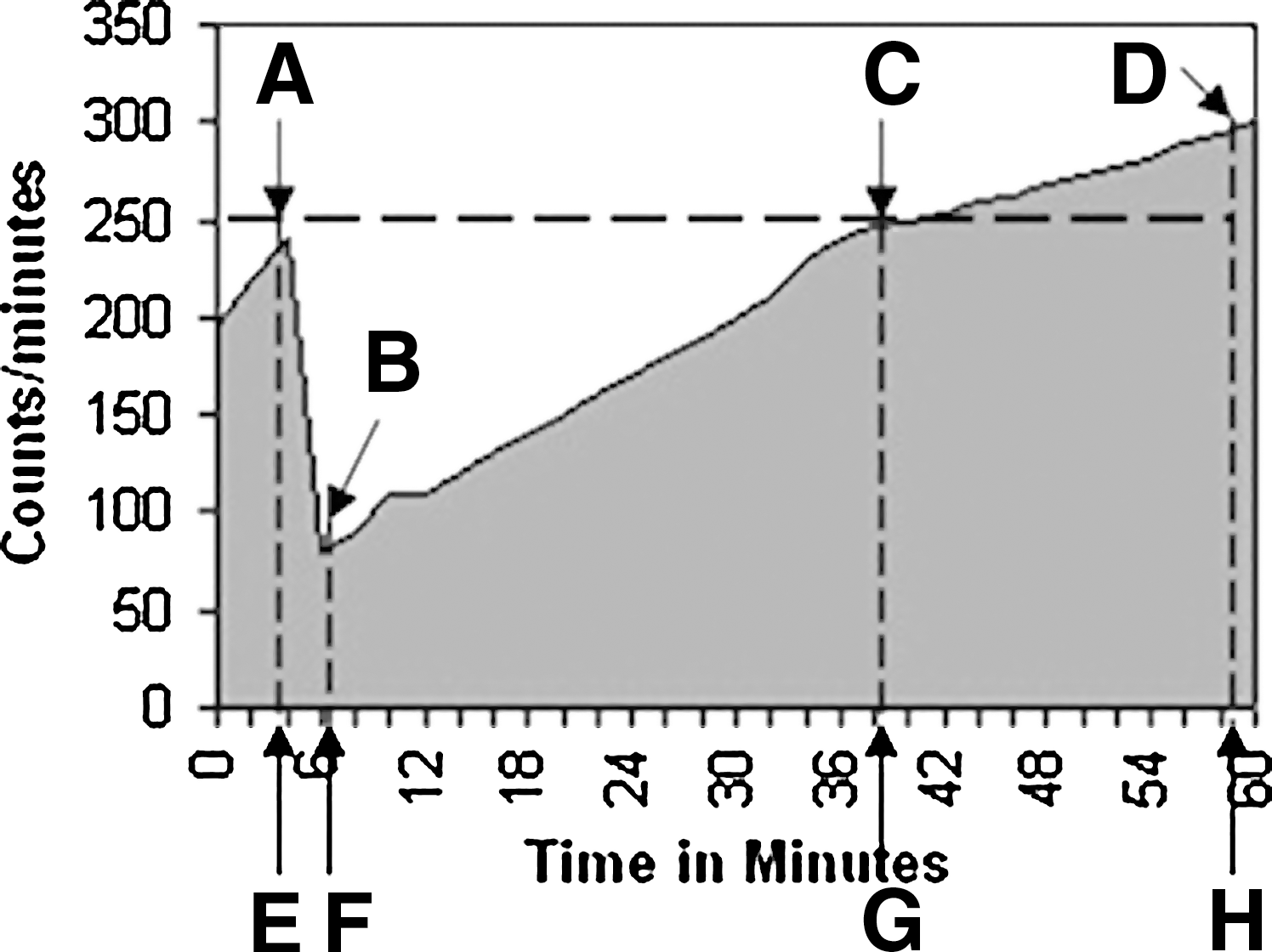
This figure demonstrates the time points used for the calculation of the radiopharmacokinetic parameters.
The relative reduction in radiation absorbed dose to the PGs secondary to the administration of sialagogues was estimated based on two assumptions (see Fig. 3). First, we assumed that if the LJ had not been administered, the radioiodine activity in the PGs would have remained at the same value as the value on the 5 minute image (baseline value), and, second, sialagogues would have been given again at a time interval equal to that required for the 123I in the PG to re-accumulate to the baseline value. It is important to note that we cannot calculate actual radiation absorbed dose. Rather we are estimating the percent reduction of radiation absorbed dose based on the above two assumptions. The submandibular glands were not evaluated for this study. This retrospective study was approved by the MedStar Institutional Review Board.

