
Abstract
Background:
Malignancies, primary or metastatic, and infections are the main causative factors that should be included in the differential diagnosis of cervical adenopathy.
Summary:
We present a 56-year-old woman who was admitted to our department because of a supraclavicular mass. A neck dissection was performed and two different masses were excised. The histopathological examination showed that the larger mass (measuring 5 cm) was a block of lymph nodes with metastatic papillary carcinoma of the thyroid. In the adjacent fibroadipose tissue, two lymph nodes with metastatic carcinoid tumor were found. The smaller mass (measuring 2 cm) was a lymph node with metastatic carcinoid tumor. The patient underwent total thyroidectomy with ipsilateral radical neck dissection. Histopatological examination of the thyroid gland showed a lesion of papillary carcinoma, measuring 0.6 cm. No further lesions of carcinoid were found.
Conclusions:
To our knowledge, this is the first report of a coexistence of metastatic papillary thyroid carcinoma and intestinal carcinoid tumor in cervical lymph nodes.
Introduction
Carcinoid tumors are slow-growing neoplasms with distinct biologic and clinical characteristics, deriving from the enterochromaffin/neuroendocrine cell system, which is scattered throughout the body (3). Carcinoid tumors represent ∼0.49% of all malignancies, and the incidence is estimated from 0.65 to 4.48 per 100,000 population per year (3). A recent analysis of 10,878 carcinoid tumors from the Surveillance, Epidemiology, and End Result Program (SEER) of the National Cancer Institute found that 64% of all carcinoids originate in the gastrointestinal tract and 28% originate in the lungs or bronchi, reflecting the high density of enterochromaffin/neuroendocrine cells in the mucosa of the digestive system and the respiratory epithelium. Carcinoids of the small intestine have the strongest predilection to metastasize among carcinoids of various locations. Regional lymph nodes, liver, lung, peritoneum, and pancreas are the most common locations where carcinoid tumors of the small intestine metastasize to. Here we present a distinctly unusual patient who had simultaneous metastases of PTC and carcinoid tumor of the small intestine in the cervical nodes.
Patients and Methods
