
Abstract

Medullary thyroid cancer (MTC) can present with many histologic variants and be difficult to diagnose. Cervical lymph node metastases occur early in the disease and approximately half of MTC cases will develop distant metastases. There have been 10 reports describing dedifferentiated MTC with low or absent serum calcitonin (1). Additionally, our review of the literature also found references to six more patients with similar profiles (2). Here we report a unusual patient with a typically elevated serum calcitonin when he presented with MTC but much lower serum calcitonin concentrations when he developed substantial metastatic disease.
The patient was a 67-year-old man who presented with a right-sided neck mass and was referred to our institution to rule out lymphoma. His family history was unremarkable for thyroid or other endocrine disease. The right neck mass was at the level of the hyoid bone (level III). Preoperative serum calcitonin was 1084 pg/mL (normal range 0.0–11.5 pg/mL) and Carcinoembryonic Antigen (CEA) was 119.5 ng/mL (normal range for nonsmokers 0.5–2.5 ng/mL). Evaluation for rearranged during transfection (RET) mutations was negative.
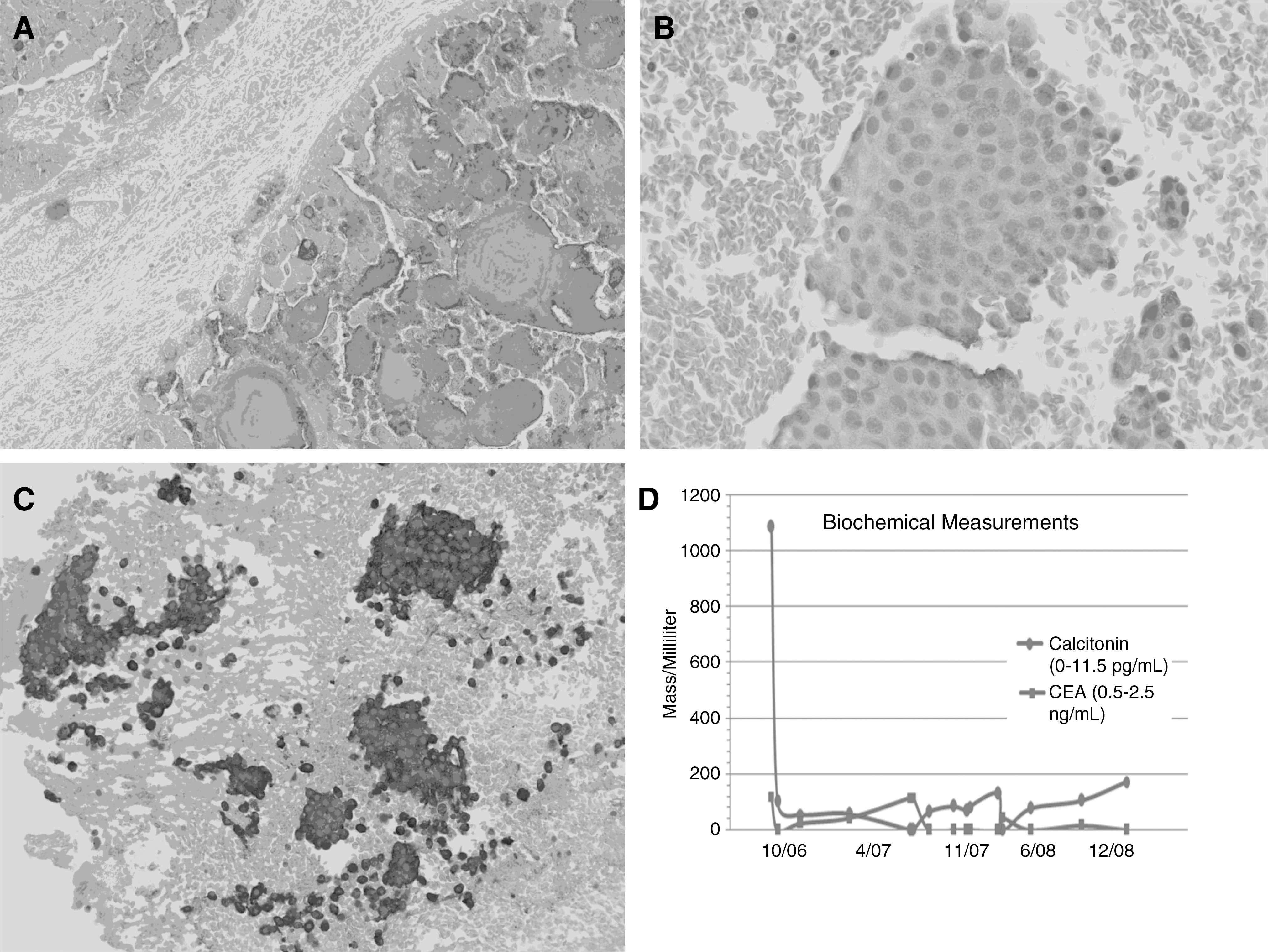
Fine-needle aspiration biopsy (FNA) of his right-sided neck mass was consistent with MTC. Stains performed were positive for chromogranin, synaptophysin, thyroid transcription factor 1, and calcitonin. Total thyroidectomy with bilateral modified radical neck dissection with central neck dissection was performed. Five out of 10 lymph nodes on the right were positive for MTC and extracapsular extension was present. Three positive nodes for MTC were taken from the central compartment. None of 10 nodes taken from the left neck were positive for malignancy. The primary MTC was 2.5 cm and it extended to within 1 mm of the margin of the thyroidectomy specimen (Fig. 1A).
