
Abstract
Background:
Papillary thyroid carcinoma (PTC) is the most common endocrine malignancy with indolent clinical course and good prognosis. Brain metastases are extremely rare and the average survival time after diagnosis has been reported to be around 12 months.
Summary:
We here report a 69-year-old patient who was admitted to the emergency room in January 2000 with progressive dizziness, headache, and vomiting. Five years before admission the patient underwent partial thyroidectomy for goiter. On admission, a diagnostic evaluation that included brain magnetic resonance imaging showed multiple brain lesions, and a stereotactic biopsy demonstrated a metastatic carcinoma from primary PTC, with the neoplastic cells staining for thyroglobulin. Total thyroidectomy was then performed, which showed colloid goiter and a PTC metastasis on a cervical lymph node. The patient received 200 mCi of radioactive iodine (131I) with suppressive therapy with
Conclusions:
To our knowledge, this is the first report of a 10-year-survival case of brain metastases from PTC, despite this being a bad prognostic factor. A combined approach of surgical excision, 131I, whole-brain radiotherapy, and gamma knife radiosurgery was successful to treat metastases derived from primary tumor.
Introduction
Patient
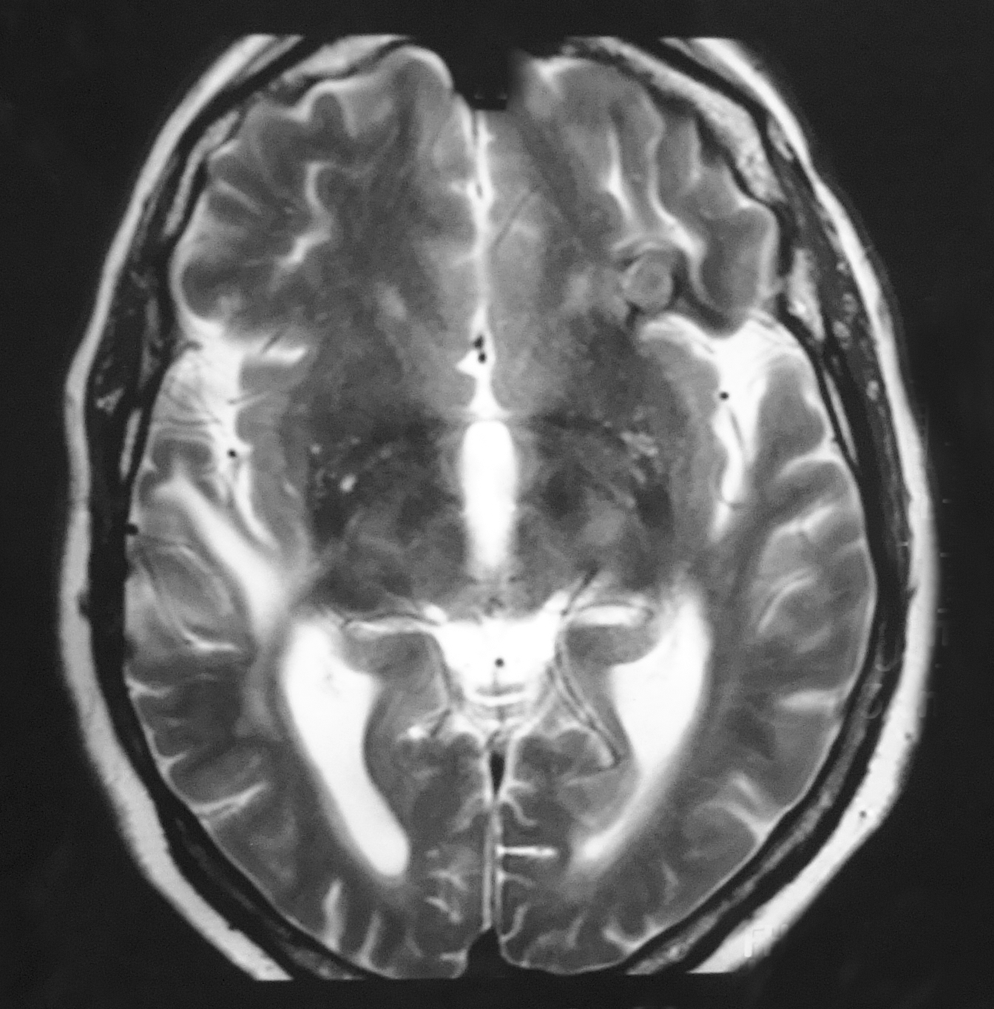
A 60-year-old woman presented at the emergency room in June 2000 with progressive dizziness, headache, and vomiting. She had a history of partial thyroidectomy for treatment of a goiter at 5 years before admission. However, histopathological report was unavailable. A diagnostic evaluation that included magnetic resonance imaging (MRI) showed two lesions, one in each cerebral hemisphere (Fig. 1). Histopathological analysis of stereotactic biopsy of the brain lesions was diagnostic for metastatic carcinoma from a primary PTC. The neoplastic cells showed positive immunohistochemistry staining for thyroglobulin. She was referred to a neurosurgeon to have the brain lesions ressected, but she refused this procedure at that time. Thereafter, she underwent total thyroidectomy. Pathology results showed a colloid goiter and a cervical lymph node with atypical cells, with fine chromatin pattern, papillary structures, and nuclear features of PTC. The patient received 200 mCi of radioactive iodine (131I), which showed strong cervical uptake, compatible with thyroid remnants, together with the two already identified brain metastatic lesions (Fig. 2). Subsequently, she was treated with suppressive therapy with

Axial magnetic resonance imaging after gadolinium administration showing irregular enhancing mass in both cerebral hemispheres (2000).
