
Abstract
Background:
Radioactive iodine (RAI) remnant ablation has been used to eliminate normal thyroid tissue and may also facilitate monitoring for persistent or recurrent thyroid carcinoma. The use of RAI for low-risk patients who we define as those under age 45 with stage I disease or over age 45 with stage I or II disease based on American Joint Committee on Cancer (AJCC) 6th edition, or low risk under the metastases, age, completeness of resection, invasion, size (MACIS) staging system (value <6) is controversial. In this extensive literature review, we sought to analyze the evidence for use of RAI treatment to improve mortality and survival and to reduce recurrence in patients of various stages and disease risk, particularly for those patients who are at low risk for recurrence and death from thyroid cancer.
Methods:
A MEDLINE search was conducted for studies published between January 1966 and April 2008 that compared the effectiveness of administering versus not administering RAI for treatment of differentiated thyroid cancer (DTC). Studies were grouped A through D based on their methodological rigor (best to worst). An analysis, focused on group A studies, was performed to determine whether treatment with RAI for DTC results in decreased recurrences and improved survival rates.
Results:
The majority of studies did not find a statistically significant improvement in mortality or disease-specific survival in those low-risk patients treated with RAI, whereas improved survival was confirmed for high-risk (AJCC stages III and IV) patients. Evidence for RAI decreasing recurrence was mixed with half of the studies showing a significant relationship and half showing no relationship.
Conclusions:
We propose a management guideline based on a patient's risk—very low, low, moderate, and high—for clinicians to use when delineating those patients who should undergo RAI treatment for initial postoperative management of DTC. A majority of very low-risk and low-risk patients, as well as select cases of patients with moderate risk do not demonstrate survival or disease-free survival benefit from postoperative RAI treatment, and therefore we recommend against postoperative RAI in these cases.
Introduction
The 2009 updated American Thyroid Association (ATA) guideline for management of DTC recommends postoperative radioiodine ablation for AJCC (6th edition) stages III/IV disease, stage II disease in patients younger than age 45 years (and selected patients 45 years or older), and select cases of stage I disease, especially those with multifocal disease, nodal metastases, extrathyroidal, or vascular invasion and/or more aggressive histologies (4). The 2006 European consensus guideline risk stratifies patients into very low-risk, low-risk, or high-risk groups according to the AJCC TNM staging system and recommends RAI for patients in the high-risk group, including stage III/IV disease, stage II disease in patients younger than age 45, or those with incomplete tumor resection. They also recommend RAI for select cases in the low-risk group, including patients with stage I or stage II disease (in those over age 45) who did not have a complete surgery or lymph node dissection, age under 18 years, or tumor size between 1 and 4 cm with no metastases (5). However, the effectiveness of RAI for improving outcomes of patients with DTC has been challenged (6,7), particularly its use in low-risk patients with small tumors. Little is known about which of these asymptomatic, nonpalpable thyroid carcinomas, whose incidence is rising due in part to increased detection of small thyroid carcinomas (8), require remnant ablation therapy. A growing body of evidence on RAI side effects, including secondary malignancies, has also contributed to the debate (9,10).
The RAI literature for treatment of thyroid cancer has several deficiencies. First, the lack of randomized controlled trials evaluating the effectiveness of remnant ablation is well established (11). Second is the use of as many as 16 staging systems (12). Third, there is the lack of agreed-upon definitions for “low risk” versus “high risk,” so it is difficult to compare the outcomes for different stages/risks from across studies (13). Fourth, despite the histological heterogeneity of DTC (14), some studies pool histological types in their analyses, whereas others do not, even though the histological types behave differently. This may be important because iodine uptake can vary depending on histologic type, and prognosis, in general, is poorer for patients with pure follicular thyroid carcinoma (FTC) and Hurthle cell tumors (15). Fifth, there are ethnic and geographic differences in total incidence and incidence of different histological types of DTC, which have not been accounted for in analyses. Sixth, recurrence and death from thyroid cancer can be seen many years after the initial diagnosis; therefore, outcome data are dependent on duration of the studies, which is variable. Lastly, methods for detecting recurrence of disease have improved over time. Newer studies use more sensitive thyroglobulin (Tg) assays and high-resolution ultrasonography to detect recurrence of disease, whereas older studies use whole-body scanning (WBS) alone, which is less sensitive (16,17). This makes it difficult to compare study outcomes.