(
The postoperative serum calcitonin was 101 pg/mL and the serum CEA was 23.9 ng/mL. Three months after surgery the serum calcitonin was 55.3 pg/mL. Six months postsurgery it was 57.1 pg/mL and serum CEA was 43.1 ng/mL (Fig. 1D). One year after his initial surgery, the patient returned with right-sided supraclavicular adenopathy. Ultrasound-guided FNA was performed and it revealed carcinoma with neuroendocrine features. In comparison with the previous tumor, there was a similar cytological appearance. Immunohistochemical stain for calcitonin was weak (Fig. 1B). The patient's serum calcitonin was 74.2 pg/mL with a CEA of 115.5 ng/mL. Radical resection of right supraclavicular fossa was performed. His postoperative calcitonin was 64.9 pg/mL.
Three months after the second surgery, there was a second recurrence. The calcitonin was 84.4 pg/mL. Ultrasound-guided FNA was positive for malignant cells consistent with the previous carcinoma. This was confirmed by strong immunoreactivity for chromogranin (Fig. 1C). Revision right central neck dissection was performed. The postoperative calcitonin was 83.1 pg/mL. The patient underwent treatment with external beam radiation therapy and his calcitonin climbed to 130 pg/mL.
At last follow-up, the patient had evidence of recurrence by ultrasound and a calcitonin of 76.2 pg/mL. Serial dilutions of his serum established that these calcitonin measurements are accurate and not artificially low by virtue of an assay hook effect. Slides from his three resections were sent for staining with antibody for calcitonin-gene-related peptide (CGRP). There was weak to no staining in all samples and it was not clear that the staining procedure was successful. The patient ultimately succumbed to his disease.
Routine measurements of serum calcitonin are considered to be an integral part of the diagnostic evaluation of thyroid nodules and the diagnosis of MTC. Serum calcitonin is a sensitive and specific indicator of disease recurrence in postoperative follow-up of patients with MTC. Calcitonin is elevated above 50 pg/mL in nearly all primary and metastatic MTC. On rare occasions, this cancer can present with serum calcitonin values that are relatively low or within the normal range (1,2). Although our patient had an original presentation with a markedly elevated serum calcitonin of 1084 pg/mL, he returned <1 year after radical surgery with documented metastases but a serum calcitonin that was <100 pg/mL. Typically, similar patients would have serum calcitonin in the thousands (3,4).
As reported by Sand et al. (5), it may be possible that rare forms of MTC have mutations in the calcitonin/CGRP gene that might predispose to normal or relatively low serum calcitonin concentrations. Our patient's tumor was associated on presentation with markedly elevated serum calcitonin concentrations, but when he had clinical recurrence of his tumor the calcitonin staining by immunohistochemistry in the metastases was weak and the serum calcitonin elevated but quite low considering his metastatic burden.
Our patient indicates that in rare instances the serum calcitonin level is a poor guide to the true extent of recurrent MTC. In a small percentage of patients with MTC its value at initial diagnosis is misleadingly low. When serum calcitonin is unremarkable or incongruous with the clinical impression, FNA, a determination of RET proto-oncogene mutations, imaging tests, testing for CEA, CGRP, and chromogranin, and a high degree of clinical suspicion necessary to diagnose and manage MTC.
Footnotes
Acknowledgments
Serum for CGRP was kindly provided to Dr. Deraedt by Dr. Walter Born, Balgrist, Switzerland. Dr. Deraedt (Leuven, Belgium) kindly performed CGRP immunostaining of our slides.
Disclosure Statement
All authors declare that they have no competing interests that may create a conflict of interest with the information presented in this article.