
Abstract
Background and Objective:
124I emits a positron and can be imaged with a positron emission tomography (PET) scanner. The objective of this study was to compare the ability of diagnostic 124I PET images versus 131I planar whole-body imaging in detecting residual thyroid tissue and/or metastatic well-differentiated thyroid cancer (WDTC).
Methods:
Patients were recruited prospectively for this study who (i) had WDTC, (ii) were suspected of having metastatic WDTC, and (iii) were referred for 131I whole-body dosimetry. The prescribed activity was 1–2 mCi (37–74 MBq) and 1.7 mCi (62.9 MBq) for 131I and 124I, respectively. For each image, one blinded reader (D.V.N.) categorized every focus of 131I and 124I radioiodine uptake as 1 = definite physiological uptake/artifact, 2 = most likely physiological uptake/artifact, 3 = indeterminate, 4 = residual thyroid tissue/metastases in the neck/bed, 5 = most likely metastases, or 6 = definite metastases. Foci categorized as 4, 5, or 6 were considered positive. When available, foci categorized as 4, 5, or 6 were correlated with other diagnostic studies.
Results:
Of the 25 patients, 8 patients (32%) had more positive foci on 124I images than on 131I, of which 3 patients to date have had metastases confirmed in one or more of the additional positive 124I foci. 124I demonstrated the same number of foci as on 131I in 16 patients (14 with no positive foci, and 2 with two positive and five positive foci each). One patient had one additional positive focus on 131I not seen on 124I, which has not yet been confirmed as a metastasis. A total of 97 positive foci were identified on either 124I or 131I. 124I identified 49 positive foci not seen with 131I, and 131I identified one positive focus not seen with 124I.
Conclusion:
Relative to 131I planar whole-body imaging, 124I PET identified as many as 50% more foci of radioiodine uptake suggestive of additional residual thyroid tissue and/or metastases in as many as 32% more patients who had WDTC.
Introduction
124
Methods
Patients were eligible for this study who (i) had histologically proven WDTC, (ii) were suspected of having metastatic WDTC (e.g., elevated thyroglobulin levels, recent fine-needle aspiration positive for cancer, and/or suspicious enlarging mass on physical or imaging study), (iii) were referred for 131I whole-body dosimetry in anticipation of 131I therapy, and (iv) were over 18 years of age. The prescribed activities for the imaging studies were 1–2 mCi (37–74 MBq) and 1.7 mCi (63 MBq) for 131I and 124I, respectively. Patients who were prepared by withdrawal of thyroid hormone had their 131I dosimetry performed first. Those prepared with recombinant human thyrotropin (rhTSH) injections were randomized to receive either 131I or 124I first. Studies were performed within 10 days of each other. Acquisition and processing techniques are summarized in Tables 1 and 2. Images that were used for interpretation were performed at 48 hours after administration of either 131I or 124I with the exception of one patient who received 124I and was imaged at 24 hours and then withdrew from the study.
MIE, Medical Imaging Electronics.
SAC, segmented attenuation correction; CT, computed tomography; OSEM, ordered subsets expectation maximization; TF, time of flight.
For each image, one blinded reader (D.V.N.) categorized every focus of 131I and 124I radioiodine uptake using the following grading system: 1 = definite physiological uptake/artifact, 2 = most likely physiological uptake/artifact, 3 = indeterminate, 4 = residual thyroid tissue/metastasis in the neck/bed, 5 = most likely distant metastasis, or 6 = definite distant metastasis. Foci that were categories as 4, 5, and 6 were considered positive. When available, foci were correlated with other diagnostic imaging studies. This prospective study was approved by the MedStar Institutional Review Board and the Radioactive Drug Research Committee.