A 56-year-old woman was admitted to the First Department of Otorhinolaryngology—Head and Neck Surgery of Aristotle University of Thessaloniki for evaluation and treatment of a supraclavicular cervical mass that had been noted 6 months previously and was gradually increasing in size. Her medical history indicated that 3 years previously she had undergone a surgical resection of two carcinoid lesions of the small intestine with metastasis in the mesentery presentation. She denied symptoms of carcinoid syndrome and was being closely followed for her history of intestinal carcinoid. Examination of the neck revealed a soft, nontender, well-defined, mobile 5-cm mass located in the supraclavicular cervical region. The remainder of the neck examination including the thyroid was normal. Common serum tests, including serotonin and calcitonin levels, and white cell count levels of inflammatory markers were normal. The urinary excretion of 5-hydroxyndol acetic acid was not elevated. Thyroid function tests were also normal.
Computed tomography and magnetic resonance imaging of the neck revealed a 3 × 4.5 × 6 cm mass in the left lateral neck suggestive of a neurofibroma of the pneumonogastric nerve or the left brachiplex. The T2-weighted magnetic resonance images of the mass were of low signal intensity with areas of necrosis (Fig. 1).
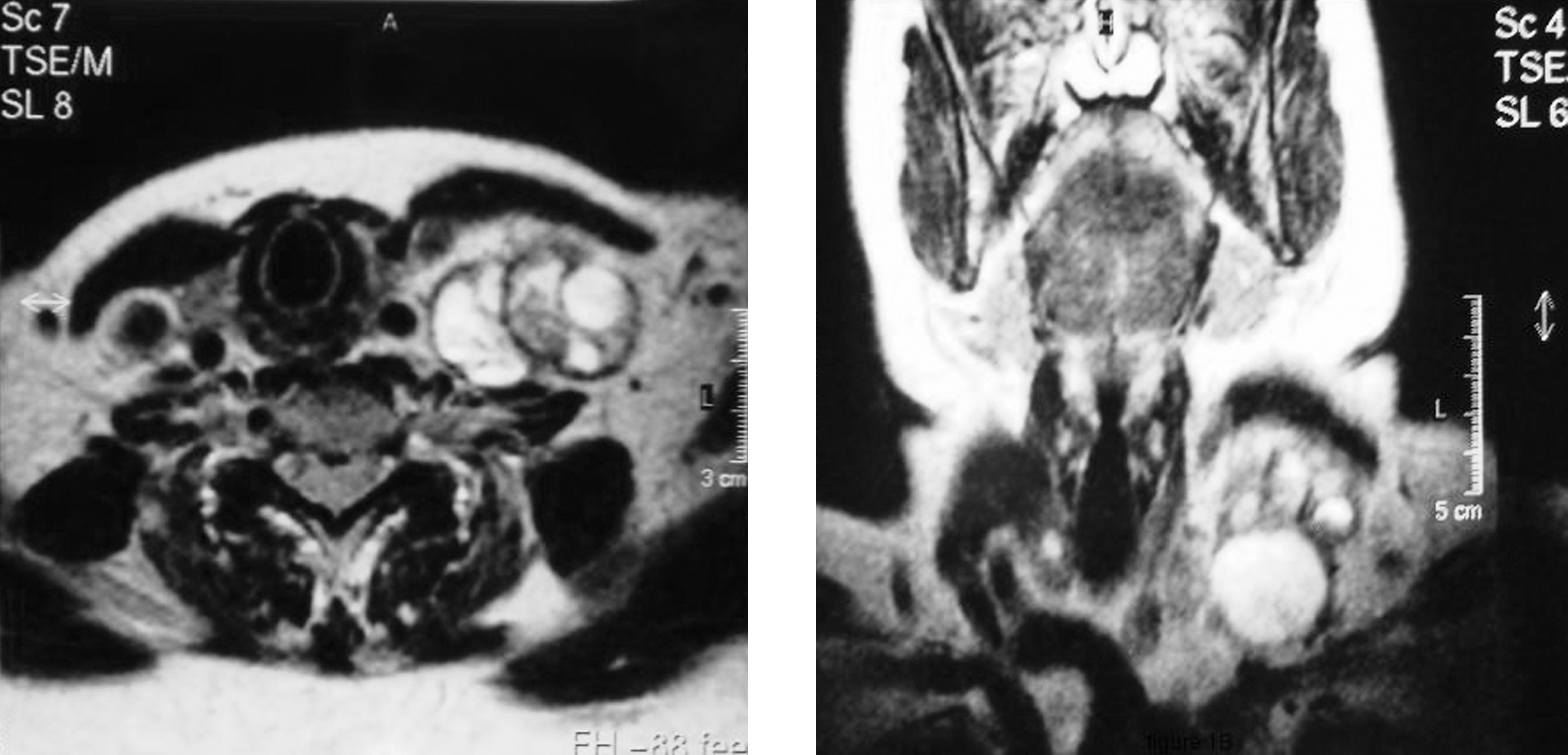
T2-weighted magnetic resonance images show a 3 × 4.5 × 6 cm mass with low signal intensity in the left cervical region.
Surgery was performed to resect the mass. Two distinct masses were observed and excised. Both were smooth, well circumscribed, and mobile, one being 5 cm in diameter and the other ∼2 cm in diameter. Histopathological examination showed that the larger mass was a lymph node containing metastatic PTC (Fig. 2A, B). The smaller mass was a lymph node with metastatic carcinoid tumor (Fig. 3A). The neoplastic cells were medium sized and arranged mainly in compact nests and rosettes. The nuclei were hyperchromatic, with small nucleoli and mild mitotic activity. On immunohistochemical staining, they were positive for neuron-specific enolase, chromogranin, synaptophysin, and cytokeratin cam5.2 (Fig. 3B–D). They were not positive for thyroglobulin or thyroid transcription factor-1. They were positive for the proliferation marker Ki-67/mib-1, reaching 8% in the most actively proliferating areas. The Ki-67 nuclear protein is a cellular marker for proliferation, determining the growth fraction of a given cell population (4). Two additional lymph nodes with metastatic carcinoid tumor were found in fibroadipose tissue next to the larger mass.