This figure shows the areas used to estimate the percent change in radiation absorbed dose to the parotid glands from the radioiodine after the administration of the LJ. The dark gray area represents the area under a typical time activity curve (TAC), with the latter representing the total counts from the radioactivity in the salivary glands during one phase. The hatched area reflects the total counts of radioactivity in the salivary glands based on the assumption that the radioiodine remained constant from the administration of LJ [point Area A = Area under the TAC reflecting the radioactivity exposing the salivary glands when LJ had been administered.
 Area B = Total area under the TAC reflecting the radioactivity exposing the salivary glands based on the assumption that the radioactivity remained constant between points A–C in Figure 2.
Area B = Total area under the TAC reflecting the radioactivity exposing the salivary glands based on the assumption that the radioactivity remained constant between points A–C in Figure 2.
 Area C = The relative reduction of radiation absorbed dose as a result of use of LJ. The estimated % change in radiation absorbed dose to the parotid gland was calculated as % reduction in radiation absorbed dose = ([Area B – Area A]/[Area B]) × 100.
Area C = The relative reduction of radiation absorbed dose as a result of use of LJ. The estimated % change in radiation absorbed dose to the parotid gland was calculated as % reduction in radiation absorbed dose = ([Area B – Area A]/[Area B]) × 100.
Results
A total of 29 patients had salivary gland scans available for review. The demographics of the patients are shown in Table 2. Six patients had no visible radioiodine activity in the PGs, of which two had no prior 131I treatments and four had one prior 131I treatment. These patients were not evaluated further. Thus, there were 23 patients who had evaluable radioiodine uptake. Sixteen, five, and two patients had no prior 131I therapy, one prior therapy, and two or more prior 131I therapies, respectively. In these 23 patients, 46 PGs were evaluated.
The data for the 123I radiopharmacokinetics in phase 1 and phase 2 are shown in Table 3. The mean decreases in radioactivity after LJ for phase 1 and phase 2 were 84% and 83%, respectively. The mean intervals from the administration of LJ to the return of the activity to that present before LJ administration was 21 minutes in phase 1 and 40 minutes in phase 2 (p < 0.0001). A typical time–activity curve for patients with PG uptake, washout, and re-accumulation is shown in Figure 4. Tables 4 and 5 demonstrate the parameters and p-values comparing right versus left individual PGs in phase 1 and 2, respectively. There were no significant differences in any parameter between the right and left PGs in both phase 1 and phase 2. Tables 6 and 7 present comparisons of the data for patients who had no prior 131I therapy and those who had at least one such therapy. At a p-value of <0.05, no statistical difference was noted regarding any parameter in both phase 1 and phase 2. In patients who were prepared with recombinant human thyrotropin injections, thyroid hormone withdrawal, or on thyroid hormone suppression, no statistical difference in any of the parameters was noted at the p < 0.05 level. Because the number of patients was low, a nonparametric method (Kruskal–Wallis one-way analysis of variance) was used to evaluate the differences.