The goal of this study was to collect and analyze the evidence for utility of RAI treatment to improve mortality and survival and to reduce recurrence in patients with low-risk DTC. We systematically examined the peer-reviewed literature published since 1966 to identify the risks and benefits of using RAI in the context of disease stage and risk.
Methods
A MEDLINE search was conducted for English-language meta-analyses, systematic reviews, decision analyses, randomized controlled trials, nonrandomized prospective studies, retrospective studies, and cross-sectional studies published between January 1966 and April 2008, using Medical Subject Headings or key words, when appropriate, as search terms (Appendix A). The reference lists of related reviews were also manually reviewed. Each article was evaluated for potential inclusion by at least two reviewers. Disagreements were resolved through discussion. Studies that compared the effectiveness of administering versus not administering RAI for treatment of thyroid cancer in human subjects and those that provided outcome data such as recurrence (Tg level, locoregional, or distant metastasis), mortality, and survival were included in the study. Only English-language full-text articles were included. Exclusion criteria were (i) outcomes only on medullary thyroid carcinoma, (ii) studies lacking a control or nonexposed group, and (iii) studies that only assessed Tg level immediately after administering RAI to determine if initial therapy was successful. Some articles contain overlapping data, because the same author published data on the same cohort over multiple points in time. We retained the most recent article only, except when earlier studies presented analyses that were not repeated in the most recent study; in the latter cases, we also retained earlier articles.
Additionally, subgroup analyses were performed to determine whether the results of recurrence rates would be impacted by duration of patient follow-up as well as method of detection of recurrence. Studies were segregated into those with <10 years of follow-up versus >10 years of follow-up. We also stratified studies by method of detection. “Older detection” refers to studies that used WBS and less-sensitive Tg assays, and “newer detection” refers to methods such as highly sensitive ultrasound and Tg assays as means of detecting recurrence of thyroid cancer.
Data synthesis and analysis
Because of the variety of different staging systems and definitions of stage and risk, for this analysis, studies were grouped based on an assigned grade to provide better and more accurate comparisons. Low-risk and high-risk patients are often grouped together in the statistical analysis, and patient demographic and tumor characteristics are not consistent from study to study; therefore, we have attempted from these articles to stratify subjects into two risk groups—lower risk and higher risk—to make conclusions regarding survival/mortality. These risk categories refer to both risk of recurrence and death from DTC. In general, low risk for recurrence and death include those patients with smaller tumors, no local or regional invasion, or distant metastases, whereas high risk refers to those patients with larger tumors (>4 cm), local and regional invasion, and/or distant metastases. Figure 1 outlines the process of categorization and provides a description of the groupings.