Results
Twenty-five patients were evaluated, and the patient characteristics are noted in Table 3. Seventeen patients were prepared with rhTSH and eight with thyroid hormone withdrawal. The patient specific results are shown in Table 4. Of the 25 patients, 8 patients (32%) had a greater number of positive foci observed on the 124I images than on the 131I images (see Fig. 1), which was statistically significant by Wilcoxon matched-pairs signed-ranks test (p < 0.02). Three of these eight patients have had metastasis confirmed in one or more of the additional positive 124I foci. 124I images demonstrated the same number and location of foci as on 131I images in 16 patients of whom 14 had no positive foci and 2 had positive foci on both sets of images (two and five foci, respectively). One patient had one additional positive focus on 131I images that was not seen on 124I images. To date, this has not been confirmed as either a metastasis or a false-positive.
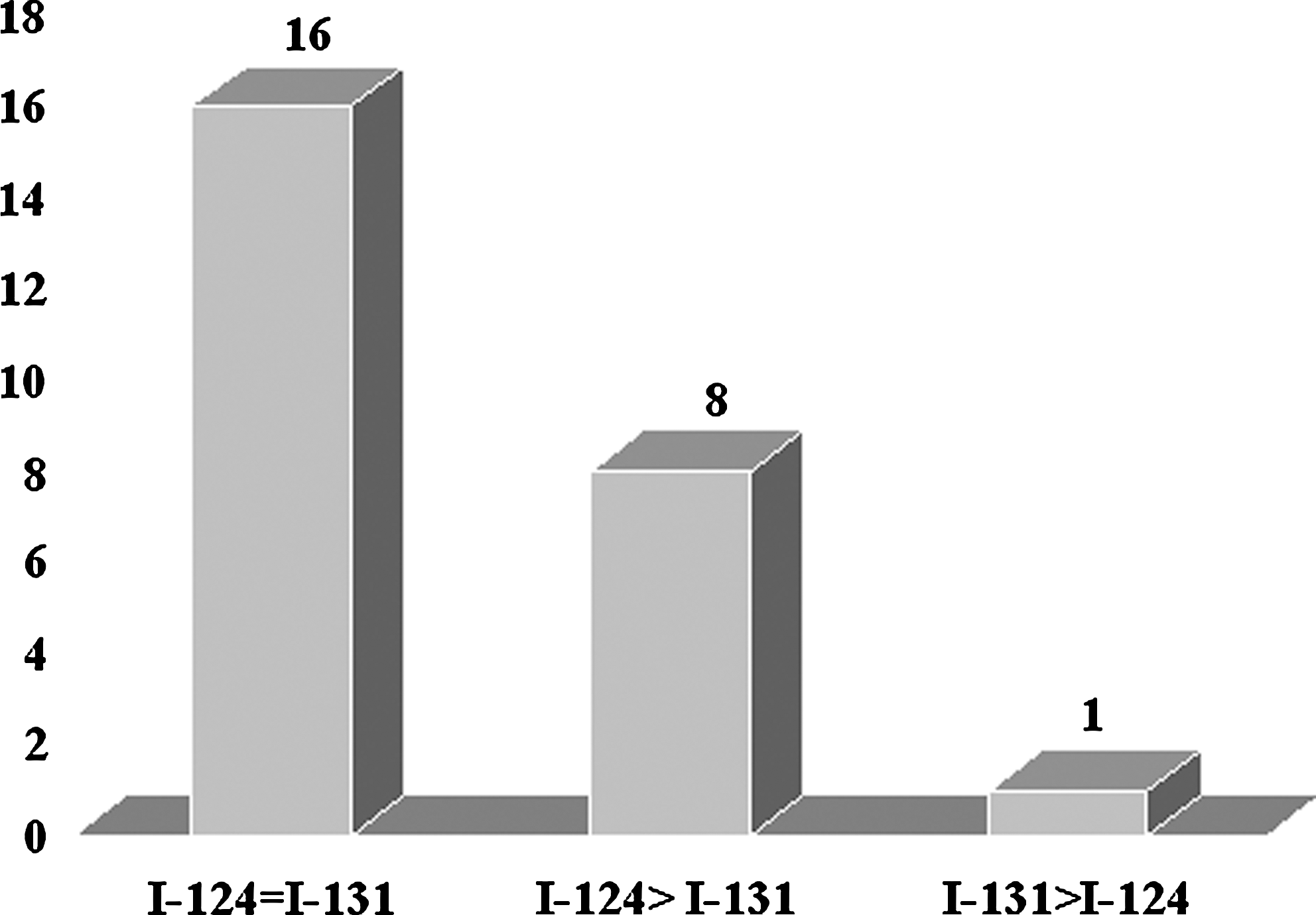
Of the 25 sets of 124I PET images and 131I planar whole-body images evaluated, 8 (32%) 124I images demonstrated more foci of radioiodine uptake than observed on the 131I images. Sixteen patients demonstrated either the same number of foci or no foci on the 124I images as demonstrated on the 131I images. Only one patient had one more focus of radioiodine uptake identified on the 131I images not detected on the 124I images. PET, positron emission tomography.