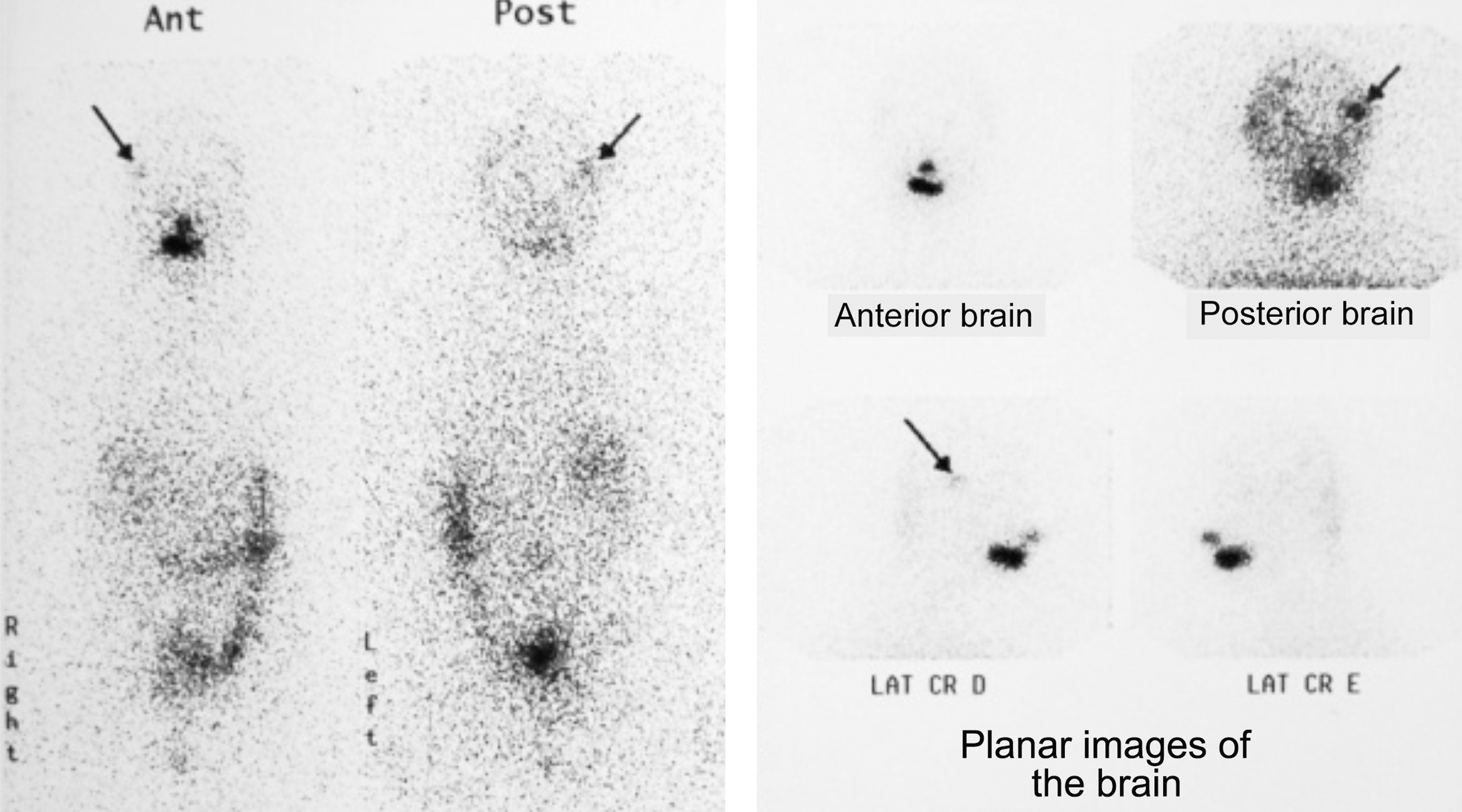
The first whole-body 131I scan showing evidence of intracranial metastases and cervical uptake (2001). Arrows show metastatic lesions.