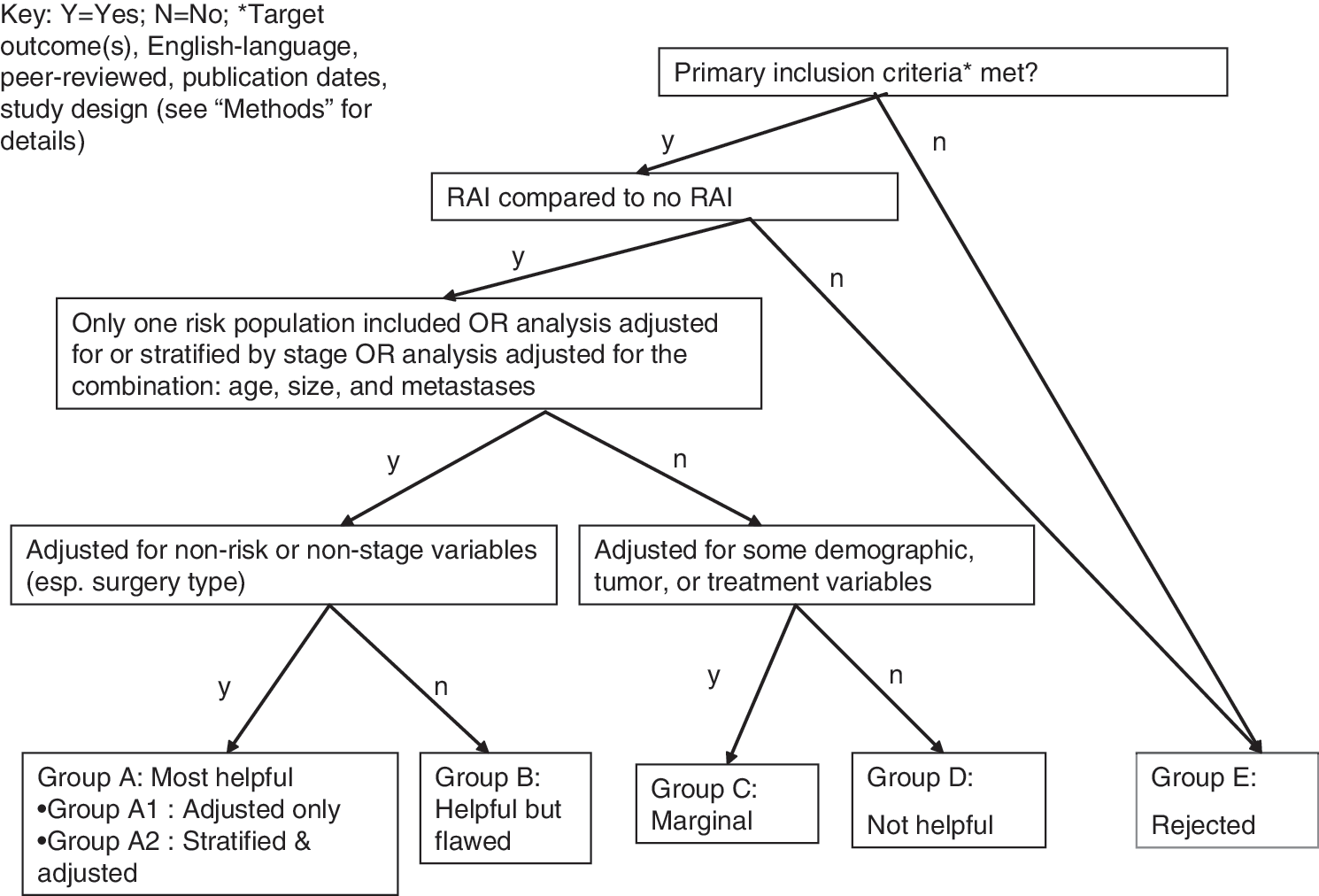
Assigned groupings of articles included in the review. y, yes; n, no. *Target outcomes(s), English language, peer reviewed, publication dates, study design.
Group A through E studies provided results for radioiodine versus no radioiodine, but differed in their methodological rigor as listed below in descending order of best to least: Group A A1 studies analyzed only one stage/risk group and further adjusted for other variables. A2 studies used multivariable model(s) and included variables that are proxy for stage/risk (age, tumor size, and metastasis) as well as other variables. Group B Studies included only one stage/risk group or included variables that contribute to stage/risk, but did not adjust for other variables. Group C Studies adjusted for some demographic, tumor, and treatment variables, but did not explicitly list stage/risk, or age, tumor size, and metastasis in a multivariable model. Group D Studies provided unadjusted comparisons only and were not very helpful. Group E Studies were rejected because they did not directly compare outcomes for patients who received RAI to those who did not.
Our review focuses on results from group A studies since these articles provide us with the most rigorous data.
Results
Survival
The majority of studies, including those that adjusted for disease stage/risk, found that RAI is not associated with a statistically significant improvement in mortality or disease-specific survival.
When adjusted for stage or risk, and other demographic, tumor, or treatment variables, four studies found a statistically significant relationship between RAI treatment and mortality/survival (14,18 –20). In a study of patients with papillary thyroid carcinoma (PTC) or FTC with primary tumor >1.5 cm, no extracapsular invasion, and no distant metastasis at the time of diagnosis treated in the U.S. Air Force or Ohio State University, the cumulative 30-year mortality was lower for patients receiving RAI as compared with no postoperative medical therapy or thyroid hormone alone (adjusted hazards ratio [AHR] 0.5, 95% CI 0.4–0.7, p = 0.001) (21), and a subsequent study on the same cohort also demonstrated a decrease in mortality after RAI treatment (AHR 0.5, 95% CI 0.4–0.7, p = 0.001) (18). Cunningham et al. found that RAI is associated with improved survival after adjusting for demographic variables and disease stage (adjusted relative odds 1.54, 95% CI 1.01–2.35) (20). In patients with high-risk PTC, Lo et al. found that a lack of treatment with RAI is associated with increased mortality (AHR 2.7, 95% CI 1.3–5.7, p = 0.009; demographic variables were considered for the model, but were not statistically significant in bivariable analyses) (19). In a study of patients with FTC using Surveillance Epidemiology and End Results (SEER) data, Podnos et al. found that RAI treatment was associated with improved overall survival (adjusted risk ratio [ARR] 1.24, 95% CI 1.03–1.51, p = 0.26) (14).