rhTSH, recombinant human thyrotropin; THW, thyroid hormone withdrawal.
Patient numbers do not necessarily represent the order that the patients were recruited. × represents the type of preparation the patient had.
In regard to the number of individual foci of uptake observed (see Fig. 2), a total of 97 positive foci were identified on either 124I or 131I. 124I identified 49 positive foci not identified on 131I, and 131I identified one positive focus not identified on 124I. Examples of 131I and 124I images are shown in Figures 3 and 4. The difference between the number of foci detect with 124I versus 131I was statistically significant using the binomial regression (p < 0.0001).
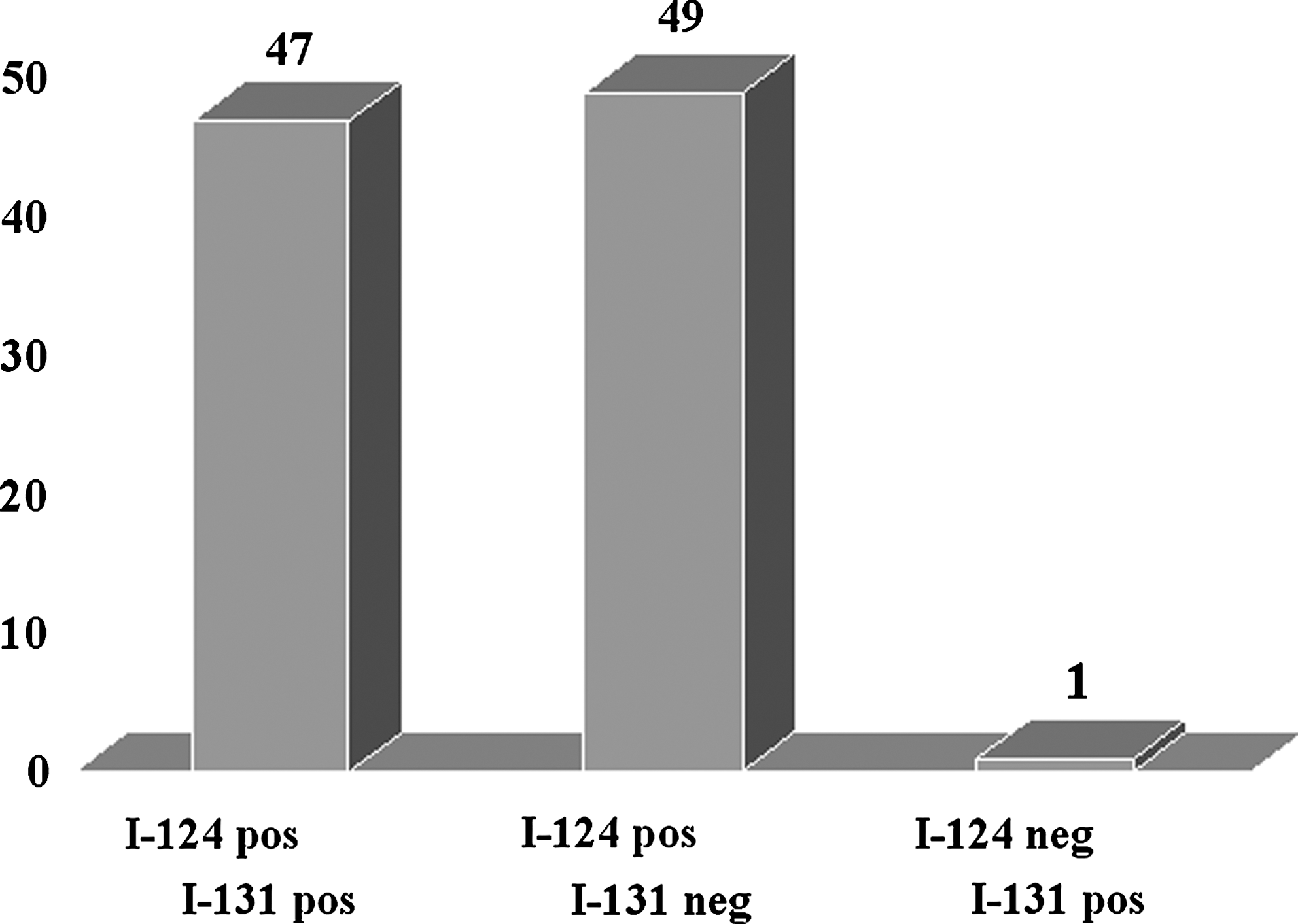
Of the 25 sets of 124I PET images and 131I planar whole-body images evaluated, 97 foci categorized as residual tissue and/or metastatic WDTC were detected on either 124I and/or 131I images. Forty-nine foci (51%) were detected only on 124I images; only one lesion was detected on the 131I images that was not detected on the 124I images. WDTC, well-differentiated thyroid cancer.
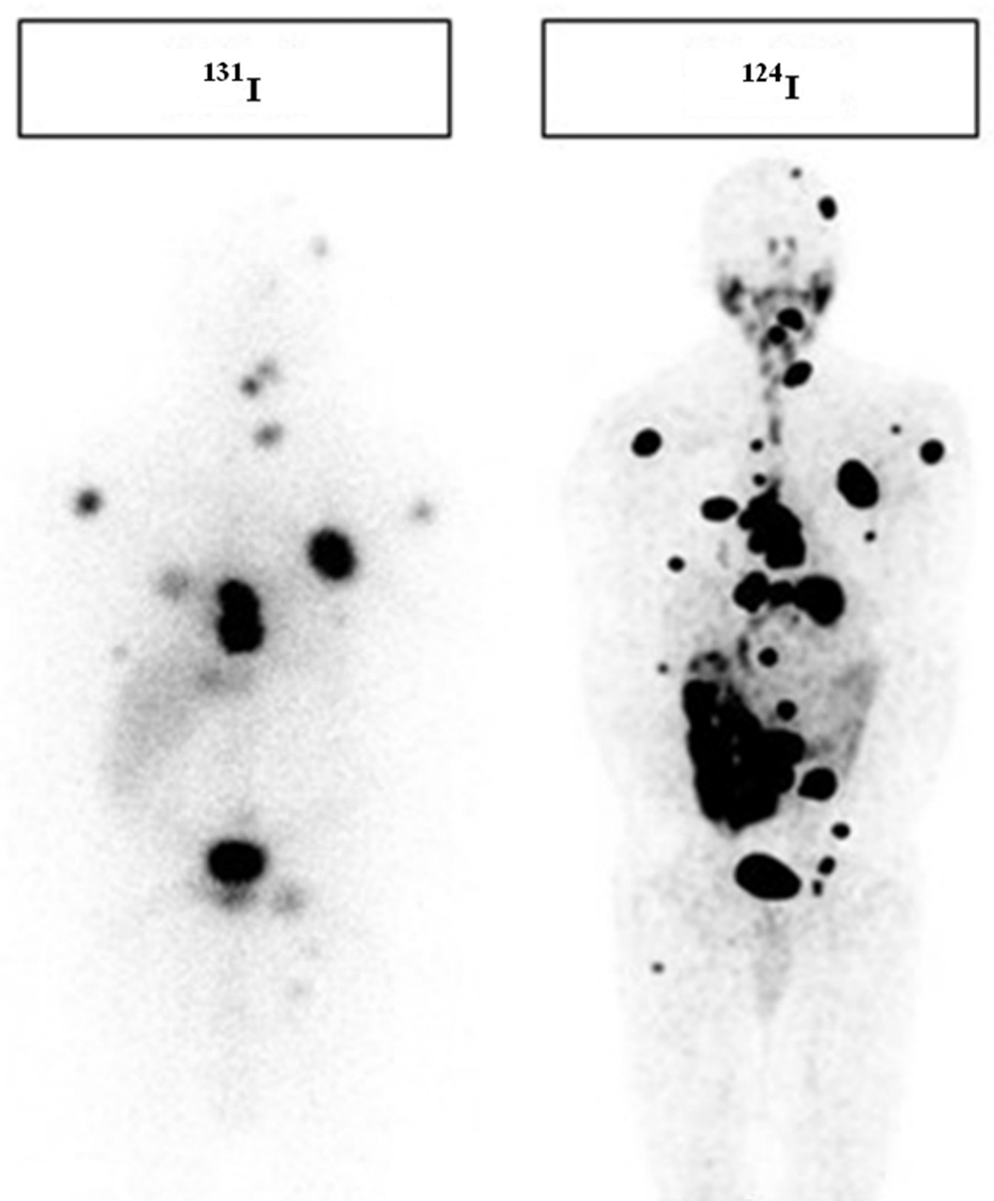