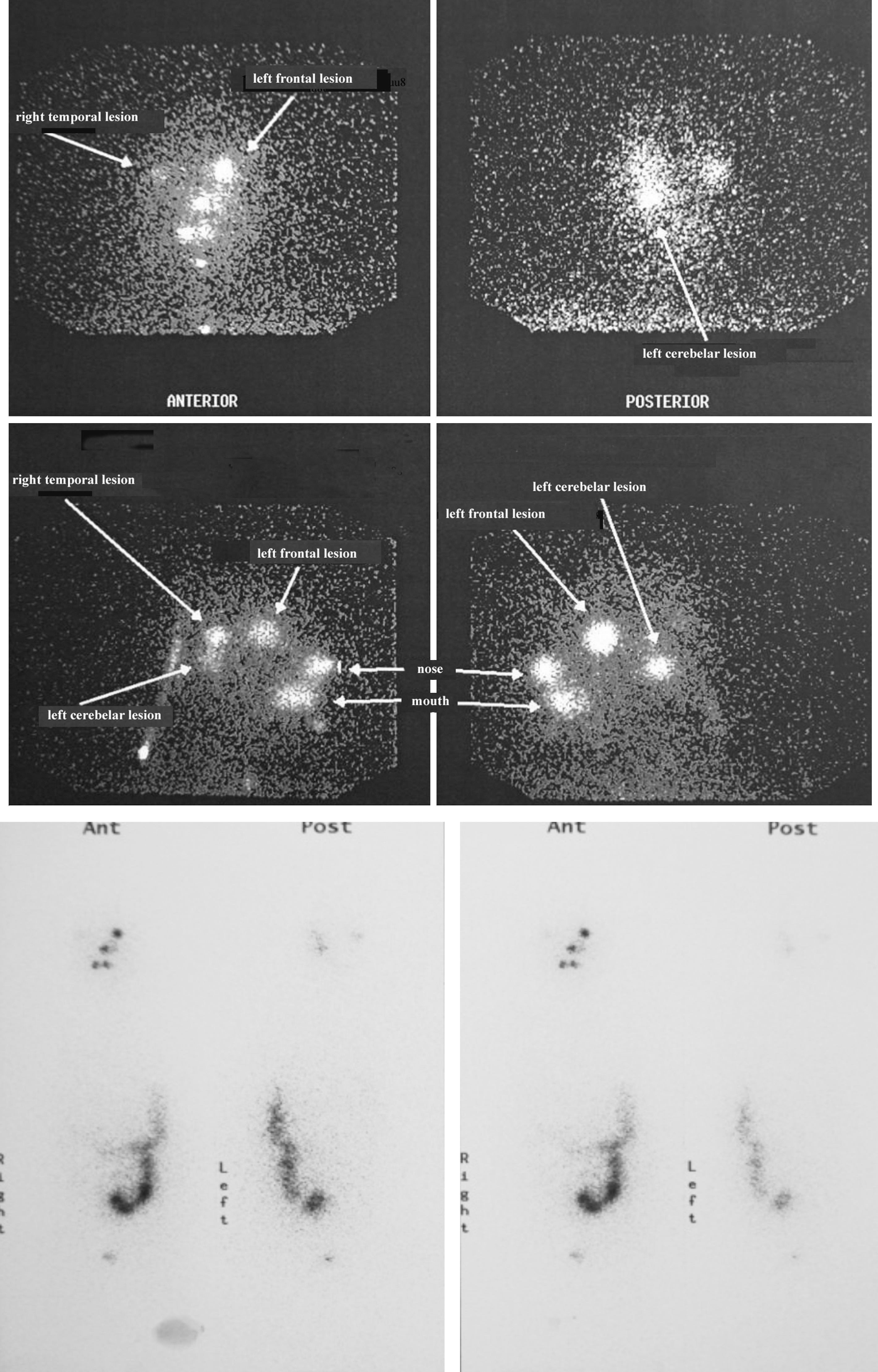
Whole-body 131I scan showing brain uptake (2003).
Because of the persistence of high levels of thyroglobulin, and brain images in MRI images, the patient underwent partial surgical removal of brain metastases, because complete resection was not achievable. Next, the patient was submitted to whole-body radiotherapy (WBRT) with a dose of 44 Gy, followed by gamma knife radiosurgery (GKR). GKR was performed in 2006 and 2008, 15 Gy twice, because of tumor growth. Subsequently, serial MRI scans performed at 6-month intervals revealed partial size reduction of the brain metastases (Fig. 4). The patient received oral dexamethasone 2 mg four times a day, beginning the day before 131I therapy or WBRT, and lasting for 3 months after treatment.