Thirteen retrospective cohort studies did not find a statistically significant relationship between RAI treatment and mortality/survival (22 –34). Sanders and Cady did not find significantly improved survival for low-risk or high-risk patients, but type and extent of surgery were not mentioned (23). Low-risk patients included women age 50 or younger, men age 40 or younger without distant metastases, older patients with tumors ≤5 cm with no extrathyroidal invasion, or FTC without capsular or vascular invasion. Loh et al. reports no reduction in cause-specific mortality in PTC and FTC patients with tumors more advanced than T1N0M0 after RAI (ARR 1.1, 95% CI 0.5–2.3, p = 0.76) (25). This is a similar conclusion to that of Tsang, who reported no reduction in cause-specific mortality in patients with stages I–IV DTC using the IUCC staging system (35) treated with near-total or total thyroidectomy and postoperative RAI (ARR 0.7, 95% CI 0.4–1.4, P0.34) (27) and to that of single institution study of Brierley et al., in which RAI treatment is not associated with improved cause-specific survival (CSS) after adjusting for stage (33). Patients with DTC from the New Mexico Tumor Registry (28) did not show reduced overall mortality (AHR 0.96, 95% CI 0.61–1.54, p = 0.88) with RAI treatment after adjusting for disease stage and patient and tumor characteristics. Saadi et al. (34) also found no association with RAI treatment and improved cumulative 10- and 15-year survival for patients with well-differentiated FTC after adjusting for demographic and tumor variables.
Three studies looking at patients with only PTC subtype also found no significant mortality benefit after RAI treatment (22,24,26). Podnos et al. performed propensity-adjusted comparisons of RAI versus no RAI treatment and found that RAI was not associated with improved survival for both lower-risk or higher-risk groups (p = 0.8 lowest risk; p = 0.2 highest risk) (22). In a single-institution study, Pelizzo et al. found that neither lower-risk patients with microcarcinoma (PTC ≤1 cm) nor those with tumors over 1 cm had improved survival (p-value not stated) with RAI treatment (24). DeGroot et al. found no mortality benefit (p-value not stated) for the lower-risk patients with PTC in their study group (26). A later study from the same institution demonstrated no reduction in cause-specific mortality (p = 0.882) of patients with FTC treated with postoperative RAI (29).
Four group A1 articles (6,13,36,37) and three group A2 articles (38 –40) report mixed statistical results mostly due to differences in patient risk categorization or stage. Data from the National Thyroid Cancer Treatment Cooperative Study Group (NTCTCSG) registry were analyzed using two statistical approaches: propensity analysis for stage I patients and multivariable proportional hazards model for stage I, stage II, and stage III/IV (6). RAI was not associated with improved disease-free survival for stage I patients after propensity analysis. RAI treatment for stage III or IV patients improved overall, disease-specific, and disease-free survival (p = 0.0049, 0.0045, and 0.035, respectively). Patients over age 45 with stage II disease in the NTCTCSG registry also benefited from postoperative RAI, but the NTCTCSG stage II patients are stage III by the AJCC staging system. Data from the NTCTCSG published by Taylor et al. (36) demonstrated that RAI is associated with improved overall mortality (p < 0.001) for high risk, non-Hurthle-cell FTC patients, and cancer-specific mortality in both FTC and PTC subjects. Another study demonstrating mixed results includes Kuijpens et al. (38), whose data originates from the Eindhoven Cancer Registry/Comprehensive Cancer Centre South. Patients with DTC treated with RAI had decreased crude mortality for up to and including 5 years; however, after 5 years, the advantage was no longer present (38). Further, Jung et al. found that high-dose RAI treatment is not associated with improved survival in analyses that include only patients with poorly DTC; however, in adjusted analyses that include both poorly DTC and aggressive variant PTC, high-dose RAI treatment is associated with improved survival (39). A single-institution study by Yildirim found that RAI treatment decreased mortality and improved overall 10-year survival in all but the very low-risk patients (40). Chow et al. found that 10-year CSS was improved with RAI treatment for PTC (p = 0.001), but in subgroup analysis of lower-risk patients without distant metastasis or postoperative residual locoregional disease, RAI was not associated with improved 10-year CSS (p = nonspecific [NS]) (13). A subsequent study by the same author found similar results for patients with FTC. In their subgroup analysis of higher-risk patients with distant metastasis, RAI was associated with reduction in mortality, but lower-risk patients did not demonstrate an improvement in CSS (37).