Both images were obtained in the same patient. The image on the left is an anterior planar 131I whole-body image demonstrating ∼18 foci of 131I uptake indicative of metastatic WDTC. The image on the right is the anterior124I PET image from the maximum intensity projection demonstrating multiple additional foci of 124I uptake not detected on the 131I images suggesting metastatic WDTC.

(
For the patients prepared with thyroid hormone withdrawal (n = 8), 131I was performed first per the approved protocol. Of these eight patients, five patients had more foci detected on the 124I scan than on 131I scan, two patients had no focus or the same number of foci detected on either scan, and one patient had one more lesion detected on 131I scan not detected on the 124I scan. Of the 17 patients who were prepared with rhTSH injections and were randomized regarding whether they were administered 1311 or 124I first, 10 had 131I and 7 patients had 124I administered first (see Table 4). Of the 10 patients who were administered 131I first, 9 had no uptake on either scan and 1 had uptake on the 124I scan not seen on the 131I scan. Of the 7 patients who were administered 124I first, 4 had no uptake on either scan, 2 had uptake seen on the 124I scan not seen on 131I scan, and 1 had the same uptake seen on both scans.
Discussion
This study demonstrates the superiority of 124I PET images relative to 131I planar whole-body imaging in the detection of residual thyroid tissue and/or metastasis in patients who have WDTC, and we attribute this superiority to at least three factors. First, 124I is a positron emitting radionuclide, which can be imaged using a PET scanner, which in turn results in significantly reduced background noise and improved spatial and contrast resolution. Second, PET images, like computed tomography (CT) images and magnetic resonance imaging, are tomographic images. Not only does this allow the images to be reviewed slice by slice, but this also allows the removal of radioactivity in front of and behind the area of the body being evaluated—one of the mechanism for improved contrast resolution. Although not used in this study, the PET tomographic images can be fused with CT and/or magnetic resonance imaging.