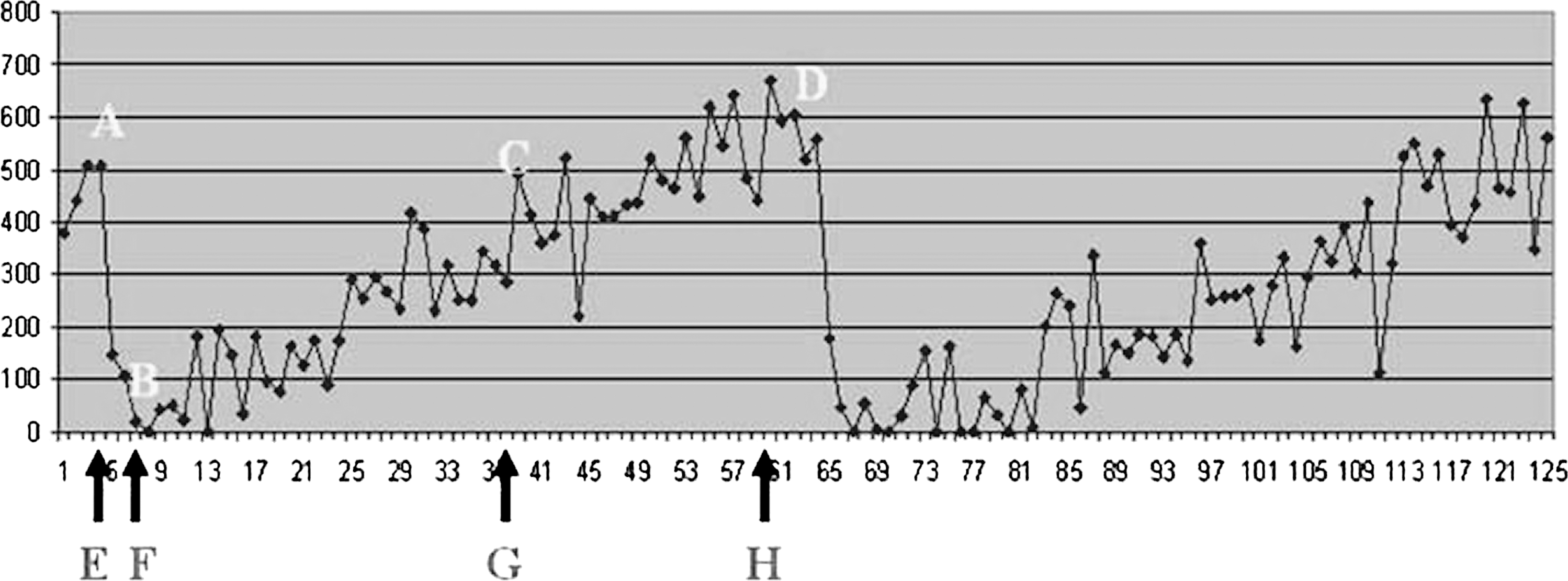
A typical background-corrected TAC demonstrating the response to the oral administration of LJ. The numbers on the X-axis are minutes, and the numbers on the Y-axis are counts/minute. The notations are the same as described in Figure 2. Note the prompt response to LJ with subsequent re-accumulation and the similar response following the second administration of LJ at ∼65 minutes into the acquisition.
p-Values were calculated using a matched-pairs t significance test. For each observation, the differences between phase 1 and phase 2 were calculated and tested against the null hypothesis that the difference is zero. The boldface entries are significant at the 0.05 level or lower.
p-Values were calculated using a matched-pairs t significance test. For each observation, the differences between right and left were calculated and tested against the null hypothesis that the difference is zero. The boldface entries are significant at the 0.05 level or lower.
p-Values were calculated using a matched-pairs t significance test. For each observation, the differences between right and left were calculated and tested against the null hypothesis that the difference is zero. The boldface entries are significant at the 0.05 level or lower.
p-Values were obtained from the Wilcoxon signed-rank test based on the null hypothesis that there is no difference between the two groups. A nonparametric test was used because of the small sample size in the “Prior Therapy” group. The boldface entries are significant at the 0.05 level or lower.
p-Values were obtained from the Wilcoxon signed-rank test based on the null hypothesis that there is no difference between the two groups. The boldface entries are significant at the 0.05 level or lower.
Discussion
This study examined the radiopharmacokinetics of radioiodine in the PGs from 2 to 3 hours (phase 1) and from 3 to 4 hours (phase 2) after administration of 123I. At the start of both phases patients received LJ. After LJ was administered, the radioiodine in the PGs rapidly declined in ∼4 minutes followed by re-accumulation of the radioiodine to the same amount of radioactivity that was present when the initial LJ was administered. This period of re-accumulation was ∼20–40 minutes. The radiopharmacokinetics of radioiodine in phase 1 and 2 were similar.
Although the actual radiation absorbed dose to the PGs cannot be calculated and although the study was not controlled by administering placebo in place of LJ, an estimate of the percent reduction in radiation absorbed dose to the PGs can be calculated with two assumptions, namely, repeat LJ was administered at the time the radioiodine re-accumulated back to the same amount of radioactivity that was present when the initial LJ was administered, and if the initial LJ had not been administered, no further radioiodine would have accumulated. On the basis of these assumptions, the percent reduction in radiation absorbed dose during this period would be as much as 37%–47%, and these estimates may be conservative because it is possible that the radioiodine would have continued to accumulate if the initial LJ has not been administered.