One group B retrospective study reported a statistically significant relationship (20), and 5 group B retrospective cohort studies reported no statistically significant relationship between RAI treatment and mortality/survival (27,41 –44). Three group B articles reported mixed statistical results (33,40,45).
From the partially adjusted group C articles, two studies reported a statistically significant relationship between RAI treatment and mortality/survival (46,47) and three articles reported no statistically significant relationship (48 –50). Five group D articles (51 –55) reported a statistically significant relationship between RAI treatment and mortality/survival and six articles found no significant relationship (56 –61). One group D article reported mixed results (62).
In summary, of the group A studies, a majority did not find an overall or CSS benefit to postoperative RAI ablation especially in subgroup analysis of lower-risk patients such as those without distant metastasis or extrathyroidal extension, but including those with lymph node metastasis. This grouping would be consistent with AJCC TNM stage I or stage II over 45 years. On the other hand, analyses of higher-risk patients with DTC, equivalent to AJCC TNM stage III/IV and stage II under age 45, did show a survival benefit with use of RAI treatment.
Recurrence
The evidence for using postoperative RAI to decrease thyroid cancer recurrence is mixed. Approximately half of the studies show a statistically significant relationship between RAI ablation and decreased recurrence, and the other half do not.
Subgroup analyses were performed to evaluate whether the recurrence data were confounded by both duration of follow-up and by method of detection of recurrence. Of a total of 14 studies, 1/7 showed significance (63) in the <10 year duration of follow-up (13,24,63 –67) and 5/7 (18,25,27,33,37) demonstrated significance in the >10 year duration of follow-up (18,25,26,27,29,33,37), but, overall, the duration of follow-up did not have a statistically significant impact on detection of recurrence rates (p = 0.1). There was a trend toward significance as we would have expected, but we did not have enough studies to demonstrate significance. To assess whether method of detection impacts recurrence rates, 13 studies were grouped into “older detection” or those studies that used WBS alone or WBS in addition to Tg (WBS+Tg) (18,25,26,27,29,63,67), versus “newer detection” or those studies using Tg or Tg+other, such as highly sensitive ultrasound (13,33,37,64,66). There was not a statistically significant difference between the method of detection when the studies were grouped in this way (p = 0.76). In summary, based on the small numbers of studies, duration of follow-up and method of detection did not confound our original analysis.
After adjusting for stage/risk and other demographic, tumor, and treatment variables, six group A articles found a statistically significant relationship between RAI treatment and recurrence (18,25,27,33,37,63). From the NTCTCSG data, the only nonrandomized prospective cohort study, Cooper et al. (63) found that RAI is a significant predictor of disease progression for PTC patients (p = 0.01), after adjusting for disease stage, mean thyrotropin score category, and other variables. However, in subgroup analyses, Cooper et al. found that for low-risk (stage I and II) patients, RAI is not a significant predictor of disease progression, whereas for high-risk (stage III and IV) patients, RAI is a significant predictor of disease progression (p < 0.001), after adjusting for mean thyrotropin score category. In contrast, a large study of lower-risk patients with PTC and FTC (tumors >1.5 cm, without extrathyroidal extension or distant metastasis) treated in the U.S. Air Force or Ohio State University hospitals demonstrated cumulative lower recurrence rates for those who received RAI as compared with those who did not receive RAI (AHR 0.87, 95% CI 0.8–0.9, p = 0.001) (19). Mazzaferri and Kloos report that therapy with RAI is associated with a decrease in all cancer recurrence (AHR 0.8, 95% CI 0.7–0.97, p = 0.016) and distant metastasis recurrence (AHR 0.6, 95% CI 0.5–0.8, p = 0.002) after adjusting for demographic, tumor, and treatment variables (18).