Magnetic resonance imaging showing partial reduction of brain metastases (2009).
The patient has been followed up for 10 years without change in biochemical tests of liver and kidney function or hemogram. In addition, she has been clinically free of intracranial hypertension and performing well her daily activities.
Discussion
PTC constitutes around 80% of all thyroid malignancies. Based on the Surveillance, Epidemiology, and End Results Program of the National Cancer Institute data, the incidence of PTC has increased significantly over 30 years (1973–2003) (6,7). In general, the prognosis is excellent and the reported survival rates for nonmetastatic lesions are 97.8% at 5 years and 94.9% at 10 years (2). The presence of distant metastases diminishes the survival rates to 37% and 24% at 5 and 10 years, respectively. Lungs are the most common site of distant metastases. Brain metastases are uncommon, comprising 0.1%–5% of all distant metastases, and few reports have been described (1,3,8,9). Risk factors for distant metastasis of PTC include male sex, advanced age, histological grade, and extra-thyroidal invasion at the onset. Other risk factors are completeness of surgical resection of the primary tumor and nuclear DNA content (1). In addition, the reported survival interval ranges from 14 months to 7 years and all patients survived for at least 1 year (5).
The optimal management of PTC consists of total or near total thyroidectomy and ablation of the thyroid remnants with 131I. The presence of brain metastasis is a negative prognostic factor; therefore, treatment must be tailored to the individual patient. Current guidelines are for surgery, when feasible, as the first option, followed by radioiodine or external radiotherapy (10,11). Several treatment modalities have been used in a limited number of patients with intracranial metastatic PTC, including surgical resection for accessible lesions, external beam radiation, GKR, and radioiodine therapy (1,12).
WBRT has been commonly used in the management of patients with incomplete resection of brain tumors. The use of GKR has not been well defined for this pathology and only scattered data have been reported (13). However, it is minimally invasive and thus enhances tumor control. It has also been suggested that the combined use of WBRT and GKR in comparison to each modality alone improves tumor management (1).
The role of 131I therapy in the management of DTC is well established (14). To date, chemotherapy has not been recommended in patients with brain metastasis from thyroid carcinoma (1,12,15,16). Given the susceptibility that small brain tissue growth can cause significant symptoms, the use of recombinant TSH stimulation of 131I uptake (instead of a several weeks of thyroid hormone withdrawal) is a reasonable approach, especially for patients with tumors localized near vital regions (12).
The most frequent early side effect is acute radiation sickness. This usually occurs within 12 hours of 131I administration and has been reported in up to 73% of cases (17). Another common side effect is sialoadenitis, which occurs shortly after treatment and lasts for several days. Brief, asymptomatic bone marrow suppression may arise within the first month of treatment. Permanent or severe marrow suppression has been reported when the blood radiation dose was high, but has not been observed when the radiation dose to the blood was less than 200 rad (17). Finally, some patients report pain in metastases following treatment. This presumably is due to radiation-induced swelling and is analogous to radiation thyroiditis (17). Although our patient received 1.2 Ci 131I therapy (44.4 GBq), she did not have any significant pain.
External beam radiation for cerebral metastases can also cause complications such as cerebral edema and transtentorial herniation (18). Steroids have been shown to decrease both the amount of radiation-induced brain edema of 131I therapy and external beam therapy (18,19). How steroids reduce brain edema associated with brain metastases is unclear. It appears that steroids stabilize the capillary endothelial membrane, thus preventing serum proteins and other substances from crossing it, or they prevent the release of enzymes by the lysosomes, which produce deleterious effects on adjacent brain tissue (17,20). Some authors recommend prophylactic glycerol rather than corticosteroids, because of the possibility of decreased iodine uptake from corticosteroids (12,17) and caution should be taken to prevent rapid worsening of tumor growth during treatment.
Conclusion
To our knowledge only a limited number of studies focused on PTC with brain metastases. Although there has been a general consensus that brain metastases are associated with poor prognosis, here we report, for the first time, a patient who survived for 10 years. This was achieved with resection of surgically accessible lesions associated with high doses of 131I therapy, whole-brain radiation external therapy, and the GKR.
Although guidelines for clinical practice cannot be derived from a report, it illustrates how four different modes of treatment can be used to promote asymptomatic and prolonged survival.
Footnotes
Acknowledgments
This work was partially supported by grants from CAPES, CNPq, and FAPEMIG (Brazil).
Disclosure Statement
The authors declare that no competing financial interests exist.