The time from either administration of LJ or the nadir after administration of LJ to the re-accumulation of radioiodine to baseline in phase 2 was longer than the comparable time in phase 1 (<0.0001). Although this may in part be a result of a higher uptake of radioiodine in the salivary glands at the start of phase 2 relative to phase 1, the mean percent reduction in radiation absorbed dose to the PGs was also greater in phase 2 than in phase 1 (<0.0001). This was true regardless of whether the data for the right and left PGs were pooled or the comparisons were made for the right or left PG individually.
It is not clear if prior treatment with 131I affected the results since there were a relatively small number of patients who could be compared. Similarly, attempts to determine if preparation of the patient with prior recombinant human thyrotropin administration differed from preparation with thyroid hormone withdrawal did not yield significant differences, again possibly the result of the small number of patients.
On the basis of the results of this study, we disagree with the recommendation of Nakada et al.'s that sialagogues be withheld for the first 24-hour period after 131I therapy (4). While withholding sialagogues for the first 24-hour period after 131I therapy may be better than a schedule of administering sialagogues every 2–3 hours when the patient is awake, our data suggest that more frequent administration of sialagogues will significantly reduce the radiation absorbed dose to the PGs. In addition, our results would support Silberstein's approach of a continuous administration of sialagogues while the patient is awake and then intermittently after retiring (6). Of note, however, the low incidence of 131I induced sialoadenitis reported by Silberstein could in part or in toto be the result of the prophylactic administration of dexamethasone to all his patients. Nevertheless, our results support the argument for more frequent administration of sialagogues.
Liu et al. (8) concluded that “the salivary stimulation with vitamin C [the same active stimulant of salivary glands as in LJ] at any time after 131I administration has only a limited effect on salivary absorbed dose in thyroid cancer patients.” They had four groups of patients who were administered 100 vitamin C orally at 1, 5, 13, and 25 hours after 131I, and the patients received additional vitamin C every 4 hours thereafter for the next 6 days, excluding the hours between 2 and 6 a.m. On the basis of the results of our study in which we noted re-accumulation of radioiodine 20–40 minutes after administration of LJ, it is likely that an interval of 4 hours between administration of vitamin C is too long to have a meaningful effect on the exposure of the PG to radioiodine.
The present study has its positive attributes and limitations. One positive attribute is that this study used radioiodine rather than 99mTechnetium pertechnetate (99mTc04). While the pharmacokinetics of 99mTc04 in the salivary glands may be similar to radioiodine, they may not be identical (9 –11). Second, the assessment of the radiopharmacokinetics of iodine in the PGs were performed during a time period after the oral administration of radioiodine when the concentration of radioiodine in the blood is typically near its peak level (12). Third, it was shown that the effects of LJ did not diminish after a second dose.
The study has several limitations. It only evaluated a 2-hour period starting 2 hours after the administration of 131I. The effect of sialagogues for a more prolonged period of several more hours or even several days is not known. Also, only one dose and one sialagogue were evaluated. Different doses of the LJ used or different sialagogues might produce different results. Third, assumptions were required to estimate the potential reduction in radiation absorbed doses. However, we consider our assumptions to be conservative since the formula used was based on PG radioactivity reaching a plateau, not continuing to rise, after the time the initial LJ was administered. It is very likely that had LJ not been administered, radioactivity would have continued to rise. In addition, if an earlier time for the administration of the LJ had been selected or if the sialagogues had been given continuously, the estimated percent reduction of radiation absorbed dose could be even greater. Another limitation of the study is that it was not placebo (in place of LJ) controlled. Finally, this study only focused on the PGs, and thus this study did not evaluate the submandibular or sublingual salivary glands.
On the basis of the data presented in this study, we recommend that sialagogues not be withheld for the first 24-hours period after administration of a therapeutic dose of 131I, but that sialagogues should be administered far more frequently than every 2–3 hours such as every 15–30 minutes or even continuously and that the sialagogues should not only be administered when the patient is awake but also intermittently throughout the night and possibly the next day. While this may result in a poor night sleep for the patient, we believe this will result in a significant reduction of the radiation absorbed dose to the patient's salivary glands. The exploration and use of a longer acting sialagogue might also be valuable especially while the patient is as sleep. In regard to when sialagogues should be initiated, this study does not address that, but this study indicates that sialagogues initiated at least 2 hours after the administration of a therapeutic dose of 131I can reduce the radiation absorbed dose to the PGs. Further study is warrant to assess the radiopharmacokinetics in the first 2 hours.
Footnotes
Acknowledgment
This study was under written in part by generous donations from grateful patients.
Disclosure Statement
The authors declare that no competing financial interests exist.