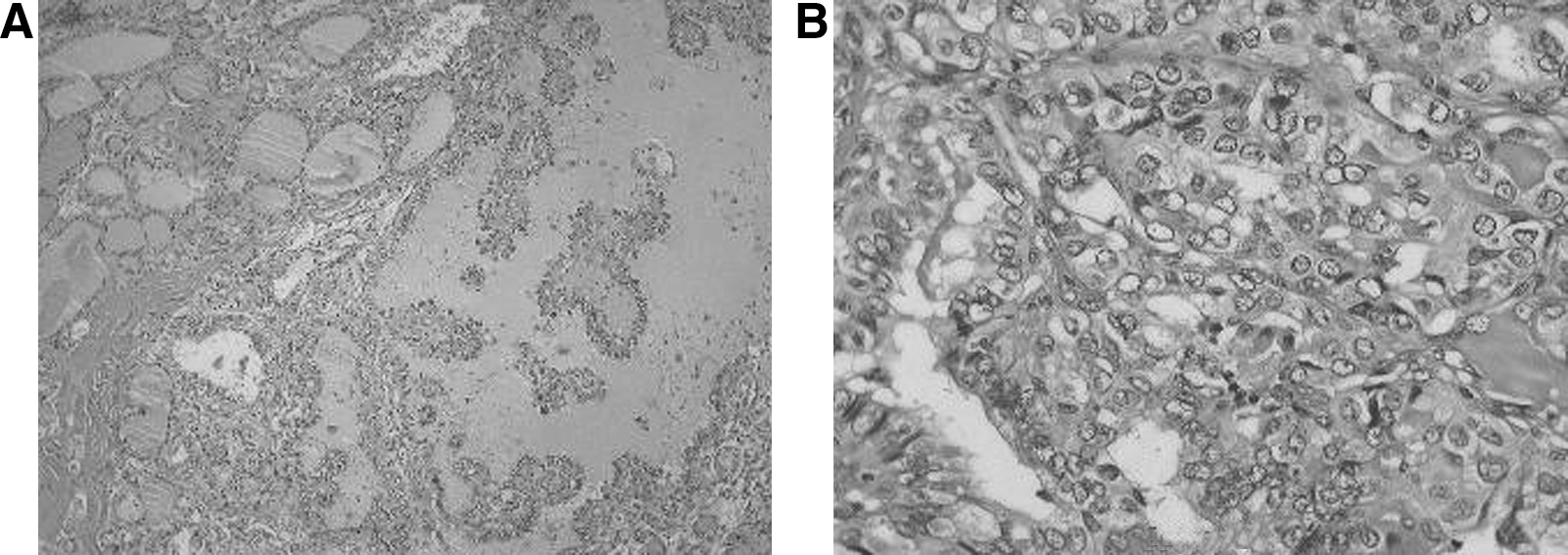
A representative section of the larger neck mass showing metastatic papillary thyroid carcinoma. (

Representative sections of the smaller neck mass showing metastatic carcinoid tumor. (
More than 90% of carcinoid tumors contain high concentrations of somatostatin receptors, which can be imaged with their radiolabeled ligands. Therefore, octreoscan scintigraphy was performed, which showed activity in the region of the left submaxillary gland. Total thyroidectomy followed with a radical ipsilateral neck dissection, and excision of the left submaxillary salivary gland and pretracheal lumph node group was performed. Histopathological examination of the thyroid showed a 0.6-cm PTC in the left lobe but no carcinoid lesions in the operative specimen including the submaxillary gland. One month after surgery the patient was treated with 150 mCi radioactive iodine (RAI). One year after thyroidectomy, diagnostic iodine-131 total body scan was normal. The patient remains disease free.
Discussion
The simultaneous occurrence of two different metastases in the neck lymph nodes is rare (4,5). To our knowledge, the present report is the first description with histopathological documentation of synchronous cervical metastases from a PTC and carcinoid of small intestine. It should be noted that the neck metastases occurred in the same group of lymph nodes.
Ten percent to 30% of PTMCs recur clinically as metastasis in the lateral cervical nodes and usually appear as solid masses in that region (6). Initial presentation of a carcinoid of the small intestine with a cervical mass is an extremely rare entity and only five cases have been reported in the literature (4,7,8). Metastatic disease in the neck may be accompanied by symptomatology of carcinoid syndrome. Two of the five reported cases presented with symptoms of carcinoid syndrome, the major clue that such metastases have occurred. In the few patients in whom this was reported the cervical metastases did not seem to have a particularly adverse effect on the prognosis. This seems to be the case in our patient who developed cervical metastasis at 3 years after resection of the primary tumor without systemic symptoms or recurrence within 1 year of its resection.
The association of gastrointestinal carcinoids with secondary malignant neoplasms has been recognized. Habal et al., in a review of over 5000 cases of gastrointestinal carcinoids, reported that the rate of coexistent primary malignancies ranged from 12% to 46%, with an average of 17% (10). Among gastrointestinal carcinoids, small bowel carcinoids have the highest rate of secondary primary malignancies (29%–52%). The majority of these secondary primary tumors are gastrointestinal and genitourinary adenocarcinomas, but a variety of other histologic types have been also reported. The reason for the increased risk of a second primary malignancy in patients with carcinoid tumors remains unknown. However, one of the predominant theories is that this malignant predisposition is related to the tumorigenic effects of the various neuroendocrine peptides elaborated and secreted by the carcinoid's neuroendocrine cells (10).
In summary, we report a patient with simultaneous metastasis in the cervical lymph nodes from PTMC and a carcinoid tumor that, based on the patient's history, probably came from an intestinal carcinoid. As PTC commonly metastasizes to the lateral cervical nodes, this is rare for carcinoid. It is even rarer for metastases from these two tumors to occur at the same time and in approximately the same location.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.