Three single-institution studies of higher-risk patients with mixed histological subtypes of tumors all demonstrated a decrease in recurrence associated with RAI treatment (21,23,25). Loh et al. found that a lack of adjuvant therapy was associated with increased cancer recurrence as compared with adjuvant therapy with RAI (ARR 2.1, 95% CI 1.5–3.1, p = 0.0001) (25), Tsang et al. found that RAI is associated with a decrease in local recurrence (ARR 0.4, 95% CI 0.2–0.7, p = 0.002) after adjusting for demographic and tumor variables (27), and Brierley et al. showed that RAI was associated with improved freedom from recurrence after adjusting for demographic, tumor, and treatment variables and stratifying by time period (AHR 0.5, 95% CI 0.3–0.8, p = 0.007) (33). Chow et al. reported that patients with FTC treated with RAI had improved 10-year locoregional control after adjustments were made for demographic, tumor, and treatment variables (ARR 0.13, 95% CI 0.05–0.35, p < 0.001) (37).
Seven group A retrospective cohort studies of lower-risk patients did not find a statistically significant relationship between RAI treatment and recurrence (22,24,26,29,64 –66). A single-institution study by Baudin et al. found that postoperative RAI treatment for lower-risk patients with papillary or follicular microcarcinoma was not associated with decreased recurrence (p-value not stated), after adjusting for demographic, tumor, and treatment variables (67). Palme et al. found that RAI treatment did not significantly predict development of more than one recurrence in patients with DTC after adjusting for demographic, disease stage, tumor, treatment, and first recurrence (66). Pelizzo et al. studied lower-risk patients with papillary thyroid microcarcinoma and found that RAI treatment is not associated with a decrease in recurrence (p = NS) after adjusting for demographic, tumor, and treatment variables. In patients with tumors over 5 mm in size, there was no statistically significant difference in recurrence with the combination of near-total thyroidectomy plus RAI as compared with thyroidectomy alone (p = NS) (24). DeGroot et al. also found a nonsignificant association with use of RAI treatment for lower-risk patients and decreased recurrence overall or for any of the PTC subgroups analyzed in a multivariable model that adjusted for demographic, disease class, tumor, and treatment variables (26). In two studies of patients with FTC, patients treated with RAI did not demonstrate decreased recurrence after adjusting for demographic, tumor, and treatment variables (29,64).
One retrospective study from group A demonstrated mixed statistical results; RAI treatment was associated with improved locoregional recurrence or uncontrolled disease (ARR 0.39, 95% CI 0.27–0.56, p < 0.001) for the entire cohort, but was not associated with improvement in freedom from distant metastasis for the entire cohort (p = NS). Patients with lower-risk disease who received RAI in an adjuvant setting (no distant metastasis and no residual gross locoregional disease) had improved locoregional and distant relapse (ARR 0.29, 95% CI 0.17–0.51, p < 0.01) and decreased distant recurrence (ARR 0.2, 95% CI 0.07–0.64) (11). Of the TNM stage I patients, Chow et al. also report that RAI treatment is associated with improved 10-year locoregional control (p = 0.15) (13).
Of the group B articles, one nonrandomized prospective study using data from the NTCTCSR found reduced risk of progression of disease after RAI treatment (ARR 0.30, 95% CI 0.13–0.72, p = 0.01; ARR 0.30, 95% CI 0.12–0.77) for high-risk PTC and FTC patients (34). One article from group B demonstrated no significant relationship between RAI treatment and recurrence (44), and three articles showed mixed statistical results (34,41,52).
Two group C articles, both retrospective studies, found a statistically significant relationship between RAI and recurrence (68,69), and one article, a meta-analysis of nonrandomized studies, showed mixed results (70). From group D articles, two demonstrated significance (59,71), two demonstrated no significance (61,72), and three reported mixed statistical results (73,74) when evaluating the relationship between RAI treatment and recurrence.
In summary, the many studies sited above demonstrate mixed results when looking at whether the use of RAI can prevent recurrence of thyroid cancer. While results seem to favor a significant relationship between RAI and recurrence in all groups, the majority of low-risk patient groups did not show significantly improved recurrence rates. High-risk patient groups did have improved recurrence rates after treatment with RAI.
Discussion
This review was conducted to identify and synthesize the evidence for using RAI for treatment of thyroid carcinoma. Of particular interest is whether and how clinical outcomes may vary based on disease stage. After searching the peer-reviewed literature, we found 79 studies published since 1966 that compared treatment versus no treatment with RAI for thyroid cancer. None of the studies used a randomized controlled trial design; overwhelmingly, the design of choice was a retrospective cohort design. Many studies used statistical methods to account for confounders, one of the main threats to validity of nonrandomized prospective and retrospective studies. Some studies used multi-institutional samples, including cancer registries to minimize issues related to selection bias, which may be more pronounced in single-institutional samples (6,14,18,20,22,28,36,63,75). A majority of studies concluded that the use of RAI did not improve mortality/survival for DTC, even after adjusting for stage/risk variables. However, roughly half of the studies looking at disease-free survival support the use of RAI to reduce recurrence after adjusting for stage/risk variables.