Although Phillips et al. first reported the use of 124I for the treatment of thyroid carcinoma in 1960 (1), only a few recent studies have been published comparing 124I versus 131I in the detection of residual thyroid tissue and/or metastases secondary to WDTC in humans (7,8). In 2004, Freudenberg et al. demonstrated additional findings on 124I images relative to 131I images in 2/12 (17%) patients. Sixty foci were identified on the 124I images and 58 on the 131I images (7). In 2008, Phan et al. reported that 8 of 20 (40%) patients had foci of 124I uptake without corresponding foci of 131I uptake identified on 131I planar whole-body imaging. Evaluation by the number of foci detected was not reported (8).
Although these two reports together with our study collectively demonstrate the superiority of 124I PET images relative to 131I planar images, there is variability in the degree of superiority [e.g., 17% (6), 32% (present report), and 40% (8)]. The reasons for the modest difference may be secondary to a difference in the incidence of residual thyroid tissue and/or metastatic disease in the patient populations of the respective facilities, the relatively low number of patients in all the studies, the time from dosing and/or duration of imaging, and instrumentation, to name only a few of the variables.
Finally, our study as well as the other studies have limitations. First and as already noted, our study has a limited number of patients. However, despite the relatively small number of patients, the superiority of 124I PET relative to 131I planar imaging was statistically significant. Second, all foci categorized as 3, 4, or 5 are not necessarily residual thyroid tissue or metastases. Third, artifact heretofore unknown may not have been recognized. For example, recently Abdul-Fatah et al. reported a shine-through artifact in the trachea with 124I (9). Fourth, none of the studies compared 124I PET-CT with either 123I or 131I single photon emission computer tomography (SPECT)–CT. Although two recent studies by Schmidt et al. (10) and Spanu et al. (11) reported that SPECT-CT performed with either 123I or 131I is superior to radioiodine planar imaging, comparison of 124I PET with planar radioiodine imaging is reasonable because to our knowledge most facilities perform radioiodine planar imaging and do not routinely perform whole-body radioiodine SPECT-CT scans. Nevertheless, if radioiodine SPECT-CT imaging of the entire body becomes routinely available and performed, then a future study comparing 124I PET-CT to 123I and/or 131I SPECT-CT is warranted, although we would expect 124I PET to be superior to either 123I or 131I SPECT-CT. As Alavi and Basu have pointed out, the latter suffers from (i) poor spatial and contrast resolution, which reduces its ability to detect smaller foci with low concentrations of radiotracers, and (ii) limited speed relative to PET-CT in screening the entire body, which will increase imaging time significantly (12). The final limitation is that this study did not evaluate cost, altered management, or changed patient outcomes.
In regard to the possibility of stunning reducing the ability of the radioiodine that was administered second to detect the same or more foci, we do not believe this was a problem because of two reasons. First, the prescribed activities of 131I and 124I were 74 MBq (2 mCi) and 63 MBq (1.7 mCi), respectively. We believe stunning at these low amounts of radioactivity is infrequent. Second, in the seven patients who were prepared with thyroid hormone withdrawal, the 131I was administered first as required by the approved protocol. Despite this, 124I scans still detect more foci than 131I scans in five of these patients. This would argue against stunning, or if stunning was present, then 124I PET scans may have been even more sensitive than 131I scans. For the patients prepared with rhTSH, these patients were randomized regarding the radioiodine isotope that they received first, and as already noted, no statistical difference was demonstrated as a result of the radioiodine that was administered first; however, again, the number of patients is low.
Conclusion
Diagnostic 124I PET imaging is superior to diagnostic 131I planar imaging in identifying a statistically greater number of foci of residual thyroid tissue and/or metastases in statistically more patients with WDTC.
With the present data available, the scientific and commercial communities should partner and pursue a new drug application with the Food and Drug Administration in the United States to expand the availability of 124I.
Footnotes
Acknowledgments
This study was supported by grants from the Latham Fund, Genzyme Corporation, and IBA Corporation.
Disclosure Statement
The authors declare that no competing financial interests exist.