The recent ATA guidelines recommend considering postoperative RAI treatment for all but the very low-risk individuals with unifocal or multifocal microcarcinoma thyroid cancer confined to the thyroid. The large number of studies in our review demonstrates no significant effect of RAI on mortality or survival for patients defined as being low risk. This body of literature includes several large, multi-institutional, or registry-based studies (6,14,18,28,36). Most of the higher quality studies adjusted for stage/risk by including stage/risk (or variables that contribute to stage/risk) in a multivariable model rather than stratifying by stage/risk. Of the studies that stratified by high-risk or advanced stage, the number of studies reporting a significant effect is higher than the number of studies reporting no significant effect. Overall, however, a larger number of studies found that RAI does not improve mortality or survival, even when stage/risk and other variables are considered.
The mixed statistical results regarding the effects of RAI treatment on recurrence are more consistent with the commentaries on the topic, which generally describe controversy over the use of RAI. Of the studies that stratified by low-risk or less advanced stage, more studies reported that RAI is not associated with reduced recurrence. Overall, however, approximately half of the studies reported significant effects. Regardless of level of adjustment (i.e., group A, B, C, or D), the number of articles presenting statistically significant results is roughly the same as the number of articles presenting nonsignificant results. A systematic review examining the effects of RAI remnant ablation on the risk of thyroid cancer-related mortality and disease recurrence in early stage DTC published by Sawka et al. also found a lack of benefit of RAI remnant ablation in decreasing cause-specific mortality or recurrence for this low-risk group. However, remnant ablation was associated with a decrease in risk of distant metastatic recurrence with a risk difference of −2% (p = 0.005) (72).
On the basis of our literature review, we have created a set of practice guidelines (see Table 1) for use in our institution for postoperative RAI for remnant ablation or adjuvant therapy in patients with DTC. We categorized patients by age and risk group (very low, low, moderate, and high risk) based on the AJCC TNM staging for thyroid cancer as well as MACIS score. These two staging systems have demonstrated consistent and similar survival and recurrence results based on stage and score (12,76).
Corresponding stages based on AJCC TNM and MACIS (20 year cause specific survival rate: if MACIS <6, 99%; 6–6.00, 89%; 7–7.99, 56%; >8, 24%).
RAI, radioactive iodine; MACIS, metastases, age, completeness of resection, invasion, size; LN, lymph node.
Age 45 years or less
We consider patients 45 years and younger to be very low risk if they have unilateral or multicentric microcarcinoma or a well-differentiated tumor confined to the thyroid with no lymph node involvement (MACIS < 6; TNM stage I; T0–T2, N0, M0) similar to the low risk defined by the European Task Force (5). Low risk in this age group includes those patients with tumors <4 cm in size and central compartment (level VI) lymph node involvement (MACIS < 6; TNM stage I; T0–T2, N0–N1a, M0). Unlike the current ATA and European guidelines (4,5), which recommend RAI in select cases of low-risk patients, based on our literature review, we do not find a survival benefit or recurrence benefit to using RAI ablation for this group and, therefore, do not recommend it. Moderate-risk patients in this age category include those with more aggressive tumor characteristics but for whom the evidence is unclear whether there is either a survival or recurrence benefit to postsurgical RAI treatment. This group includes patients with tumors >4 cm, tumors with a more aggressive histologic subtype (insular, sclerosing, and tall cell variants), minimal extrathyroidal extension, as well as minimally invasive follicular carcinoma. We also include in this moderate-risk group patients with macroscopic central lymph nodes as well as lateral lymph node involvement on initial presentation. While several studies have found nodal metastasis to have no overall prognostic significance in young patients (77,78), the presence of lateral nodal disease at the time of initial surgery may indicate more aggressive disease and may impact locoregional recurrence. Therefore, we suggest that clinical judgment be used for selective use of RAI for remnant ablation in these TNM stage I patients. High-risk patients in this age category include those with distant metastasis (TNM stage II disease or MACIS > 6) and those with extrathyroidal invasion of tumor into muscle, subcutaneous tissue, larynx, trachea, esophagus, or recurrent laryngeal nerve, and as the evidence suggests, RAI remnant ablation is beneficial for these patients.
Age greater than 45 years
For very low-risk and low-risk patients over age 45 (stage I/II, MACIS < 6), which include those with microcarcinomas and tumors <4 cm with no lymph node involvement, we do not recommend I-131 remnant ablation. For select patients, this recommendation differs from the current ATA and European guidelines. Moderate-risk patients in this age group include those with more aggressive histologic variants of PTC or minimally invasive follicular carcinoma. Clinical judgment of the physician should be used to determine use of RAI ablation for this group. Patients over 45 years of age with lymph node involvement, extrathyroidal extension, distant metastasis, or widely invasive follicular carcinomas make up the high-risk category (TNM stage III/IV, MACIS > 6). We recommend postoperative RAI for patients in the high-risk group because of the benefit seen in CSS. The ATA and European guidelines also recommend treating this group (4,5).
As multiple thyroid carcinoma experts have observed, the lack of randomized controlled trials and the preponderance of studies that use retrospective study designs makes this literature challenging; therefore, our analysis should be interpreted with caution. The RAI–clinical outcome relationship is particularly difficult to discern when retrospective study designs are employed because of the tendency to offer and treat higher-risk patients more aggressively. In the absence of randomized controlled trials, several authors have used statistical methods to correct for confounding. By assigning grades to each article, we have attempted to place more emphasis on studies that used statistical approaches to address confounding, and by comparing articles within the same grading stratum, our results may have more validity. Some articles used conventional multivariable regression methods, whereas others have used propensity score methods (two authors used both methods) (6,22). As noted in our methods section, we grouped these articles similarly based upon the results of two systematic reviews that find no empirical evidence that one method is superior to the other for addressing confounding (79,80).
Another reason for interpreting these results with caution is the variability in quality of presentation of results. Although we did not explicitly assess the quality of presentation of the studies, we found that some authors more carefully documented their methods and more clearly conveyed the variables in their final statistical model than others.
Finally, the absence of an explicit conceptual model in the literature to guide and ground the analyses is notable. Many of the articles identified for this review used semi-automated statistical processes to build the multivariable model, which could affect the results of this review. Future conceptual and statistical models and data collection efforts should also consider the effects of provider-level and system-level variables such as provider experience and high surgical volume, which are known to be associated with better clinical outcomes, including mortality (81 –84).
Conclusions
On the basis of this systematic analysis of the peer-reviewed literature, we conclude that the preponderance of evidence suggests that RAI treatment is not associated with improved survival in patients with low-stage or low-risk DTC. The data concerning recurrence rates following RAI treatment in this group of patients are less conclusive. The lack of randomized controlled trials and the variability in the quality of studies deserve attention, and results should be interpreted with caution. A controlled multicenter prospective trial looking at the effect of RAI on recurrence and mortality is needed to mitigate the factors limiting our current results.
Footnotes
Disclaimer
The views expressed in this article are those of the authors and do not necessarily represent the views of Zynx Health, Inc.
Disclosure Statement
J.T.C. is an employee of Zynx Health Incorporated. The remaining authors declare that no competing financial interests exist.
Appendix
| Search | Search strings | No. of articles |
|---|---|---|
| #6 | Search #5 NOT (Bibliography[pt] OR Comment[pt] OR Historical Article [pt] OR Interview[pt] OR Letter[pt] OR Newspaper Article[pt]) | 2697 |
| #5 | Search #4 Limits: Entrez Date from 1966 to 2008, Publication Date from 1966 to 2008, Humans, English | 2887 |
| #4 | Search #3 Limits: Entrez Date from 1966 to 2008, Publication Date from 1966 to 2008, Humans | 3789 |
| #3 | Search #1 AND #2 | 4140 |
| #2 | Search Radioactive iodine remnant ablation OR Iodine radioisotopes OR Iodine radioisotopes/*therapeutic use OR Radiotherapy, adjuvant OR Iodine-131 OR* IODINE/radioactive | 59082 |
| #1 | Search Thyroid neoplasms OR Papillary thyroid carcinoma OR Carcinoma, Papillary OR Follicular thyroid carcinoma OR Adenocarcinoma, Follicular OR Thyroid Neoplasms/mortality/pathology/radiotherapy/surgery/*therapy OR Neoplasm, Residual/*radiotherapy/surgery OR THYROID GLAND, neoplasms | 38122 |
The asterisk (*) represents a wildcard character as part of PubMed searching syntax. It does not represent a significant value.